Das könnte Ihnen auch gefallen
- Common Pediatric Cases in OpdDokument90 SeitenCommon Pediatric Cases in OpdJamie Sebastian100% (3)
- 2016COMSSATDokument33 Seiten2016COMSSATDiana AlShrah100% (4)
- Principles of Post Operative Care..Dokument21 SeitenPrinciples of Post Operative Care..Namra MazharNoch keine Bewertungen
- Emergency Department Handbook PDFDokument461 SeitenEmergency Department Handbook PDFdmallozziNoch keine Bewertungen
- Emt Skill SheetsDokument39 SeitenEmt Skill SheetsPatriciaChRistiani100% (1)
- 23 Mock CodesDokument56 Seiten23 Mock Codesmaguisssa100% (4)
- Initial Evaluation Reveals Moderate ComplexityDokument3 SeitenInitial Evaluation Reveals Moderate ComplexitykhushmitNoch keine Bewertungen
- Anemia Concept Mapping. Group 1Dokument82 SeitenAnemia Concept Mapping. Group 1Giselle EstoquiaNoch keine Bewertungen
- Emergency Department Triage ProcessDokument27 SeitenEmergency Department Triage ProcessJerry AbleNoch keine Bewertungen
- Trauma OverviewDokument48 SeitenTrauma OverviewFrancescoBarbero100% (1)
- Triage in Emergency DepartmentDokument25 SeitenTriage in Emergency DepartmentLourdelina Techap100% (1)
- Min Min Min Min: Most Urgent Very Urgent Urgent Less Urgent Not UrgentDokument1 SeiteMin Min Min Min: Most Urgent Very Urgent Urgent Less Urgent Not UrgentAlma Alnajjar0% (1)
- Sree Vasantham Hospital, Salem: 1. Er Protocol For Acute Intoxication (Poisoning)Dokument7 SeitenSree Vasantham Hospital, Salem: 1. Er Protocol For Acute Intoxication (Poisoning)Elango MuthuNoch keine Bewertungen
- The Triage ProcessDokument3 SeitenThe Triage ProcessepingNoch keine Bewertungen
- Acute Respiratory Distress: Section I: Scenario DemographicsDokument6 SeitenAcute Respiratory Distress: Section I: Scenario DemographicsharasthaNoch keine Bewertungen
- Diagnosis and Treatment of Intraabdominal InjuriesDokument88 SeitenDiagnosis and Treatment of Intraabdominal Injuriessgod34Noch keine Bewertungen
- Nursing Care Plans for Febrile Seizures in ChildrenDokument16 SeitenNursing Care Plans for Febrile Seizures in ChildrenRedgina CalimlimNoch keine Bewertungen
- A&E Triage SystemDokument5 SeitenA&E Triage SystemArnel AlmutiahNoch keine Bewertungen
- Thoracic Trauma - Navy - PSPD 2021Dokument45 SeitenThoracic Trauma - Navy - PSPD 2021Naavy LaksmonoNoch keine Bewertungen
- Early Emergency Care ProceduresDokument53 SeitenEarly Emergency Care ProceduresDwi ayu oktaveni100% (1)
- Nursing Care of Clients in Emergency Situation 2Dokument52 SeitenNursing Care of Clients in Emergency Situation 2Danica FrancoNoch keine Bewertungen
- Taking Anthropometric MeasureDokument1 SeiteTaking Anthropometric MeasureAdee FerrandoNoch keine Bewertungen
- BASIC LIFE SUPPORT: ESSENTIAL CONCEPTS AND PROCEDURESDokument8 SeitenBASIC LIFE SUPPORT: ESSENTIAL CONCEPTS AND PROCEDURESHynne Jhea EchavezNoch keine Bewertungen
- Bls Dewasa PKDJB 2022Dokument74 SeitenBls Dewasa PKDJB 2022Halawatul ImanNoch keine Bewertungen
- Blood Transfusion Single Use PathwayDokument6 SeitenBlood Transfusion Single Use PathwayropusanNoch keine Bewertungen
- Anaphylaxis With Angioedema: Section I: Scenario DemographicsDokument7 SeitenAnaphylaxis With Angioedema: Section I: Scenario DemographicsharasthaNoch keine Bewertungen
- AbbreviationDokument19 SeitenAbbreviationJayson NatividadNoch keine Bewertungen
- Initial Assessment and Management of Trauma PatientsDokument8 SeitenInitial Assessment and Management of Trauma PatientsAlvin De LunaNoch keine Bewertungen
- Saudi CPR Guidlines in EnglishDokument16 SeitenSaudi CPR Guidlines in EnglishpiyushbamsNoch keine Bewertungen
- Vitals Pocket ChartDokument4 SeitenVitals Pocket ChartAli MullaNoch keine Bewertungen
- Managing The Deteriorating PatientDokument14 SeitenManaging The Deteriorating PatientArie PurwantoNoch keine Bewertungen
- Initial Assessment and Management: Presented by Fayez Abillama, MDDokument53 SeitenInitial Assessment and Management: Presented by Fayez Abillama, MDDaniel GhosseinNoch keine Bewertungen
- RSI For Nurses ICUDokument107 SeitenRSI For Nurses ICUAshraf HusseinNoch keine Bewertungen
- Modified Early Obstetric Warning Score MEOWS MID33 AO13 v4.2Dokument9 SeitenModified Early Obstetric Warning Score MEOWS MID33 AO13 v4.2indirinoor5Noch keine Bewertungen
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsVon EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNoch keine Bewertungen
- Needle Thoracentesis GuideDokument30 SeitenNeedle Thoracentesis GuideAlvin BernardNoch keine Bewertungen
- Student Refresher CourseDokument87 SeitenStudent Refresher CourseRaisa S. MariscalNoch keine Bewertungen
- CURRENT MEDICAL TREATMENT ON BPHDokument33 SeitenCURRENT MEDICAL TREATMENT ON BPHDeviruchi GamingNoch keine Bewertungen
- Nursing Care for Chest TraumaDokument100 SeitenNursing Care for Chest TraumaGabriel Liberon P. JazonNoch keine Bewertungen
- Ed Assessment Tool SampleDokument28 SeitenEd Assessment Tool SampleAnonymous ibmeej9Noch keine Bewertungen
- Advanced Airway Management: Leaugeay Webre, BS, CCEMT-P, Nremt-PDokument35 SeitenAdvanced Airway Management: Leaugeay Webre, BS, CCEMT-P, Nremt-Pbasic100% (4)
- Operating Room Nurse Interview QuestionsDokument2 SeitenOperating Room Nurse Interview Questionsali aliNoch keine Bewertungen
- PRE ANAESTHETIC ASSESSMENT New 1Dokument41 SeitenPRE ANAESTHETIC ASSESSMENT New 1lokeswara reddyNoch keine Bewertungen
- A3 - ABCDE Algorithms PDFDokument63 SeitenA3 - ABCDE Algorithms PDFteguhNoch keine Bewertungen
- NTILS GuideDokument11 SeitenNTILS GuideNeil ThomasNoch keine Bewertungen
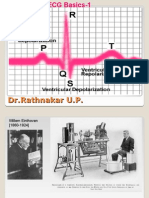
- ECG Basics 1Dokument24 SeitenECG Basics 1Dr.U.P.Rathnakar.MD.DIH.PGDHMNoch keine Bewertungen
- Intensive Care UnitDokument12 SeitenIntensive Care UnitAnt OnNoch keine Bewertungen
- Basic Life SupportDokument5 SeitenBasic Life SupportbuenoevelynNoch keine Bewertungen
- TriageDokument42 SeitenTriageNic JiNoch keine Bewertungen
- Emergency NursingDokument46 SeitenEmergency NursingJoshua P AloveroNoch keine Bewertungen
- CPR - Cardiopulmonary ResuscitationDokument31 SeitenCPR - Cardiopulmonary ResuscitationPanji HerlambangNoch keine Bewertungen
- Basic Life SupportDokument34 SeitenBasic Life SupportEveline FebrinaNoch keine Bewertungen
- Malaysiantriagescalenewrevised2019!1!221014090642 28d8e1aeDokument18 SeitenMalaysiantriagescalenewrevised2019!1!221014090642 28d8e1aenaqibsakila4286Noch keine Bewertungen
- DVT Assessment FormDokument1 SeiteDVT Assessment FormLoy ZiNoch keine Bewertungen
- Emergency Trauma CareDokument49 SeitenEmergency Trauma Careandrei neagNoch keine Bewertungen
- Emergency Rooms (ER) : Presented By: AdamDokument6 SeitenEmergency Rooms (ER) : Presented By: AdamSulemanNoch keine Bewertungen
- Potential Post Operative ComplicationsDokument18 SeitenPotential Post Operative ComplicationsethelnmundaNoch keine Bewertungen
- Blood Transfusion ReactionDokument9 SeitenBlood Transfusion ReactionReema Akberali nooraniNoch keine Bewertungen
- Adult CPR flow chartDokument1 SeiteAdult CPR flow chartLia IshakNoch keine Bewertungen
- CPR Exam TheoryDokument10 SeitenCPR Exam TheorysahirbuleNoch keine Bewertungen
- Accident and Emergency DepartmentDokument9 SeitenAccident and Emergency Departmentshah007zaadNoch keine Bewertungen
- Acute Respiratory FailureDokument29 SeitenAcute Respiratory FailurePIYALI BISWASNoch keine Bewertungen
- ICU Scoring Systems A Complete Guide - 2020 EditionVon EverandICU Scoring Systems A Complete Guide - 2020 EditionNoch keine Bewertungen
- Chest PhysioDokument44 SeitenChest PhysioagungNoch keine Bewertungen
- Patient Transfer SheetDokument3 SeitenPatient Transfer SheetagungNoch keine Bewertungen
- TRIAGEDokument59 SeitenTRIAGEagungNoch keine Bewertungen
- Marissa Lamanna March 2013Dokument44 SeitenMarissa Lamanna March 2013agung100% (1)
- GINA Pocket 2015Dokument32 SeitenGINA Pocket 2015Ramzi AkramNoch keine Bewertungen
- Emergenci NursingDokument2 SeitenEmergenci NursingagungNoch keine Bewertungen
- Nursing Trauma PDFDokument2 SeitenNursing Trauma PDFagungNoch keine Bewertungen
- Medical Evacuation On TraumaDokument102 SeitenMedical Evacuation On Traumaagung100% (1)
- Spanish Pediatric Immunisation Reccommendation 2012Dokument23 SeitenSpanish Pediatric Immunisation Reccommendation 2012agungNoch keine Bewertungen
- DM 2Dokument85 SeitenDM 2agungNoch keine Bewertungen
- Malnutrition Screening Tool - FINALDokument1 SeiteMalnutrition Screening Tool - FINALagungNoch keine Bewertungen
- Nursing TraumaDokument2 SeitenNursing TraumaagungNoch keine Bewertungen
- Medical Evacuation On TraumaDokument102 SeitenMedical Evacuation On Traumaagung100% (1)
- Patient - Safety and IT TrendsDokument3 SeitenPatient - Safety and IT TrendsagungNoch keine Bewertungen
- Triage PDFDokument59 SeitenTriage PDFagungNoch keine Bewertungen
- GINA Pocket 2015Dokument32 SeitenGINA Pocket 2015Ramzi AkramNoch keine Bewertungen
- Medical Evacuation On TraumaDokument102 SeitenMedical Evacuation On Traumaagung100% (1)
- Triage PDFDokument59 SeitenTriage PDFagungNoch keine Bewertungen
- Hand Hygiene Why How and When BrochureDokument7 SeitenHand Hygiene Why How and When BrochureLeis FatwaNoch keine Bewertungen
- Manuskrip Bu Siwi PDFDokument18 SeitenManuskrip Bu Siwi PDFagungNoch keine Bewertungen
- Manuskrip Bu Siwi PDFDokument18 SeitenManuskrip Bu Siwi PDFagungNoch keine Bewertungen
- Fire Panel ZonesDokument2 SeitenFire Panel ZonesagungNoch keine Bewertungen
- ChatGPT AI For Medicine NEJM Mar 23Dokument7 SeitenChatGPT AI For Medicine NEJM Mar 23Julio CidNoch keine Bewertungen
- Quiz 21 - Pediatrics RECORTADA (Hoja Alumno)Dokument2 SeitenQuiz 21 - Pediatrics RECORTADA (Hoja Alumno)Cynthia Argüelles GuzmánNoch keine Bewertungen
- CARDIODokument10 SeitenCARDIOkristineNoch keine Bewertungen
- Aluminum Safety Data Sheet SummaryDokument6 SeitenAluminum Safety Data Sheet SummarySaul MontielNoch keine Bewertungen
- Occupational Therapy Interventions-MorganDokument6 SeitenOccupational Therapy Interventions-MorganJulieta CastellanoNoch keine Bewertungen
- Cardiogenic Shock and Pulmonary EdemaDokument41 SeitenCardiogenic Shock and Pulmonary EdemaChristian Gallardo, MD100% (7)
- A Case Investigator's Guide For COVID-19: CDC - Gov/coronavirusDokument27 SeitenA Case Investigator's Guide For COVID-19: CDC - Gov/coronavirusChris-Goldie LorezoNoch keine Bewertungen
- CHF: Congestive Heart Failure Diagnosis, Pathophysiology, and ManagementDokument6 SeitenCHF: Congestive Heart Failure Diagnosis, Pathophysiology, and ManagementSOPHIA LOISE TEJANO FULACHENoch keine Bewertungen
- Focused AssessmentDokument5 SeitenFocused AssessmentPiyali SahaNoch keine Bewertungen
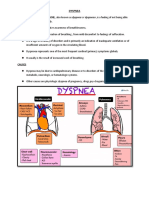
- Dyspnea: CausesDokument7 SeitenDyspnea: CausesGetom NgukirNoch keine Bewertungen
- Cee Based Model Exam Bhadra 30, 2080, Saturday Page 1 of 10Dokument6 SeitenCee Based Model Exam Bhadra 30, 2080, Saturday Page 1 of 10Kailash KhatriNoch keine Bewertungen
- Safety Data Sheet for Fluorosilicic AcidDokument11 SeitenSafety Data Sheet for Fluorosilicic AcidMohammadreza MalekNoch keine Bewertungen
- Vii. Nursing Care Plan: Secretions in The AirwaysDokument5 SeitenVii. Nursing Care Plan: Secretions in The AirwaysJai - Ho100% (2)
- .Uk-EH1 Exercise Handbook v5Dokument17 Seiten.Uk-EH1 Exercise Handbook v5Shamen DubonNoch keine Bewertungen
- Cap MR DDHDokument32 SeitenCap MR DDHLovelle LopezNoch keine Bewertungen
- Clinical Case Presentation Proforma For Respiratory System: July 2019Dokument6 SeitenClinical Case Presentation Proforma For Respiratory System: July 2019Santhosh VaranNoch keine Bewertungen
- Respiratorycasestudy 1Dokument2 SeitenRespiratorycasestudy 1api-265854240Noch keine Bewertungen
- Mock2 9thmarch CompDokument41 SeitenMock2 9thmarch CompObaidNoch keine Bewertungen
- Clerk Sheet Imed and ObsDokument4 SeitenClerk Sheet Imed and ObsGrace PhiriNoch keine Bewertungen
- Dyspnea - Pulmonary Disorders - MSD Manual Professional EditionDokument11 SeitenDyspnea - Pulmonary Disorders - MSD Manual Professional EditionSalma KarimahNoch keine Bewertungen
- Exercise in PregnancyDokument7 SeitenExercise in PregnancynirchennNoch keine Bewertungen
- Nicola Zammitt, - Alastair O'Brien - Essentials of Kumar & Clark's Clinical Medicine-Elsevier (2017) PDFDokument927 SeitenNicola Zammitt, - Alastair O'Brien - Essentials of Kumar & Clark's Clinical Medicine-Elsevier (2017) PDFJamie Baczewski100% (8)
- Case No. 3Dokument3 SeitenCase No. 3Rialyn PontillasNoch keine Bewertungen
- NRLTL QuizletDokument6 SeitenNRLTL QuizletReniella HidalgoNoch keine Bewertungen
- Cough and Dyspnea Case StudyDokument4 SeitenCough and Dyspnea Case StudyAbigail Balbuena100% (1)
- CBSE Chapter 3 Yoga and Lifestyle DiseasesDokument54 SeitenCBSE Chapter 3 Yoga and Lifestyle DiseasesShagnik BasuNoch keine Bewertungen