Beruflich Dokumente
Kultur Dokumente
1 s2.0 S1470204513705850 Main
Hochgeladen von
TYAOriginaltitel
Copyright
Verfügbare Formate
Dieses Dokument teilen
Dokument teilen oder einbetten
Stufen Sie dieses Dokument als nützlich ein?
Sind diese Inhalte unangemessen?
Dieses Dokument meldenCopyright:
Verfügbare Formate
1 s2.0 S1470204513705850 Main
Hochgeladen von
TYACopyright:
Verfügbare Formate
Review
Clinical use of dendritic cells for cancer therapy
Sbastien Anguille, Evelien L Smits, Eva Lion, Viggo F van Tendeloo, Zwi N Berneman
Since the mid-1990s, dendritic cells have been used in clinical trials as cellular mediators for therapeutic vaccination
of patients with cancer. Dendritic cell-based immunotherapy is safe and can induce antitumour immunity, even in
patients with advanced disease. However, clinical responses have been disappointing, with classic objective tumour
response rates rarely exceeding 15%. Paradoxically, ndings from emerging research indicate that dendritic cell-based
vaccination might improve survival, advocating implementation of alternative endpoints to assess the true clinical
potency of dendritic cell-based vaccination. We review the clinical eectiveness of dendritic cell-based vaccine therapy
in melanoma, prostate cancer, malignant glioma, and renal cell carcinoma, and summarise the most important
lessons from almost two decades of clinical studies of dendritic cell-based immunotherapy in these malignant
disorders. We also address how the specialty is evolving, and which new therapeutic concepts are being translated
into clinical trials to leverage the clinical eectiveness of dendritic cell-based cancer immunotherapy. Specically, we
discuss two main trends: the implementation of the next-generation dendritic cell vaccines that have improved
immunogenicity, and the emerging paradigm of combination of dendritic cell vaccination with other cancer therapies.
Introduction
Safety
2013 marked the 40th anniversary of the discovery by
Cohn and Steinman1 of a new type of immune cell:
dendritic cells. Although our knowledge of their biology
and function is incomplete, evidence shows that
dendritic cells play a crucial part in the induction of
antitumour immunity.2 Immunotherapeutic approaches
involving dendritic cells aim to capitalise on the ability
of the cells to direct cytotoxic T lymphocytes and natural
killer cells to become potent antitumour eectors
capable of eradicating malignant cells (gure).3 The
basic immunological principles that provide a
compelling rationale for use of dendritic cells in
immunotherapy and the dierent ways to prepare these
cells for clinical application have been reviewed
elsewhere,2,4 and are beyond the scope of this Review. In
this Review, we rst aim to examine the most important
lessons gained from almost two decades of clinical
studies of dendritic cell-based immunotherapy,
particularly regarding the actual therapeutic usefulness
of dendritic cells. We then describe how the specialty of
dendritic cell-based immunotherapy is evolving, and
provide an update of new models and approaches that
are being adopted in clinical trials.
Since the rst published clinical trials in the mid1990s, many early-phase clinical trials have been done
across a wide range of tumour types. Dendritic cellbased treatments have been tested most often in
patients with malignant melanoma,5 with more than
1250 patients treated (appendix pp 23), followed by
prostate cancer (>750 patients treated; appendix p 4),
malignant glioma (>500 patients treated; appendix p 5),
and renal cell cancer (>250 patients treated; appendix
p 6). These malignant diseases are the only tumour
types in which phase 3 clinical trials of these treatments
have been done or are underway (table 1). Therefore, in
this Review we focus on these four tumour types, and
use them to summarise the conclusions that can be
gathered about the clinical use of dendritic cells in
cancer immunotherapy.
The safety of dendritic cell-based immunotherapy has
been well documented in many phase 1 clinical studies.6
Local reactions at the injection sites (ie, pain, rash, and
pruritus) are common, but these reactions are generally
mild and self-limiting.6 Systemic side-eects, including
pyrexia, malaise, and other inuenza-like symptoms, can
occur; however, systemic grade 34 (US National Cancer
Institute-Common Terminology Criteria) toxicity is
extremely uncommon when dendritic cell vaccination is
given as monotherapy.6 One particular concern with
immunotherapy is the possibility of induction of
autoimmunity.7 However, cancer vaccine strategies are
rarely associated with severe immune-related toxicity,
which contrasts sharply with other immunotherapeutic
methods such as monoclonal antibodies and cytokines.7
For example, immune-related adverse events have been
reported in up to 60% (of which 15% are grade 34 toxicity)
of patients treated with the anti-cytotoxic T lymphocyte
antigen-4 (CTLA-4) monoclonal antibody ipilimumab,8
which has been approved by US and European health
authorities for the treatment of melanoma.
In line with its low toxicity, dendritic cell-based
immunotherapy is expected to preserve the quality of life
of patients with cancer.9 Quality of life is an important
outcome in assessment of novel anticancer agents,
especially in the non-curative setting. However, reports on
the quality-of-life outcomes of dendritic cell-based
immunotherapy are scarce. One study9 assessing
55 patients with renal cell carcinoma treated with dendritic
cells showed no negative eect of dendritic cell-based
immunotherapy on quality of life, thereby comparing
favourably with other existing and emerging therapies for
renal cell carcinoma that can cause substantial toxicity and
seriously impair quality of life.
www.thelancet.com/oncology Vol 15 June 2014
Lancet Oncol 2014; 15: e25767
Center for Cell Therapy and
Regenerative Medicine,
Antwerp University Hospital,
Edegem, Belgium
(S Anguille MD,
Prof E L Smits PhD,
Prof Z N Berneman FRCP); and
Laboratory of Experimental
Hematology, Tumor
Immunology Group (TIGR),
Vaccine and Infectious Disease
Institute (VAXINFECTIO)
(S Anguille, E Lion,
Prof V F van Tendeloo PhD,
Prof Z N Berneman), and Center
for Oncological Research
(Prof E L Smits), University of
Antwerp, Faculty of Medicine
and Health Sciences, Antwerp,
Belgium
Correspondence to:
Dr Sbastien Anguille, Antwerp
University Hospital (UZA), Center
for Cell Therapy and
Regenerative Medicine (U111),
Wilrijkstraat 10, 2650 Edegem,
Belgium
sebastien.anguille@uantwerp.
be
See Online for appendix
Antitumour immune responses
The main goal of cancer vaccine strategies involving
dendritic cells is to stimulate tumour antigen-specic
cytotoxic T lymphocytes that can recognise and eliminate
e257
Review
Increase in immune
eector response
Reversal of
immunosuppression
Decrease in tumour burden
Increase in tumour immunogenicity
Chemotherapy
Adoptive
T-cell therapy
Increase of
lymphopeniaassociated
cytokines
COX-2
inhibitor
Radiation
therapy
Decrease of
tumour mass;
immunogenic
cell death
Decrease of
Tregs, MDSCs
Hormone
therapy
ATRA
TC
NK
MDSC
TC
VEGF
DC
TLR-L/cytokines
Interleukin 2 IMID/TKI
IDO
TC
MHC/Ag
TCR
CTL
CTLA-4
mAb
Treg
PD-1 CD25
mAb mAb
1-MT
Denileukin
diftitox
Patient selection
MRD or low tumour burden
(increase in likelihood of
developing immunity)
Early disease stage
(increase in time for
immunity to develop)
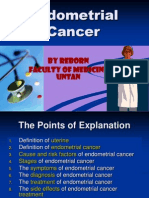
Figure: Combination strategies to maximise the therapeutic eectiveness of dendritic cell-based
immunotherapy and their underlying mechanisms of action
Dendritic cell-based cancer therapies seek to exploit the intrinsic capacity of dendritic cells to stimulate antitumour
immune eector cells, such as tumour antigen-specic cytotoxic T lymphocytes and natural killer cells. Therapeutic
interventions that aim to enhance the strength of the immune eector response (A), reverse tumour-associated
immunosuppression (B), or reduce the tumour burden and increase the immune susceptibility of the tumour cells
(C), are being actively pursued in combination with dendritic cell therapy. DC=dendritic cell. MHC/Ag=antigen bound
to major histocompatibility complex. TCR=T-cell receptor. CTL=cytotoxic T lymphocyte. NK=natural killer cell.
TLR-L=toll-like receptor ligand. mAb=monoclonal antibody. CTLA-4=cytotoxic T lymphocyte antigen-4.
PD-1=programmed death-1. MDSC=myeloid-derived suppressor cell. Treg=regulatory T cell.
IMID=immunomodulatory drug (eg, lenalidomide). TKI=tyrosine kinase inhibitor (eg, sunitinib).
COX-2 inhibitor=cyclooxygenase-2 inhibitor. ATRA=all-trans retinoic acid. VEGF=vascular endothelial growth factor.
IDO=indoleamine-2,3-dioxygenase. 1-MT=1-D-methyl-tryptophan. TC=tumour cell. MRD=minimal residual disease.
cancer cells in an antigen-specic way.2 According to
results of a meta-analysis of dendritic cell-based
immunotherapy, such cellular immune responses can be
elicited in 77% of patients with prostate cancer and 61%
with renal cell carcinoma.6 In view of the fact that most of
these patients have metastatic disease, this result
conrms that active immunisation with dendritic cells
can elicit adaptive antitumour immunity in many
patients, even in those with advanced disease who are
thought to be less immune responsive.10
Emerging evidence from clinical trials indicates that
dendritic cells, in addition to inducing tumour-specic
cytotoxic T lymphocytes, can also enhance natural-killercell immunity.11 Positive natural-killer-cell responses (eg,
increases in frequency, or induction of phenotypic or
functional activation, or both) have been noted in about
50% of patients after dendritic cell vaccination.11 This
e258
nding is particularly relevant in view of the growing
evidence indicating that natural killer cells play a key
part in the generation of protective anti-tumour
immunity.11 Natural killer cells can contribute to tumour
rejection both directly and indirectly by supporting the
generation of cytotoxic T-lymphocyte immunity.11 In a
murine melanoma model, Boudreau and colleagues12
showed that dendritic cells mediate tumour eradication
via both cytotoxic T lymphocytes and natural killer cells.
Notably, this eect was completely abrogated after
natural-killer-cell depletion,12 which underscores the
possibly pivotal role of natural killer cells in the
development of eective antitumour immunity by
dendritic cell vaccination.11,12
Taken together, these data indicate that dendritic cellbased immunotherapy can elicit adaptive and innate
antitumour immunity in at least half of all patients. This
action, coupled with the low occurrence of immunerelated adverse events, challenges the notion that
induction of cancer immunity by immunotherapy must
come at the cost of autoimmunity, as has been suggested
for other immunotherapies such as ipilimumab.7
Overall objective response
Despite their favourable safety proles and proven
immunogenicity, cancer vaccine strategies have received
a great deal of criticism, and even scepticism, because of
their poor therapeutic ecacy in terms of inducing
objective clinical responses.13 The same criticism has also
been levied at dendritic cell-based cancer vaccine
approaches.14 We did a systematic review of all published
clinical trials to document the proportion of patients who
had an objective response (achieving either a complete
response or partial response as dened by WHO criteria,
or by the Response Evaluation Criteria In Solid Tumors
[RECIST]13) after dendritic cell vaccination in melanoma,
prostate cancer, malignant glioma, and renal cell
carcinoma (appendix pp 112). From this review, we
conclude that the clinical benet of dendritic cell-based
immunotherapy in terms of objective response is real,
but small. With 85% of melanoma patients achieving an
objective response (appendix pp 23), dendritic cell
therapy has similar ecacy to dacarbazine (the standard
chemotherapeutic drug for treatment of melanoma) or to
ipilimumab, for which 515% of patients have an
objective response.15,16 For prostate cancer, 71% of
patients treated with dendritic cell therapy had an
objective response when assessed by either imaging
studies or by assessment of the prostate-specic antigen
(PSA) tumour marker level (appendix p 4), which is
similar to the 10% of patients with metastatic, androgenresistant prostate cancer who are treated with conventional
chemotherapeutic drugs.17 In patients with malignant
glioma, 156% of patients treated with dendritic cell
therapy had an objective response (appendix p 5). In
advanced renal cell carcinoma, dendritic cell therapy
produces an objective response in 115% of patients
www.thelancet.com/oncology Vol 15 June 2014
Review
Dendritic cell product
Control group
Status
ClinicalTrials.gov
identier
Melanoma
Autologous monocyte-derived DCs pulsed with melanoma peptides
Autologous DCs mixed with irradiated autologous tumour cells
suspended in GM-CSF (melapuldencel-T)
Dacarbazine
Autologous PBMCs
suspended in GM-CSF
Completed
Not yet recruiting
NA5
NCT01875653
Prostate
Autologous APCs (including DCs) loaded with PAP/GM-CSF
(sipuleucel-T)
Autologous APCs
Completed
NCT00005947
NCT00065442
NCT00779402
NCT01133704
Brain (GBM)
Autologous DCs pulsed with autologous tumour lysate (DC-VAX-L)
Autologous PBMCs
Recruiting
NCT00045968
Renal
Autologous DCs electroporated with autologous tumour mRNA and Sunitinib
CD40L mRNA, in combination with sunitinib (AGS-003)
Recruiting
NCT01582672
Excludes one study in prostate cancer that was withdrawn before enrolment (NCT00043212) and three studies with phase 2/3 design (NCT01759810, NCT01782274, and
NCT01782287). DCs=dendritic cells. GM-CSF=granulocyte macrophage colony-stimulating factor. PBMCs=peripheral blood mononuclear cells. APCs=antigen-presenting cells.
PAP/GM-CSF=chimeric antigen consisting of the prostate tumour antigen prostatic acid phosphatase (PAP) linked to GM-CSF. GBM=glioblastoma multiforme. NA=not available.
Table 1: Overview of completed and ongoing randomised phase 3 clinical trials of dendritic cell-based cancer immunotherapy, by cancer type
(appendix p 6), which is also similar to that obtained with
other immunotherapies such as interleukin 2.18
Survival benet
Whereas objective response is a rapid and direct
parameter with which to assess the antitumour activity
of an experimental treatment, survivalparticularly
overall survivalis generally thought of as the most
important outcome measure of therapeutic benet.19,20
Table 2 provides an overview of all published trials5,2162 of
dendritic cell vaccines in melanoma, prostate cancer,
malignant glioma, and renal cell carcinoma in which
overall survival comparisons have been done. Although
results of two melanoma trials did not show survival
benet,5,22 an increase in median overall survival of at
least 20% has been documented in most studies
(table 2).21,2335 Although many of these trials were early
phase and not designed primarily to measure survival,
the results obtained are nevertheless noteworthy,
especially in view of the fact that the bar for establishment
of a clinically meaningful improvement in median
overall survival is generally set at 20%.63 Perhaps the
most compelling evidence that dendritic cell therapy can
confer survival benet comes from the IMPACT study
in prostate cancer (table 2).42 In this phase 3 randomised
controlled trial, the dendritic cell-based therapeutic
sipuleucel-T (Dendreon, Seattle, WA) showed
signicantly larger median overall survival of patients
with metastatic hormone-resistant prostate cancer than
did placebo (table 1): median overall survival was
258 months in the experimental group versus
217 months in the control group.42 On the basis of this
survival advantage and despite few patients achieving an
objective response (<5%), sipuleucel-T was approved by
the US Food and Drug Administration in 2010.3 Phase 3
trials using overall survival as the primary endpoint are
underway in patients with advanced melanoma, glioma,
and renal cell carcinoma (table 1).
Importantly, a positive association between immunity
induced by dendritic cells and patient survival is
www.thelancet.com/oncology Vol 15 June 2014
increasingly being reported (appendix pp 1415). For
example, an integrated analysis of the immune
monitoring data collected during the IMPACT trial and
two other phase 3 studies of sipuleucel-T in prostate
cancer39,40,42 has shown a correlation between the
induction of antigen-specic immune responses by
sipuleucel-T and prolonged overall survival.64 These data
provide a mechanism for the clinical benet noted in
patients with prostate cancer treated with sipuleucel-T,
and link the increased overall survival in these patients to
the induction of tumour-specic immunity.6
Therapeutic eectiveness
The observed dissociation between objective response
and survival indicates that alternative surrogate endpoints
should be used to assess the therapeutic eectiveness of
dendritic cell-based immunotherapy. As outlined,
dendritic cell-based immunotherapeutic approaches can
positively aect clinical outcome in terms of increasing
patient survival rather than by inducing objective tumour
responses. Although this notion might seem
counterintuitive, for several tumour types and disease
settings tumour response criteria cannot be used to
accurately assess the eect of a certain treatment on
survival.65 This absence of association between objective
response and overall survival has been reported
particularly with the use of immunotherapeutic drugs
and targeted therapies.66 For example, ipilimumab
therapy signicantly improved overall survival of patients
with metastatic melanoma by 45 months (compared
with a control group given a tumour peptide vaccine),8
despite only 515% of patients having an objective
response.16 A phase 3 clinical trial of the tyrosine kinase
inhibitor sorafenib in patients with advanced renal cell
carcinoma yielded similar results, in which only 10% of
patients had an objective response,67 but survival was
nevertheless signicantly prolonged by 35 months
(compared with a placebo control group).68 These two
examples, along with the evidence presented in this
Review, suggest that the dissociation between objective
e259
Review
Evidence level
Overall survival
DC group
(months)
Dendritic cell product
Control group
(months)
% change
Dendritic cell type
Activation
Melanoma
N=1121
III-3
93
40
+133%
IL-4 moDCs
MCM
N=1322
III-1
62
148
58%
IL-4 moDCs
Immature
N=542325
III-1
640
310
+107%
IL-4 moDCs
GM-CSF
N=1726
III-3
224
80
+180%
IL-4 moDCs
TNF-
N=1127
III-3
73
40
+83%
IL-4 moDCs
TNF-/IL-1/IL-6/PGE2
N=16/22*28
III-2
123
58
+112%
IL-4 moDCs
TNF-/IL-1/IL-6/PGE2
N=2029,30
III-3
86
40
+115%
IL-4 moDCs
TNF-+Poly(I:C)
N=535
II
93
116
20%
IL-4 moDCs
TNF-/IL-1/IL-6/PGE2
N=3431
III-3
185
116
+60%
IL-4 moDCs
TNF-/IL-1/IL-6/PGE2
N=2832
III-3
94
51
+84%
IL-4 moDCs
TNF-/IL-1/IL-6/PGE2
N=2433
III-3
136
73
+86%
IL-4 moDCs
Immature
N=2934
III-3
150
83
+81%
IL-4 moDCs
TNF-/PGE2
N=1535
III-3
220
76
+189%
Natural pDCs
FSME-IMMUN
N=333638
III-3
>200
60
+233%
IL-4 moDCs
Immature
N=147/22539,40
II
232
189
+23%
Sipuleucel-T
GM-CSF
N=1241
III-3
210
1219
+1075%
IL-4 moDCs
TNF-/PGE2
N=341/51242
II
258
217
+19%
Sipuleucel-T
GM-CSF
Immature
Prostate
Brain
N=8/1443
III-2
333
75
+344%
IL-4 moDCs
N=1944
III-1
380
240
+58%
IL-4 moDCs
Immature
N=1245
III-2
234
183
+28%
IL-4 moDCs
Immature
N=1846
III-3
157
131
N=5647
III-3
96
N=1248
III-3
228
N=849
III-3
240
N=16/1750
III-3
170
N=1051
III-3
N=1552
+20%
IL-4 moDCs
OK-432
+3962%
IL-4 moDCs
TNF-/IL-1/PGE2
156
+46%; NS
IL-4 moDCs
TNF-/IL-1/IL-6
120
+100%
IL-4 moDCs
TNF-/IL-1/PGE2
125
+36%
IL-4 moDCs
Immature
280
146
+92%
IL-4 moDCs
TNF-/PGE2
III-3
359
140
+156%
IL-4 moDCs
+Imiquimod or poly(I:C)LC
N=7753
III-3
183
146
+25%
IL-4 moDCs
TNF-/IL-1/PGE2
N=1854
III-1
319
150
+113%
IL-4 moDCs
Immature
N=1355
III-2
170
105
+62%
IL-4 moDCs:
TNF-/IL-1/PGE2
N=556
III-3
270
123
+120%
IL-4 moDCs
TNF-/IFN-/Poly(I:C)
N=757
III-3
249
192
+30%; NS
IL-4 moDCs
TNF-/IL-1/IL-6/PGE2
6070
Renal
N=1058
III-3
198
+65120%
IL-4 moDCs
Immature
N=959
III-3
290
120
90120
+142%
IL-4 moDCs
MCM/CD40L/IFN
N=2760
III-3
166
127
+31%
IL-4 moDCs
TNF-/IL-1/IL-6/PGE2
N=1861
III-3
>180
138
+29%
IL-4 moDCs
TNF- +/ PGE2
N=10 (PR)62
III-3
91
53
+72%
moDCs
CD40L mRNA
N=11 (IR)62
III-3
395
207
+91%
moDCs
CD40L mRNA
Last update: Nov 14, 2013. DC=dendritic cell. N=total number of vaccinated patients. PR=poor-risk group. IR=intermediate-risk group. Evidence level is according to NHMRC
gradation system (http://www.nhmrc.gov.au), derived from dierent trial types: II=randomised controlled trial. III-1=pseudorandomised controlled trial (eg, other
treatment). III-2= trial including a non-randomised concurrent control group. III-3=trial without concurrent control group (eg, historical controls or comparison of two or
more single-group trials). % change=percentage change from overall survival in control group to DC group. NS=not signicant. IL-4 moDCs=interleukin-4-dierentiated
monocyte-derived DCs. pDCs=plasmacytoid DCs. MCM=monocyte-conditioned medium. GM-CSF=granulocyte macrophage colony-stimulating factor. TNF=tumour necrosis
factor. PGE2=prostaglandin E2. Poly(I:C)=polyinosinic:polycytidylic acid, a toll-like receptor (TLR)3 agonist. Poly(I:C)LC=poly(I:C) stabilised with lysine and
carboxymethylcellulose. FSME-IMMUN=tick-borne encephalitis vaccine. OK-432=picibanil, a TLR4 agonist. IFN=interferon. *M1c patient subgroup. newly diagnosed
glioblastoma multiforme patient subgroup. combined with sunitinib.
Table 2: Overview of dendritic cell vaccine trials in melanoma, prostate cancer, primary brain tumours (glioma), and renal cell cancer reporting overall
survival outcome
e260
www.thelancet.com/oncology Vol 15 June 2014
Review
response and overall survival is a class-specic occurrence
of immunotherapies and targeted therapies,66 and
corroborate the notion that the objective response might
not show the true clinical activity of these therapies.66,69,70
If eective, classic cytotoxic drugs usually cause fairly
rapid reductions in tumour size and, in such cases, the
objective response is a suitable parameter to assess
treatment response.69,70 By contrast, immunotherapies
often produce dierent clinical response patterns, none
of which are accurately captured by establishment of
objective response.69,70 Among these atypical response
proles, which are also frequently observed in the context
of dendritic cell-based immunotherapy, are delayed initial
increases in tumour burden associated with inammation
or immune cell inltration of the tumour lesions later
followed by regression, and changes in disease
progression kinetics.21,71 The response prole changes in
disease progression kinetics have been well documented
in patients with prostate cancer, in whom results of many
studies show that therapeutic cancer vaccines, including
dendritic cell-based vaccines, can attenuate the PSA
progression rate without signicantly reducing PSA
levels.71,72 Such response patterns cannot be classied as
objective with classic response assessment criteria;
however, they might be highly clinically relevant in view
of the association between changes in PSA kinetics and
the survival of patients with prostate cancer.73 Taken
together, these data underscore the idea that dendritic
cell-based immunotherapeutic strategies, and, by
extension, all cancer immunotherapies, necessitate
ecacy endpoints other than the traditional outcome
parameters used in oncology clinical trials.19,70 As outlined,
overall survival is the most appropriate endpoint in latestage clinical trials.20 For early-phase clinical trials, the
immune-related response criteria might be a valid
alternative to the classic WHO or RECIST criteria to
assess antitumour responses, because they accommodate
the atypical tumour response patterns recorded with
immunotherapies.69,70
How is the specialty evolving?
Trends
Among the studies of dendritic cell cancer vaccines
registered at http://www.clinicaltrials.gov, two main
emerging trends in dendritic cell-based anticancer
immunotherapy can be identied. The rst revolves
around the use of next-generation dendritic cell products
with improved immunostimulatory activity. The second
is to potentiate the eectiveness of dendritic cell
immunotherapy through combination therapy.
Next-generation dendritic cell vaccines
Most published clinical trials have been done with earlygeneration dendritic cell vaccines, including dendritic
cell-enriched cell preparations (eg, sipuleucel-Ta crude
preparation of prostate antigen-loaded, GM-CSFactivated blood mononuclear cells of which dendritic
www.thelancet.com/oncology Vol 15 June 2014
cells constitute only a small proportion) and interleukin-4
monocyte dendritic cells (dendritic cells generated ex
vivo from peripheral blood monocytes in the presence of
GM-CSF and interleukin 4; table 2).3 The interleukin-4
monocyte dendritic celleither used in its immature
form or after activation or maturation with a proinammatory cytokine cocktail composed of tumour
necrosis factor (TNF) , interleukin 1, interleukin 6, and
prostaglandin E2is by far the most commonly used
dendritic cell type in clinical trials (table 2).4
Which dendritic cell vaccine parameters are important
for clinical eectiveness is not fully understood. Although
clinical benet has been shown in trials using immature
interleukin-4 monocyte dendritic cells (table 2) and many
individual studies have not established a correlation
between dendritic cell activation parameters and survival
outcome,28,31,33,43 results of a meta-analysis of dendritic cell
immunotherapy in prostate cancer have shown a clear
superiority of mature monocyte dendritic cells over their
immature counterparts in terms of clinical outcome.6
Similar observations have been made in the context of
melanoma74 and malignant glioma.46 In addition to
maturation state, the ability of dendritic cells to produce
interleukin 12p70which favours the induction of a
protective T-helper type 1 (Th1) immune responseis
being increasingly recognised as an important determinant
of clinical activity.3 In two clinical trials, one in glioma75 and
one in melanoma,76 high concentrations of dendritic cellderived interleukin 12p70 were predictive of favourable
clinical outcome.
This evidence explains the impetus behind the recent
and ongoing eorts to develop the next generation of
dendritic cell vaccines biased to induce a Th1 immune
response (referred to as type 1-polarised dendritic cells)
and endowed with a superior capacity to elicit tumour
antigen-specic cytotoxic T lymphocytes and naturalkiller-cell immunity.3 The aim of this work is not to
provide an exhaustive compilation of all available nextgeneration dendritic cell vaccine protocols, but to touch
on some salient examples to show the main trends in
this eld of research. Several groups, including ours,
have shown interest in use of Langerhans cell-type
dendritic cells as vehicles for dendritic cell vaccination in
view of their remarkable eciency to stimulate cytotoxic
T lymphocyte immunity.77 Langerhans cell-like dendritic
cells can be derived from CD34-positive haemopoietic
progenitors,78 or from CD14-positive monocytes cultured
with interleukin 15 (instead of interleukin 4).79 Clinical
studies using these Langerhans cell-type dendritic cells
are
underway
in
melanoma
(NCT00700167,78
NCT01456104, and NCT01189383). In view of the key role
of interleukin 12p70 and the observed absence of
interleukin 12p70 production with use of the classic
maturation cocktail of TNF-, interleukin 1,
interleukin 6, and prostaglandin E2, much work has
been devoted to development of alternative maturationinducing regimens.4 Examples of maturation stimuli that
e261
Review
allow for the generation of dendritic cells with the desired
capacity to produce interleukin 12p70 are CD40L with
interferon ;76 toll-like receptor ligands (eg, TLR3 agonist
poly[I:C]);80 or a combination of TNF-, interleukin 1,
interferon , interferon , and polyI:C.75 In patients with
malignant glioma, dendritic cells matured with the latter
combination (designated as -type-1-polarised dendritic
cells) have shown potent ability to produce interleukin
12p70 and to augment the expression of the cytotoxic
T-lymphocyte-attracting chemokine CXCL10 in the
tumour microenvironment,75 which has been identied
as another key factor in the therapeutic activity of
dendritic cell vaccines in a murine study of malignant
glioma.81 The clinical eectiveness of -type-1-polarised
dendritic cells is being further assessed in several clinical
trials in melanoma (NCT00390338), prostate cancer
(NCT00970203), and glioma (NCT00766753).
Combination therapy
Categorisation
The appendix (pp 1618) provides an overview of the
dierent therapeutic interventions being assessed in
terms of their potential synergistic interaction with
dendritic cell vaccination. In this Review, for clarity, we
have divided these interventions into three categories on
the basis of their principal mechanism of action (gure).
Interventions that enhance the strength of the immune
eector response
Immune inhibitory pathways often dominate in
patients with cancer and can aect the eectiveness of
dendritic cell-based immunotherapy by preventing
cytotoxic T lymphocytes and natural killer cells from
exerting their eector function (gure). The immune
checkpoint receptors CTLA-4 and programmed death-1
(PD-1) are among the best understood molecules
involved in the negative regulation of cytotoxic
T-lymphocyte function.3 In recent years, several
monoclonal antibodies that can interfere with these
inhibitory molecules have become available for clinical
application, opening up the prospect of their use in
combination with dendritic cell-based immunotherapy.3
Preliminary clinical evidence obtained in patients with
advanced melanoma suggests that dendritic cell therapy
in combination with CTLA-4-targeting monoclonal
antibodies is more eective than is use of these agents
as monotherapies.82,83 However, we believe that these
monoclonal antibodies should be used with caution in
view of their potential (immune-related) toxicity. AntiPD-1 monoclonal antibodies seem to have a more
favourable toxicity prole, and can even be combined
with ipilimumab without a signicant increase in the
rate of immune-related adverse events.84,85 In view of
this prole, therapeutic blockade of the PD-1/PD
ligand 1 pathway might be a more viable strategy from
the perspective of clinical applicability. Several antiPD-1 monoclonal antibodies have entered the clinical
e262
trial stage,84,85 one of which (pidilizumab; CT-011) is
being tested in combination with dendritic cell therapy
in four clinical trials (appendix p 18).
Toll-like receptor agonists and cytokines (eg,
interferon ) have also come under intense scrutiny as
dendritic cell vaccine adjuvants to harness the antitumour
eector response (gure).86,87 These stimuli can either be
incorporated into the vaccine itselfeg, as ex-vivo
maturation agentsor applied concomitantly with the
dendritic cell vaccine (appendix pp 1718).75 Perhaps the
most extensively studied cytokine used in combination
with dendritic cell vaccination is interleukin 2. Despite
strong preclinical evidence supporting this combination,88
results of clinical trials have not shown that the addition
of interleukin 2 to dendritic cell vaccine regimens results
in a superior induction of antitumour immunity.89,90
Moreover, interleukin 2 could negatively aect dendritic
cell immunotherapy by causing an undesired stimulation
of regulatory T cells (Tregs) or of myeloid-derived
suppressor cells (MDSCs), or both (gure).32,91
The antitumour immune responses elicited by
dendritic cell therapy can also be potentiated by
stimulation of the endogenous production of immunostimulatory cytokines. This process can be achieved with
lymphodepleting chemotherapy regimens, such as
temozolomide or cyclophosphamide with or without
udarabine.92 These therapies seek to reboot the immune
system by elimination of negative immune-cell
populations (eg, Tregs) and creation of an optimum
cytokine milieu (eg, interleukin 7 and interleukin 15) for
expansion of antitumour eector cells, including natural
killer cells and tumour antigen-specic cytotoxic
T lymphocytes (gure).93,94 This recovery phase after
lymphodepletion provides an ideal opportunity for
dendritic cell vaccination in combination with adoptive
transfer of immune eector cells (gure).94 This strategy
has generated promising results in preclinical studies
and in a pilot clinical trial,95,96 and is being pursued in
several ongoing clinical studies (appendix p 18).
Interventions that reverse tumour-associated
immunosuppression
The translation of dendritic cell-induced antitumour
immunity into clinical activity needs to overcome the
immune suppressive barrier that is imposed by Tregs,
MDSCs, and other negative immune regulators
(gure).3,10,97 Tregs are by far the best characterised cells
that prevent the generation of eective antitumour
responses.98 Two main strategies are being used to
modulate Tregs in dendritic cell-based immunotherapy
protocols. First, dendritic cells themselves can be
harnessed to target Tregs, which can be achieved, for
example, by loading dendritic cells with antigenic
components of the Treg transcription factor forkhead
box P3 (FoxP3) to mount a FoxP3-directed cytotoxic
T-lymphocyte response.98 Second, dendritic cells can be
combined with Treg-targeting drugs, such as the
www.thelancet.com/oncology Vol 15 June 2014
Review
monoclonal antibodies basiliximab and daclizumab
(appendix p 17; gure).98 These monoclonal antibodies are
directed towards the interleukin-2 receptor chain
(CD25), which is abundantly expressed on the surface of
Tregs (gure). The combination of dendritic cell therapy
and daclizumab has been examined in patients with
metastatic melanoma.99 Daclizumab eectively depleted
Tregs but also targeted tumour-specic T cells
(presumably because of the expression of CD25 on
activated T cells) and impaired their functionality.99
Denileukin diftitox, a fusion protein composed of
interleukin 2 and diphtheria toxin, is another CD25directed approach to deplete Tregs (gure). In patients
with advanced renal cell carcinoma, the addition of
denileukin diftitox to dendritic cell vaccination resulted in
a 16-fold increase in the frequency of tumour-specic
cytotoxic T lymphocytes.100 In another study,101 dendritic
cell therapy induced a more persistent cytotoxic
T-lymphocyte response after Tregs were depleted by
denileukin diftitox. By contrast, Baur and colleagues102
showed that denileukin diftitox can negatively aect the
capacity of dendritic cells to induce tumour-specic
cytotoxic T lymphocytes by inducing a tolerogenic
phenotype in dendritic cells, and by promoting the
survival of non-activated Tregs.102 Moreover, CD25 can
also be expressed on activated natural killer cells (gure)
and, consequently, denileukin diftitox can also lead to
depletion of natural killer cells.103 Collectively, these data
indicate that CD25-based Treg-targeting strategies, such
as denileukin diftitox, can produce paradoxical
immunological eects that can impair the activity of
dendritic cell vaccination. Non-CD25-based methods,
such as low-dose cyclophosphamide or 1-methyl-Dtryptophan,98 might therefore be more appropriate.
Clinical trials of metronomically dosed cyclophosphamide
in combination with dendritic cell therapy have yielded
mixed results and have not consistently shown a reduction
in the frequency of Tregs.93 However, these results do not
necessarily preclude a possible benecial eect of
cyclophosphamide on dendritic cell vaccine ecacy,
because cyclophosphamide might enhance antitumour
immunity via mechanisms other than Treg elimination
(eg, by directly aecting the dendritic cell compartment).104
Indoleamine-2,3-dioxygenase, an immunoregulatory
enzyme that supports Treg function and numbers, can be
inhibited by 1-methyl-D-tryptophan (gure);87 clinical
trials of its combined use with dendritic cell therapy are
underway (appendix p 17). The antitumour activities of
several newer anticancer drugs, such as the VEGFtargeting monoclonal antibody bevacizumab, the
immunomodulatory drug lenalidomide, and the tyrosine
kinase inhibitors dasatinib and sunitinib also seem to
rely, at least in part, on their inhibitory activities on Tregs
(gure).105,106 Sunitinib is being tested in combination with
dendritic cell-based immunotherapy in a phase 3 clinical
trial in patients with advanced renal cell carcinoma
(table 1, appendix pp 1718).
www.thelancet.com/oncology Vol 15 June 2014
In addition to Tregs, MDSCs are being increasingly
recognised as important mediators of tumour-induced
immunosuppression.107 MDSCs exert negative eects on
both T cells and natural killer cells,107 and can directly
impair the activity of dendritic cell vaccines.108 This eect
provides a compelling rationale to combine dendritic cell
vaccination with MDSC-targeted interventions, such as
VEGF inhibitors, lenalidomide, all-trans retinoic acid,
chemotherapeutic drugs (eg, gemcitabine), and
cyclooxygenase-2 (COX-2) inhibitors (gure, appendix
pp 1718).105,107 COX-2 inhibitors diminish expression of the
MDSC-attracting chemokine CCL2 in the tumour bed, and
promote tumour inltration by cytotoxic T lymphocytes
through increasing the concentration of CXCL10, thereby
creating a favourable immune context for the induction of
antitumour immunity by dendritic cells.75,109 Tyrosine
kinase inhibitors such as sunitinib and vemurafenib can
also reverse MDSC-mediated immunosuppression.107,110
Vemurafenib, a BRAF inhibitor, has become available for
treatment of advanced BRAFV600E-positive melanoma.111
Apart from its direct antimelanoma activity, vemurafenib
exerts a wide range of benecial immunomodulatory
eects. Like COX-2 inhibitors, vemurafenib reduces
tumour CCL2 expression and mobilises antitumour
eector cells into the tumour microenvironment.111 These
eects, coupled with its inhibitory action on Tregs111 and
MDSCs,110 make vemurafenib an attractive candidate for
combination therapy with dendritic cell vaccination.112
Interventions to reduce tumour burden and increase immune
susceptibility of tumour cells
The level of tumour-induced immunosuppression is a
function of the total burden of the tumour.10 This
observation led to the suggestion that immunotherapies
might function less well in the context of high tumour
burden.10 Ample evidence supports the hypothesis that
patients with advanced or bulky disease are less likely to
benet from cancer immunotherapy, including dendritic
cell therapy, than are patients with less-advanced
disease.97,113 A good example of this inverse association
between tumour burden and the eectiveness of
immunotherapy comes from haematology, in which
dendritic cell therapy has shown little eectiveness in
patients with relapsed or progressive acute myeloid
leukaemia, but strong antileukaemic activity in patients
with minimal residual disease.114,115
These considerations provide a rationale for combination
of dendritic cell therapy with cytoreductive cancer
treatments (eg, chemotherapy) to bring the patient to a
state of low tumour burden or minimal residual disease
state (gure).10,113 In view of the fact that chemotherapy by
itself has immunosuppressive eects, and that patients
heavily pretreated with chemotherapy are less responsive
to subsequent immunotherapy,94 the idea of combination
of immunotherapy and chemotherapy seems counterintuitive. Nevertheless, this theory has been challenged by
several clinical trials, the results of which showed that this
e263
Review
Search strategy and selection criteria
We selected references through a PubMed search with the terms dendritic cells, cancer,
and immunotherapy. We retrieved data presented in table 1 and appendix pp 1718 from
the online clinical trial database http://www.clinicaltrials.gov with the search term
dendritic cells. We excluded studies with the status withdrawn. We identied relevant
records for the data presented in table 2, appendix pp 212, and appendix pp 1415 by a
systematic search of PubMed for all studies published between Jan 1, 1995, and Nov 14,
2013, containing the following search terms: dendritic cells AND clinical trial AND
melanoma OR prostate cancer OR glioblastoma OR renal cell carcinoma. We
identied additional records by screening bibliographies of key articles on the subject and
by screening conference proceedings of the American Society of Clinical Oncology (ASCO).
We excluded articles not published in English, case reports, and duplicate publications.
combinatorial approach might be highly synergistic.92,97,116,117
Many mechanisms seem to be involved in the synergistic
interaction between chemotherapy and dendritic cell
therapy. Apart from the aforementioned immunepotentiating eects (ie, reversal of tumour-induced
immunosuppression associated with high tumour burden,
creation of a lymphopenic state favouring expansion of
antitumour eector cells, and inhibition or depletion, or
both, of Tregs and MDSCs), many chemotherapeutic
drugs seem able to induce immunogenic tumour cell
death, making these cells more susceptible to antitumour
immunity elicited by dendritic cell therapy (gure).94,118
Dendritic cell therapies are being increasingly integrated
into existing chemotherapy schedules, which indicates
that the concept of chemoimmunotherapy is becoming an
important treatment model in the area of dendritic cellbased immunotherapy (appendix p 17). Other conventional
anticancer treatmentsie, radiation therapy and hormonal
therapyalso have pleiotropic immunomodulatory eects
that extend beyond their primary mode of action, and that
can be exploited to increase the activity of dendritic cellbased immunotherapy.97,119,120
Conclusion
We conclude that dendritic cell therapy is a safe and well
tolerated immunotherapeutic method that can elicit
immunity even in patients with advanced-stage cancer.
This work also conrms that dendritic cell-based
interventions have only some capacity to produce
objective tumour responses, as established by classic
response assessment criteria such as RECIST. Although
not all studies were designed primarily to measure
survival, an increasing number indicate that dendritic cell
therapy could confer a survival benet. These preliminary
but encouraging survival data provide a strong incentive
to begin a new series of clinical trials using overall
survival as the primary endpoint or using surrogate
endpoints for clinical eectiveness (eg, the proposed
immune-related response criteria).69,70 We foresee that the
specialty will benet from two developments, which are
already beginning to be incorporated in clinical trials: the
implementation of the next generation of dendritic cell
e264
vaccines with optimised activity; and the rational use of
these vaccines in combination with other anticancer
therapies that could improve their eectiveness. These
developments might hold the key to the full therapeutic
potential of dendritic cells for cancer immunotherapy.
Contributors
SA researched the data, wrote the Review, and designed the gure. ELS,
EL, VFvT, and ZNB reviewed and revised the manuscript for intellectual
content.
Declaration of interests
We declare no competing interests.
Acknowledgments
We thank Jan-Baptist Vermorken for critical reading of the manuscript,
and acknowledge the Research Foundation Flanders (FWO Vlaanderen),
the Flemish League against Cancer (Vlaamse Liga tegen Kanker), the
Belgian Foundation against Cancer (Stichting tegen Kanker), and the
Belgian public utility foundation VOCATIO for their invaluable support.
SA holds an Emmanuel van der Schueren fellowship of the Flemish
League against Cancer.
References
1
Steinman RM, Cohn ZA. Identication of a novel cell type in
peripheral lymphoid organs of mice. I. Morphology, quantitation,
tissue distribution. J Exp Med 1973; 137: 114262.
2
Palucka K, Banchereau J. Cancer immunotherapy via dendritic
cells. Nat Rev Cancer 2012; 12: 26577.
3
Kirkwood JM, Buttereld LH, Tarhini AA, Zarour H, Kalinski P,
Ferrone S. Immunotherapy of cancer in 2012. CA Cancer J Clin
2012; 62: 30935.
4
Tacken PJ, de Vries IJ, Torensma R, Figdor CG. Dendritic-cell
immunotherapy: from ex vivo loading to in vivo targeting.
Nat Rev Immunol 2007; 7: 790802.
5
Schadendorf D, Ugurel S, Schuler-Thurner B, et al, and the DC
study group of the DeCOG. Dacarbazine (DTIC) versus vaccination
with autologous peptide-pulsed dendritic cells (DC) in rst-line
treatment of patients with metastatic melanoma: a randomized
phase III trial of the DC study group of the DeCOG. Ann Oncol
2006; 17: 56370.
6
Draube A, Klein-Gonzlez N, Mattheus S, et al. Dendritic cell based
tumor vaccination in prostate and renal cell cancer: a systematic
review and meta-analysis. PLoS One 2011; 6: e18801.
7
Amos SM, Duong CP, Westwood JA, et al. Autoimmunity
associated with immunotherapy of cancer. Blood 2011;
118: 499509.
8
Hodi FS, ODay SJ, McDermott DF, et al. Improved survival with
ipilimumab in patients with metastatic melanoma. N Engl J Med
2010; 363: 71123.
9
Leonhartsberger N, Ramoner R, Falkensammer C, et al. Quality of
life during dendritic cell vaccination against metastatic renal cell
carcinoma. Cancer Immunol Immunother 2012; 61: 140713.
10 Widn K, Mozaari F, Choudhury A, Mellstedt H. Overcoming
immunosuppressive mechanisms. Ann Oncol 2008;
19 (suppl 7): vii 24147.
11 Lion E, Smits EL, Berneman ZN, Van Tendeloo VF. NK cells: key
to success of DC-based cancer vaccines? Oncologist 2012;
17: 125670.
12 Boudreau JE, Bridle BW, Stephenson KB, et al. Recombinant
vesicular stomatitis virus transduction of dendritic cells enhances
their ability to prime innate and adaptive antitumor immunity.
Mol Ther 2009; 17: 146572.
13 Rosenberg SA, Yang JC, Restifo NP. Cancer immunotherapy:
moving beyond current vaccines. Nat Med 2004; 10: 90915.
14 Huber ML, Haynes L, Parker C, Iversen P. Interdisciplinary critique
of sipuleucel-T as immunotherapy in castration-resistant prostate
cancer. J Natl Cancer Inst 2012; 104: 27379.
15 Robert C, Thomas L, Bondarenko I, et al. Ipilimumab plus
dacarbazine for previously untreated metastatic melanoma.
N Engl J Med 2011; 364: 251726.
16 Weber J. Overcoming immunologic tolerance to melanoma:
targeting CTLA-4 with ipilimumab (MDX-010). Oncologist 2008;
13 (suppl 4): 1625.
www.thelancet.com/oncology Vol 15 June 2014
Review
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
Tay M-H, Nakabayashi M, Oh WK. Management of hormone
refractory prostate cancer. In: Vogelzang NJ, Scardino PT,
Shipley WU, Debruyne FMJ, Linehan WM, eds. Comprehensive
textbook of genitourinary oncology, 3 edn. Philadelphia, PA:
Lippincott Williams & Wilkins, 2006: 34154.
Coppin C, Porzsolt F, Awa A, Kumpf J, Coldman A, Wilt T.
Immunotherapy for advanced renal cell cancer.
Cochrane Database Syst Rev 2005; 1: CD001425.
Madan RA, Gulley JL, Fojo T, Dahut WL. Therapeutic cancer
vaccines in prostate cancer: the paradox of improved survival
without changes in time to progression. Oncologist 2010; 15: 96975.
Saad ED, Buyse M. Overall survival: patient outcome, therapeutic
objective, clinical trial end point, or public health measure?
J Clin Oncol 2012; 30: 175054.
Thurner B, Haendle I, Rder C, et al. Vaccination with mage-3A1
peptide-pulsed mature, monocyte-derived dendritic cells expands
specic cytotoxic T cells and induces regression of some metastases
in advanced stage IV melanoma. J Exp Med 1999; 190: 166978.
Slinglu CL Jr, Petroni GR, Yamshchikov GV, et al. Clinical and
immunologic results of a randomized phase II trial of vaccination
using four melanoma peptides either administered in granulocytemacrophage colony-stimulating factor in adjuvant or pulsed on
dendritic cells. J Clin Oncol 2003; 21: 401626.
Dillman R, Selvan S, Schiltz P, et al. Phase I/II trial of melanoma
patient-specic vaccine of proliferating autologous tumor cells,
dendritic cells, and GM-CSF: planned interim analysis.
Cancer Biother Radiopharm 2004; 19: 65865.
Dillman RO, Selvan SR, Schiltz PM, et al. Phase II trial of dendritic
cells loaded with antigens from self-renewing, proliferating
autologous tumor cells as patient-specic antitumor vaccines in
patients with metastatic melanoma: nal report.
Cancer Biother Radiopharm 2009; 24: 31119.
Dillman RO, Cornforth AN, Depriest C, et al. Tumor stem cell
antigens as consolidative active specic immunotherapy: a
randomized phase II trial of dendritic cells versus tumor cells in
patients with metastatic melanoma. J Immunother 2012;
35: 64149.
Trefzer U, Herberth G, Wohlan K, et al. Vaccination with hybrids of
tumor and dendritic cells induces tumor-specic T-cell and clinical
responses in melanoma stage III and IV patients. Int J Cancer 2004;
110: 73040.
Vilella R, Bentez D, Mil J, et al. Pilot study of treatment of
biochemotherapy-refractory stage IV melanoma patients with
autologous dendritic cells pulsed with a heterologous melanoma
cell line lysate. Cancer Immunol Immunother 2004; 53: 65158.
Kyte JA, Mu L, Aamdal S, et al. Phase I/II trial of melanoma therapy
with dendritic cells transfected with autologous tumor-mRNA.
Cancer Gene Ther 2006; 13: 90518.
Nakai N, Asai J, Ueda E, Takenaka H, Katoh N, Kishimoto S.
Vaccination of Japanese patients with advanced melanoma with
peptide, tumor lysate or both peptide and tumor lysate-pulsed
mature, monocyte-derived dendritic cells. J Dermatol 2006;
33: 46272.
Nakai N, Katoh N, Kitagawa T, Ueda E, Takenaka H, Kishimoto S.
Evaluation of survival in Japanese stage IV melanoma patients
treated with melanoma antigen-pulsed mature monocyte-derived
dendritic cells. J Dermatol 2008; 35: 80103.
Hersey P, Halliday GM, Farrelly ML, DeSilva C, Lett M,
Menzies SW. Phase I/II study of treatment with matured dendritic
cells with or without low dose IL-2 in patients with disseminated
melanoma. Cancer Immunol Immunother 2008; 57: 103951.
Ellebaek E, Engell-Noerregaard L, Iversen TZ, et al. Metastatic
melanoma patients treated with dendritic cell vaccination,
Interleukin-2 and metronomic cyclophosphamide: results from a
phase II trial. Cancer Immunol Immunother 2012; 61: 1791804.
Oshita C, Takikawa M, Kume A, et al. Dendritic cell-based
vaccination in metastatic melanoma patients: phase II clinical trial.
Oncol Rep 2012; 28: 113138.
Aarntzen EH, De Vries IJ, Lesterhuis WJ, et al. Targeting CD4(+)
T-helper cells improves the induction of antitumor responses in
dendritic cell-based vaccination. Cancer Res 2013; 73: 1929.
Tel J, Aarntzen EH, Baba T, et al. Natural human plasmacytoid
dendritic cells induce antigen-specic T-cell responses in melanoma
patients. Cancer Res 2013; 73: 106375.
www.thelancet.com/oncology Vol 15 June 2014
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
Murphy G, Tjoa B, Ragde H, Kenny G, Boynton A. Phase I clinical
trial: T-cell therapy for prostate cancer using autologous dendritic
cells pulsed with HLA-A0201-specic peptides from prostatespecic membrane antigen. Prostate 1996; 29: 37180.
Tjoa BA, Erickson SJ, Bowes VA, et al. Follow-up evaluation of
prostate cancer patients infused with autologous dendritic cells
pulsed with PSMA peptides. Prostate 1997; 32: 27278.
Tjoa BA, Simmons SJ, Bowes VA, et al. Evaluation of phase I/II
clinical trials in prostate cancer with dendritic cells and PSMA
peptides. Prostate 1998; 36: 3944.
Small EJ, Schellhammer PF, Higano CS, et al. Placebo-controlled
phase III trial of immunologic therapy with sipuleucel-T (APC8015)
in patients with metastatic, asymptomatic hormone refractory
prostate cancer. J Clin Oncol 2006; 24: 308994.
Higano CS, Schellhammer PF, Small EJ, et al. Integrated data from
2 randomized, double-blind, placebo-controlled, phase 3 trials of
active cellular immunotherapy with sipuleucel-T in advanced
prostate cancer. Cancer 2009; 115: 367079.
Hildenbrand B, Sauer B, Kalis O, et al. Immunotherapy of patients
with hormone-refractory prostate carcinoma pre-treated with
interferon-gamma and vaccinated with autologous PSA-peptide
loaded dendritic cellsa pilot study. Prostate 2007; 67: 50008.
Kanto PW, Higano CS, Shore ND, et al, and the IMPACT Study
Investigators. Sipuleucel-T immunotherapy for castration-resistant
prostate cancer. N Engl J Med 2010; 363: 41122.
Yu JS, Liu G, Ying H, Yong WH, Black KL, Wheeler CJ. Vaccination
with tumor lysate-pulsed dendritic cells elicits antigen-specic,
cytotoxic T-cells in patients with malignant glioma. Cancer Res 2004;
64: 497379.
Niu H, Dong Z, Dong F, Zhang T, Lei T, Xue D. Experimental and
clinical research of dendritic cell and syngeneic immunotherapy of
brain glioma. Chinese-German J Clin Oncol 2004; 3: 14750.
Liau LM, Prins RM, Kiertscher SM, et al. Dendritic cell vaccination
in glioblastoma patients induces systemic and intracranial T-cell
responses modulated by the local central nervous system tumor
microenvironment. Clin Cancer Res 2005; 11: 551525.
Yamanaka R, Homma J, Yajima N, et al. Clinical evaluation of
dendritic cell vaccination for patients with recurrent glioma: results
of a clinical phase I/II trial. Clin Cancer Res 2005; 11: 416067.
De Vleeschouwer S, Fieuws S, Rutkowski S, et al. Postoperative
adjuvant dendritic cell-based immunotherapy in patients with
relapsed glioblastoma multiforme. Clin Cancer Res 2008;
14: 3098104.
Sampson JH, Archer GE, Mitchell DA, et al. An epidermal growth
factor receptor variant III-targeted vaccine is safe and immunogenic
in patients with glioblastoma multiforme. Mol Cancer Ther 2009;
8: 277379.
Ardon H, Van Gool S, Lopes IS, et al. Integration of autologous
dendritic cell-based immunotherapy in the primary treatment for
patients with newly diagnosed glioblastoma multiforme: a pilot
study. J Neurooncol 2010; 99: 26172.
Chang CN, Huang YC, Yang DM, et al. A phase I/II clinical trial
investigating the adverse and therapeutic eects of a postoperative
autologous dendritic cell tumor vaccine in patients with malignant
glioma. J Clin Neurosci 2011; 18: 104854.
Fadul CE, Fisher JL, Hampton TH, et al. Immune response in
patients with newly diagnosed glioblastoma multiforme treated
with intranodal autologous tumor lysate-dendritic cell vaccination
after radiation chemotherapy. J Immunother 2011; 34: 38289.
Prins RM, Soto H, Konkankit V, et al. Gene expression prole
correlates with T-cell inltration and relative survival in
glioblastoma patients vaccinated with dendritic cell
immunotherapy. Clin Cancer Res 2011; 17: 160315.
Ardon H, Van Gool SW, Verschuere T, et al. Integration of
autologous dendritic cell-based immunotherapy in the standard of
care treatment for patients with newly diagnosed glioblastoma:
results of the HGG-2006 phase I/II trial.
Cancer Immunol Immunother 2012; 61: 203344.
Cho DY, Yang WK, Lee HC, et al. Adjuvant immunotherapy with
whole-cell lysate dendritic cells vaccine for glioblastoma multiforme:
a phase II clinical trial. World Neurosurg 2012; 77: 73644.
Jie X, Hua L, Jiang W, Feng F, Feng G, Hua Z. Clinical application
of a dendritic cell vaccine raised against heat-shocked glioblastoma.
Cell Biochem Biophys 2012; 62: 9199.
e265
Review
56
57
58
59
60
61
62
63
64
65
66
67
68
69
70
71
72
73
74
75
76
e266
Valle RD, de Cerio AL, Inoges S, et al. Dendritic cell vaccination in
glioblastoma after uorescence-guided resection. World J Clin Oncol
2012; 3: 14249.
Vik-Mo EO, Nyakas M, Mikkelsen BV, et al. Therapeutic vaccination
against autologous cancer stem cells with mRNA-transfected
dendritic cells in patients with glioblastoma.
Cancer Immunol Immunother 2013; 62: 1499509.
Su Z, Dannull J, Heiser A, et al. Immunological and clinical
responses in metastatic renal cancer patients vaccinated with tumor
RNA-transfected dendritic cells. Cancer Res 2003; 63: 212733.
Kim JH, Lee Y, Bae Y-S, et al. Phase I/II study of immunotherapy
using autologous tumor lysate-pulsed dendritic cells in patients
with metastatic renal cell carcinoma. Clin Immunol 2007;
125: 25767.
Berntsen A, Trepiakas R, Wenandy L, et al. Therapeutic dendritic
cell vaccination of patients with metastatic renal cell carcinoma:
a clinical phase 1/2 trial. J Immunother 2008; 31: 77180.
Schwaab T, Schwarzer A, Wolf B, et al. Clinical and immunologic
eects of intranodal autologous tumor lysate-dendritic cell vaccine
with Aldesleukin (interleukin 2) and IFN-alpha2a therapy in
metastatic renal cell carcinoma patients. Clin Cancer Res 2009;
15: 498692.
Amin A, Dudek A, Logan T, et al. Prolonged survival with
personalized immunotherapy (AGS-003) in combination with
sunitinib in unfavorable risk metastatic RCC (mRCC).
Proc Am Soc Clin Oncol 2013; 31 (suppl 6): abstr 357.
American Society of Clinical Oncology. Dening clinically
meaningful outcomes: ASCO recommendations to raise the bar for
clinical trials. 2013. http://www.asco.org/sites/www.asco.org/les/
asco_meaningful_outcomes_draft_for_website_-_05_13_13_0.pdf
(accessed May 8, 2014).
Sheikh NA, Petrylak D, Kanto PW, et al. Sipuleucel-T immune
parameters correlate with survival: an analysis of the randomized
phase 3 clinical trials in men with castration-resistant prostate
cancer. Cancer Immunol Immunother 2013; 62: 13747.
Johnson JR, Williams G, Pazdur R. End points and United States
Food and Drug Administration approval of oncology drugs.
J Clin Oncol 2003; 21: 140411.
Sharma P, Wagner K, Wolchok JD, Allison JP. Novel cancer
immunotherapy agents with survival benet: recent successes and
next steps. Nat Rev Cancer 2011; 11: 80512.
Escudier B, Eisen T, Stadler WM, et al, and the TARGET Study
Group. Sorafenib in advanced clear-cell renal-cell carcinoma.
N Engl J Med 2007; 356: 12534.
Escudier B, Eisen T, Stadler WM, et al. Sorafenib for treatment of
renal cell carcinoma: nal ecacy and safety results of the phase III
treatment approaches in renal cancer global evaluation trial.
J Clin Oncol 2009; 27: 331218.
Wolchok JD, Hoos A, ODay S, et al. Guidelines for the evaluation
of immune therapy activity in solid tumors: immune-related
response criteria. Clin Cancer Res 2009; 15: 741220.
Hoos A. Evolution of end points for cancer immunotherapy trials.
Ann Oncol 2012; 23 (suppl 8): viii 4752.
Beer TM, Bernstein GT, Corman JM, et al. Randomized trial of
autologous cellular immunotherapy with sipuleucel-T in androgendependent prostate cancer. Clin Cancer Res 2011; 17: 455867.
Di Lorenzo G, Buonerba C, Kanto PW. Immunotherapy for the
treatment of prostate cancer. Nat Rev Clin Oncol 2011; 8: 55161.
Stein WD, Gulley JL, Schlom J, et al. Tumor regression and growth
rates determined in ve intramural NCI prostate cancer trials:
the growth rate constant as an indicator of therapeutic ecacy.
Clin Cancer Res 2011; 17: 90717.
de Vries IJM, Lesterhuis WJ, Scharenborg NM, et al. Maturation of
dendritic cells is a prerequisite for inducing immune responses in
advanced melanoma patients. Clin Cancer Res 2003; 9: 5091100.
Okada H, Kalinski P, Ueda R, et al. Induction of CD8+ T-cell
responses against novel glioma-associated antigen peptides and
clinical activity by vaccinations with alpha-type 1 polarized dendritic
cells and polyinosinic-polycytidylic acid stabilized by lysine and
carboxymethylcellulose in patients with recurrent malignant
glioma. J Clin Oncol 2011; 29: 33036.
Carreno BM, Becker-Hapak M, Huang A, et al. IL-12p70-producing
patient DC vaccine elicits Tc1-polarized immunity. J Clin Invest
2013; 123: 338394.
77
78
79
80
81
82
83
84
85
86
87
88
89
90
91
92
93
94
95
96
97
Ueno H, Schmitt N, Klechevsky E, et al. Harnessing human
dendritic cell subsets for medicine. Immunol Rev 2010;
234: 199212.
Romano E, Rossi M, Ratzinger G, et al. Peptide-loaded Langerhans
cells, despite increased IL15 secretion and T-cell activation in vitro,
elicit antitumor T-cell responses comparable to peptide-loaded
monocyte-derived dendritic cells in vivo. Clin Cancer Res 2011;
17: 198497.
Anguille S, Lion E, Van den Bergh J, et al. Interleukin-15 dendritic
cells as vaccine candidates for cancer immunotherapy.
Hum Vaccin Immunother 2013; 9: 195661.
Boullart AC, Aarntzen EH, Verdijk P, et al. Maturation of monocytederived dendritic cells with Toll-like receptor 3 and 7/8 ligands
combined with prostaglandin E2 results in high interleukin-12
production and cell migration. Cancer Immunol Immunother 2008;
57: 158997.
Fujita M, Zhu X, Ueda R, et al. Eective immunotherapy against
murine gliomas using type 1 polarizing dendritic cells--signicant
roles of CXCL10. Cancer Res 2009; 69: 158795.
Pierret L, Wilgenhof S, Corthals J, Roelandt T, Thielemans K,
Neyns B. Correlation between prior therapeutic dendritic cell
vaccination and the outcome of patients with metastatic melanoma
treated with ipilimumab. Proc Am Soc Clin Oncol 2009;
27 (suppl): abstr e20006.
Ribas A, Comin-Anduix B, Chmielowski B, et al. Dendritic cell
vaccination combined with CTLA4 blockade in patients with
metastatic melanoma. Clin Cancer Res 2009; 15: 626776.
Hamid O, Robert C, Daud A, et al. Safety and tumor responses with
lambrolizumab (anti-PD-1) in melanoma. N Engl J Med 2013;
369: 13444.
Wolchok JD, Kluger H, Callahan MK, et al. Nivolumab plus
ipilimumab in advanced melanoma. N Engl J Med 2013;
369: 12233.
Smits EL, Ponsaerts P, Berneman ZN, Van Tendeloo VF. The use of
TLR7 and TLR8 ligands for the enhancement of cancer
immunotherapy. Oncologist 2008; 13: 85975.
Whiteside TL. Inhibiting the inhibitors: evaluating agents targeting
cancer immunosuppression. Expert Opin Biol Ther 2010;
10: 101935.
Shimizu K, Fields RC, Giedlin M, Mul JJ. Systemic administration
of interleukin 2 enhances the therapeutic ecacy of dendritic
cell-based tumor vaccines. Proc Natl Acad Sci USA 1999;
96: 226873.
Escobar A, Lpez M, Serrano A, et al. Dendritic cell immunizations
alone or combined with low doses of interleukin-2 induce specic
immune responses in melanoma patients. Clin Exp Immunol 2005;
142: 55568.
Redman BG, Chang AE, Whiteld J, et al. Phase Ib trial assessing
autologous, tumor-pulsed dendritic cells as a vaccine administered
with or without IL-2 in patients with metastatic melanoma.
J Immunother 2008; 31: 59198.
Mirza N, Fishman M, Fricke I, et al. All-trans-retinoic acid improves
dierentiation of myeloid cells and immune response in cancer
patients. Cancer Res 2006; 66: 9299307.
Zitvogel L, Apetoh L, Ghiringhelli F, Andr F, Tesniere A,
Kroemer G. The anticancer immune response: indispensable for
therapeutic success? J Clin Invest 2008; 118: 19912001.
Ridol L, Petrini M, Granato AM, et al. Low-dose temozolomide
before dendritic-cell vaccination reduces (specically)
CD4+CD25++Foxp3+ regulatory T-cells in advanced melanoma
patients. J Transl Med 2013; 11: 135.
Chen G, Emens LA. Chemoimmunotherapy: reengineering
tumor immunity. Cancer Immunol Immunother 2013;
62: 20316.
Wang LX, Li R, Yang G, et al. Interleukin-7-dependent expansion
and persistence of melanoma-specic T cells in lymphodepleted
mice lead to tumor regression and editing. Cancer Res 2005;
65: 1056977.
Kandalaft LE, Powell DJ Jr, Chiang CL, et al. Autologous lysatepulsed dendritic cell vaccination followed by adoptive transfer of
vaccine-primed ex vivo co-stimulated T cells in recurrent ovarian
cancer. OncoImmunology 2013; 2: e22664.
Schlom J. Therapeutic cancer vaccines: current status and moving
forward. J Natl Cancer Inst 2012; 104: 599613.
www.thelancet.com/oncology Vol 15 June 2014
Review
98
99
100
101
102
103
104
105
106
107
108
109
Jacobs JF, Nierkens S, Figdor CG, de Vries IJ, Adema GJ.
Regulatory T cells in melanoma: the nal hurdle towards eective
immunotherapy? Lancet Oncol 2012; 13: e3242.
Jacobs JF, Punt CJ, Lesterhuis WJ, et al. Dendritic cell vaccination
in combination with anti-CD25 monoclonal antibody treatment:
a phase I/II study in metastatic melanoma patients. Clin Cancer Res
2010; 16: 506778.
Dannull J, Su Z, Rizzieri D, et al. Enhancement of vaccine-mediated
antitumor immunity in cancer patients after depletion of regulatory
T cells. J Clin Invest 2005; 115: 362333.
Morse MA, Hobeika AC, Osada T, et al. Depletion of human
regulatory T cells specically enhances antigen-specic immune
responses to cancer vaccines. Blood 2008; 112: 61018.
Baur AS, Lutz MB, Schierer S, et al. Denileukin diftitox (ONTAK)
induces a tolerogenic phenotype in dendritic cells and stimulates
survival of resting Treg. Blood 2013; 122: 218594.
Yamada Y, Aoyama A, Tocco G, et al. Dierential eects of
denileukin diftitox IL-2 immunotoxin on NK and regulatory T cells
in nonhuman primates. J Immunol 2012; 188: 606370.
Radojcic V, Bezak KB, Skarica M, et al. Cyclophosphamide resets
dendritic cell homeostasis and enhances antitumor immunity
through eects that extend beyond regulatory T cell elimination.
Cancer Immunol Immunother 2010; 59: 13748.
Heine A, Held SA, Bringmann A, Holderried TA, Brossart P.
Immunomodulatory eects of anti-angiogenic drugs. Leukemia
2011; 25: 899905.
Sakamaki I, Kwak LW, Cha SC, et al. Lenalidomide enhances the
protective eect of a therapeutic vaccine and reverses immune
suppression in mice bearing established lymphomas. Leukemia
2014; 28: 32937.
Najjar YG, Finke JH. Clinical perspectives on targeting of myeloid
derived suppressor cells in the treatment of cancer. Front Oncol
2013; 3: 49.
Poschke I, Mao Y, Adamson L, Salazar-Onfray F, Masucci G,
Kiessling R. Myeloid-derived suppressor cells impair the quality of
dendritic cell vaccines. Cancer Immunol Immunother 2012;
61: 82738.
Fujita M, Kohanbash G, Fellows-Mayle W, et al. COX-2 blockade
suppresses gliomagenesis by inhibiting myeloid-derived suppressor
cells. Cancer Res 2011; 71: 266474.
www.thelancet.com/oncology Vol 15 June 2014
110 Schilling B, Sucker A, Griewank K, et al. Vemurafenib reverses
immunosuppression by myeloid derived suppressor cells.
Int J Cancer 2013; 133: 165363.
111 Knight DA, Ngiow SF, Li M, et al. Host immunity contributes to the
anti-melanoma activity of BRAF inhibitors. J Clin Invest 2013;
123: 137181.
112 Ott PA, Henry T, Baranda SJ, et al. Inhibition of both BRAF and
MEK in BRAF(V600E) mutant melanoma restores compromised
dendritic cell (DC) function while having dierential direct eects
on DC properties. Cancer Immunol Immunother 2013; 62: 81122.
113 Gulley JL, Madan RA, Schlom J. Impact of tumour volume on the
potential ecacy of therapeutic vaccines. Curr Oncol 2011;
18: e15057.
114 Van Tendeloo VF, Van de Velde A, Van Driessche A, et al. Induction
of complete and molecular remissions in acute myeloid leukemia
by Wilms tumor 1 antigen-targeted dendritic cell vaccination.
Proc Natl Acad Sci USA 2010; 107: 1382429.
115 Anguille S, Willemen Y, Lion E, Smits EL, Berneman ZN. Dendritic
cell vaccination in acute myeloid leukemia. Cytotherapy 2012;
14: 64756.
116 Gabrilovich DI. Combination of chemotherapy and immunotherapy
for cancer: a paradigm revisited. Lancet Oncol 2007; 8: 23.
117 Wheeler CJ, Das A, Liu G, Yu JS, Black KL. Clinical responsiveness
of glioblastoma multiforme to chemotherapy after vaccination.
Clin Cancer Res 2004; 10: 531626.
118 Bracci L, Schiavoni G, Sistigu A, Belardelli F. Immune-based
mechanisms of cytotoxic chemotherapy: implications for the design
of novel and rationale-based combined treatments against cancer.
Cell Death Dier 2014; 21: 1525.
119 Aragon-Ching JB, Williams KM, Gulley JL. Impact of androgendeprivation therapy on the immune system: implications for
combination therapy of prostate cancer. Front Biosci 2007;
12: 495771.
120 Kalbasi A, June CH, Haas N, Vapiwala N. Radiation and
immunotherapy: a synergistic combination. J Clin Invest 2013;
123: 275663.
e267
Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- 1 PBDokument9 Seiten1 PBnabila noorNoch keine Bewertungen
- Neeman Presentation On OncologyDokument20 SeitenNeeman Presentation On Oncologyjlduorah7118100% (1)
- Postmenopausal BleedingDokument36 SeitenPostmenopausal BleedingANJU S BNoch keine Bewertungen
- Cancer EpidemiologyDokument80 SeitenCancer EpidemiologyLuckyme5Noch keine Bewertungen
- Immunotherapy For Non-Small Cell Lung CancerDokument6 SeitenImmunotherapy For Non-Small Cell Lung CancerFarhulNoch keine Bewertungen
- Surgery in Hymoma and MGDokument11 SeitenSurgery in Hymoma and MGHeru SigitNoch keine Bewertungen
- Cobalt-60 Vs LinacDokument33 SeitenCobalt-60 Vs LinacAnisza OkseliaNoch keine Bewertungen
- New Microsoft Word DocumentDokument6 SeitenNew Microsoft Word DocumentEklabya ChhetriNoch keine Bewertungen
- Major R Cance Er Miles Stones: Overvie EwDokument14 SeitenMajor R Cance Er Miles Stones: Overvie Ewtkobosz4877Noch keine Bewertungen
- EwingDokument10 SeitenEwingMd Ahsanuzzaman PinkuNoch keine Bewertungen
- Benign Tumor Malignant Tumor: Ms. Sneha Sehrawat AIIMS RishikeshDokument37 SeitenBenign Tumor Malignant Tumor: Ms. Sneha Sehrawat AIIMS RishikeshRajaNoch keine Bewertungen
- TXIT Exam PDFDokument155 SeitenTXIT Exam PDFcnn90Noch keine Bewertungen
- NMSCDokument50 SeitenNMSCBladimir Rodríguez LechtigNoch keine Bewertungen
- Group 10-Breast CancerDokument39 SeitenGroup 10-Breast CancerShiangNoch keine Bewertungen
- Endometrial CancerDokument34 SeitenEndometrial CancertyasdwiarumNoch keine Bewertungen
- Uk Guidelines SarcomaDokument21 SeitenUk Guidelines Sarcomachu_chiang_3Noch keine Bewertungen
- CancerDokument25 SeitenCancerItemba OnyinyechukwuNoch keine Bewertungen
- Brochure 2021Dokument114 SeitenBrochure 2021Maurizio MarchettiNoch keine Bewertungen
- Granules Speciality PDFDokument2 SeitenGranules Speciality PDFMadhavi VutukuruNoch keine Bewertungen
- Pancreaticcancer 150917114601 Lva1 App6891Dokument25 SeitenPancreaticcancer 150917114601 Lva1 App6891enam professorNoch keine Bewertungen
- Vimentin Positive Gastric Adenocarcinoma Arising in A Hyperplastic PolypDokument6 SeitenVimentin Positive Gastric Adenocarcinoma Arising in A Hyperplastic Polypkatherine albujaNoch keine Bewertungen
- Internatinal 1Dokument5 SeitenInternatinal 1daffunkmadansyahNoch keine Bewertungen
- REPORTING CERVICAL CYTOLOGY, The Bethesda SystemDokument3 SeitenREPORTING CERVICAL CYTOLOGY, The Bethesda SystemNgotelo FunwiNoch keine Bewertungen
- Resume - Taraneh Sadeghian HaghighiDokument3 SeitenResume - Taraneh Sadeghian Haghighiarian tejaratNoch keine Bewertungen
- Periarterial Divestment in Pancreatic Cancer SurgeryDokument7 SeitenPeriarterial Divestment in Pancreatic Cancer SurgeryMatias Jurado ChaconNoch keine Bewertungen
- Retromolar Embryonal Rhabdomyosarcoma: A CaseDokument6 SeitenRetromolar Embryonal Rhabdomyosarcoma: A CaseNabila RizkikaNoch keine Bewertungen
- Giant Cell Tumor: Books and Links Used For Presentation: - Robins and Cotran Book of Pathology. - AmbossDokument5 SeitenGiant Cell Tumor: Books and Links Used For Presentation: - Robins and Cotran Book of Pathology. - Ambosszaina9tariqNoch keine Bewertungen
- Robotic Prostate Cancer Surgery - Advanced TechnologyDokument8 SeitenRobotic Prostate Cancer Surgery - Advanced TechnologyindiacarezNoch keine Bewertungen
- Cancer Disease by SlidesgoDokument41 SeitenCancer Disease by SlidesgodeyaNoch keine Bewertungen
- Proceedins - Book - First ASPIC International Conference, The Portuguese Association of Cancer ResearchDokument129 SeitenProceedins - Book - First ASPIC International Conference, The Portuguese Association of Cancer ResearchAnaMRebeloNoch keine Bewertungen