Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- File 02 PDFDokument107 SeitenFile 02 PDFWaqar DarNoch keine Bewertungen
- Flow Chart For The Process of Domestic Gas ConnectionDokument1 SeiteFlow Chart For The Process of Domestic Gas ConnectionWaqar DarNoch keine Bewertungen
- List of Voters 2014-15Dokument74 SeitenList of Voters 2014-15Waqar DarNoch keine Bewertungen
- 100 Question - FPM - Summer19 - KEYDokument14 Seiten100 Question - FPM - Summer19 - KEYWaqar DarNoch keine Bewertungen
- Epaper - EPaperDokument1 SeiteEpaper - EPaperWaqar DarNoch keine Bewertungen
- Resource ID Resource Description Unit of Measure Resource TypeDokument4 SeitenResource ID Resource Description Unit of Measure Resource TypeWaqar DarNoch keine Bewertungen
- Quality Audit Plan - SNGPL: Purpose: Audit Scope: Audit TeamDokument2 SeitenQuality Audit Plan - SNGPL: Purpose: Audit Scope: Audit TeamWaqar DarNoch keine Bewertungen
- Process Groups PMBOKDokument1 SeiteProcess Groups PMBOKWaqar DarNoch keine Bewertungen
- Time and Motion StudyDokument25 SeitenTime and Motion StudyWaqar DarNoch keine Bewertungen
- Sample Aptitude TestDokument40 SeitenSample Aptitude TestWaqar DarNoch keine Bewertungen
- Primavera Project Planner P6 Assignment No. 1:: Bahria University, Lahore Campus (BULC)Dokument4 SeitenPrimavera Project Planner P6 Assignment No. 1:: Bahria University, Lahore Campus (BULC)Waqar DarNoch keine Bewertungen
- Primavera Project Planner P6 Homework No. 1:: Submitted ToDokument5 SeitenPrimavera Project Planner P6 Homework No. 1:: Submitted ToWaqar DarNoch keine Bewertungen
- Wa0018Dokument4 SeitenWa0018Waqar DarNoch keine Bewertungen
- Project Brief: Bahria University, Lahore Campus (BULC)Dokument3 SeitenProject Brief: Bahria University, Lahore Campus (BULC)Waqar DarNoch keine Bewertungen
- 1 Lecture Hours, 1 Recitation Hour, 1 Semester Hour Credit.: ENGR 300 Dr. Tarek SobhDokument1 Seite1 Lecture Hours, 1 Recitation Hour, 1 Semester Hour Credit.: ENGR 300 Dr. Tarek SobhWaqar DarNoch keine Bewertungen
- Solid RodDokument14 SeitenSolid RodWaqar DarNoch keine Bewertungen
- Internal Inspection Checklist - Fire Tube Boiler PDFDokument2 SeitenInternal Inspection Checklist - Fire Tube Boiler PDFWaqar Dar100% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- 9.16. Prepare A Plot of Work Per Pound Mole Versus The Pressue Ratio PDokument6 Seiten9.16. Prepare A Plot of Work Per Pound Mole Versus The Pressue Ratio PttussenoNoch keine Bewertungen
- Bsee201 B - Fluid MechanicsDokument150 SeitenBsee201 B - Fluid MechanicsMarvin GagarinNoch keine Bewertungen
- L1F1Dokument5 SeitenL1F1DanielNoch keine Bewertungen
- Civil Engineering PDFDokument3 SeitenCivil Engineering PDFchetan c patilNoch keine Bewertungen
- Hindalco Aluminium Catalogue PDFDokument4 SeitenHindalco Aluminium Catalogue PDFVansu Saini0% (1)
- VNX Unified Storage ManagementDokument3 SeitenVNX Unified Storage ManagementNicoleNoch keine Bewertungen
- Hayward Super II Pump Model SP3005X7 ManualDokument14 SeitenHayward Super II Pump Model SP3005X7 ManualhsmerkelNoch keine Bewertungen
- Bosch Powerpack-BrochureDokument16 SeitenBosch Powerpack-BrochurengazawooNoch keine Bewertungen
- Fracture in Concrete and Reinforced ConcreteDokument23 SeitenFracture in Concrete and Reinforced ConcreteNilay GandhiNoch keine Bewertungen
- Tools of BiotechnologyDokument10 SeitenTools of Biotechnologyiamforu1Noch keine Bewertungen
- Saurabh ShrivastavaDokument37 SeitenSaurabh ShrivastavaMahendraNoch keine Bewertungen
- Debug 1214Dokument3 SeitenDebug 1214Pandji AsmaraNoch keine Bewertungen
- PDFDokument255 SeitenPDFwrite2arshad_mNoch keine Bewertungen
- Bloor Research On Data MigrationDokument13 SeitenBloor Research On Data MigrationivahdamNoch keine Bewertungen
- 02 - Student Lesson 2 Pile Driving SystemDokument91 Seiten02 - Student Lesson 2 Pile Driving SystemdannyzuanNoch keine Bewertungen
- Carpentry: Exploratory CourseDokument25 SeitenCarpentry: Exploratory CourseJohn Nelson Picones100% (3)
- Mitsubishi 4g13 Engine ManualDokument6 SeitenMitsubishi 4g13 Engine ManualJose Luis Caceres Severino100% (1)
- DNF Stand PipeDokument3 SeitenDNF Stand PipeChristopher BrownNoch keine Bewertungen
- RDSL 993K Z4D - Z4ZDokument11 SeitenRDSL 993K Z4D - Z4ZDAnielNoch keine Bewertungen
- Pace Power System Presentation - 0Dokument15 SeitenPace Power System Presentation - 0everetteNoch keine Bewertungen
- Gsk980Tda Turning Machine CNC System: CharacteristicsDokument10 SeitenGsk980Tda Turning Machine CNC System: CharacteristicsPramod YadavNoch keine Bewertungen
- WinDNC - V05 - 02 English PDFDokument2 SeitenWinDNC - V05 - 02 English PDFAnonymous XXKCjKnc0Noch keine Bewertungen
- Aurora: AE MC-120 SeriesDokument2 SeitenAurora: AE MC-120 SeriestasoNoch keine Bewertungen
- Brickwork ApparatusDokument4 SeitenBrickwork ApparatusRoslie AbdullahNoch keine Bewertungen
- Method Statement of Pipeline WorksDokument13 SeitenMethod Statement of Pipeline Worksमनिसभेटुवाल86% (21)
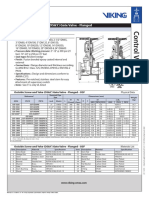
- Outside Screw and Yoke (OS&Y) Gate Valve - Flanged: Technical FeaturesDokument2 SeitenOutside Screw and Yoke (OS&Y) Gate Valve - Flanged: Technical FeaturesMark Louie GuintoNoch keine Bewertungen
- Caustic CrackingDokument17 SeitenCaustic CrackingDurga PrasadNoch keine Bewertungen
- Manual PSW 2600Dokument18 SeitenManual PSW 2600Jc C. GomezNoch keine Bewertungen
- While Start Drive Test Learning, You Must Know The Basic Things! These All Conotents Are at Introductory LevelDokument15 SeitenWhile Start Drive Test Learning, You Must Know The Basic Things! These All Conotents Are at Introductory LevelRakesh SolankiNoch keine Bewertungen
- Machine Safeguarding at The Point of Operation: A Guide For Finding Solutions To Machine HazardsDokument60 SeitenMachine Safeguarding at The Point of Operation: A Guide For Finding Solutions To Machine HazardsYovanyCalPadillaNoch keine Bewertungen