Das könnte Ihnen auch gefallen
- 2010 PPS Guidelines On DengueDokument15 Seiten2010 PPS Guidelines On DengueAguilar JehuNoch keine Bewertungen
- CPG Dengue - PaediatricDokument28 SeitenCPG Dengue - PaediatricTzeyong FooNoch keine Bewertungen
- National Guidelines On Management of Dengue Fever & Dengue Haemorrhagic Fever in Adults - Sri LankaDokument49 SeitenNational Guidelines On Management of Dengue Fever & Dengue Haemorrhagic Fever in Adults - Sri LankaNational Dengue Control Unit,Sri LankaNoch keine Bewertungen
- Cpm15th Dengue Fever (Doh)Dokument18 SeitenCpm15th Dengue Fever (Doh)Marko ParungoNoch keine Bewertungen
- National Guidelines On Management of Dengue Fever & Dengue Haemorrhagic Fever in Children and Adolescents - Sri LankaDokument53 SeitenNational Guidelines On Management of Dengue Fever & Dengue Haemorrhagic Fever in Children and Adolescents - Sri LankaNational Dengue Control Unit,Sri Lanka100% (1)
- Pang Et Al 2014Dokument11 SeitenPang Et Al 2014paiskopaxiew888Noch keine Bewertungen
- PCH 32 s1 033Dokument6 SeitenPCH 32 s1 033dydy_7193Noch keine Bewertungen
- Guidelines For The Management of DF and DHF in AdultsDokument46 SeitenGuidelines For The Management of DF and DHF in AdultsNanda SulistyaningrumNoch keine Bewertungen
- CPG Management of Dengue Infection in Adults (Revised 2nd Edition)Dokument68 SeitenCPG Management of Dengue Infection in Adults (Revised 2nd Edition)umiraihana1Noch keine Bewertungen
- Management of - Dengue Fever in ChildrenDokument27 SeitenManagement of - Dengue Fever in Childrenumiraihana1Noch keine Bewertungen
- Management of Dengue Fever in Children PDFDokument41 SeitenManagement of Dengue Fever in Children PDFnakalnakal2015Noch keine Bewertungen
- Dengue How ClassifyDokument5 SeitenDengue How ClassifyErlin IrawatiNoch keine Bewertungen
- Dengue GCP GuidelinesDokument127 SeitenDengue GCP GuidelinesShafiq AhmadNoch keine Bewertungen
- Dengue ClassificationDokument11 SeitenDengue ClassificationzhafranNoch keine Bewertungen
- 2020 Cde Algorithms Dengue Regional enDokument16 Seiten2020 Cde Algorithms Dengue Regional endr FaisalNoch keine Bewertungen
- Algorithms For The Clinical Management of Dengue Patients (2020)Dokument16 SeitenAlgorithms For The Clinical Management of Dengue Patients (2020)Charlie CharcapeNoch keine Bewertungen
- JBB2012 151967Dokument13 SeitenJBB2012 151967Prodia Central Java RegionNoch keine Bewertungen
- Cpm15th Dengue Fever (Doh)Dokument18 SeitenCpm15th Dengue Fever (Doh)Jeanne Marie ValesNoch keine Bewertungen
- Dengue Fever Journal 1Dokument10 SeitenDengue Fever Journal 1aurazhavaNoch keine Bewertungen
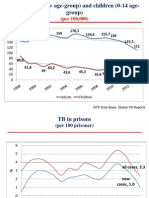
- NTP Data Base. Global TB ReportsDokument36 SeitenNTP Data Base. Global TB ReportsComingSoonNoch keine Bewertungen
- Anak Bu HeniDokument10 SeitenAnak Bu HeniVeronika IntanNoch keine Bewertungen
- Manual of Procedures NTP 5th EditionDokument172 SeitenManual of Procedures NTP 5th EditionMercuryCas100% (3)
- 2016 Article 1849 PDFDokument8 Seiten2016 Article 1849 PDFdydy_7193Noch keine Bewertungen
- 4550 16204 1 PBDokument7 Seiten4550 16204 1 PBKhoirunisah Dwi HartantiNoch keine Bewertungen
- Dengue Guideline 082012 Edit UmyDokument47 SeitenDengue Guideline 082012 Edit UmyFarika NorNoch keine Bewertungen
- Case Definitions For Infectious Diseases in Malaysia 2nd Edition Jan 2006Dokument110 SeitenCase Definitions For Infectious Diseases in Malaysia 2nd Edition Jan 2006Veronica Vivi67% (3)
- PCAP UpdatesDokument60 SeitenPCAP UpdatesMarko ParungoNoch keine Bewertungen
- COVID-19: Who To Test and When? CME / ABIM MOC / CEDokument6 SeitenCOVID-19: Who To Test and When? CME / ABIM MOC / CELuis Henrique SalesNoch keine Bewertungen
- TRZ 068Dokument8 SeitenTRZ 068salsabilapraninditaNoch keine Bewertungen
- 671 - Rhinosinusitis and Nasal Polyps (CompleteDokument89 Seiten671 - Rhinosinusitis and Nasal Polyps (CompleteAprilla Handayani100% (1)
- 2nd Edition of Malaysian COPD Clinical Practice GuidelineDokument67 Seiten2nd Edition of Malaysian COPD Clinical Practice GuidelineFay Fanny FlanneryNoch keine Bewertungen
- National Tuberculosis Program MOPDokument192 SeitenNational Tuberculosis Program MOPlpanatalioNoch keine Bewertungen
- Definitive Tests For Dengue Fever When and Which SDokument5 SeitenDefinitive Tests For Dengue Fever When and Which SAlone EvensNoch keine Bewertungen
- Managemant Copd CPG MsiaDokument67 SeitenManagemant Copd CPG MsiaNur Anis ZarimeNoch keine Bewertungen
- TB Treatment Advances in GeorgiaDokument31 SeitenTB Treatment Advances in GeorgiaComingSoonNoch keine Bewertungen
- NTCP MOP 5e FinalDokument192 SeitenNTCP MOP 5e FinalcharmainegoNoch keine Bewertungen
- Revealed That: Among New and Among Re-Treatment TB Cases Had MDR-TBDokument32 SeitenRevealed That: Among New and Among Re-Treatment TB Cases Had MDR-TBComingSoonNoch keine Bewertungen
- TB Bahasa 11-15Dokument5 SeitenTB Bahasa 11-15MomonNoch keine Bewertungen
- Dengue ThesisDokument5 SeitenDengue ThesisPat Vierneza-Calalang100% (2)
- 14.Cpg Dengue Fever in ChildrenDokument27 Seiten14.Cpg Dengue Fever in ChildrenFaridahNoch keine Bewertungen
- Living on the Frontline of COVID-19 in MCO And CMCOVon EverandLiving on the Frontline of COVID-19 in MCO And CMCONoch keine Bewertungen
- Virologic Failure in HIV: An Updated Clinician’s Guide to Assessment and ManagementVon EverandVirologic Failure in HIV: An Updated Clinician’s Guide to Assessment and ManagementNoch keine Bewertungen
- Diagnosis and Treatment of Chronic CoughVon EverandDiagnosis and Treatment of Chronic CoughSang Heon ChoNoch keine Bewertungen
- Living on the Frontline of COVID-19 in MCO And CMCO: Clinical Updates in COVID-19Von EverandLiving on the Frontline of COVID-19 in MCO And CMCO: Clinical Updates in COVID-19Noch keine Bewertungen
- Guidance for COVID-19: Prevention, Control, Diagnosis and ManagementVon EverandGuidance for COVID-19: Prevention, Control, Diagnosis and ManagementNoch keine Bewertungen
- Optimizing Advanced Therapies in Ulcerative Colitis: Is Your Practice Up to Date? A Focus on Clinical Evidence and Guideline RecommendationsVon EverandOptimizing Advanced Therapies in Ulcerative Colitis: Is Your Practice Up to Date? A Focus on Clinical Evidence and Guideline RecommendationsNoch keine Bewertungen
- COVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19Von EverandCOVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19Noch keine Bewertungen
- Atopic Dermatitis: New Perspectives on Managing a Chronic Inflammatory DiseaseVon EverandAtopic Dermatitis: New Perspectives on Managing a Chronic Inflammatory DiseaseBewertung: 5 von 5 Sternen5/5 (1)
- Influenza vaccination: What does the scientific proof say?: Could it be more harmful than useful to vaccinate indiscriminately elderly people, pregnant women, children and health workers?Von EverandInfluenza vaccination: What does the scientific proof say?: Could it be more harmful than useful to vaccinate indiscriminately elderly people, pregnant women, children and health workers?Noch keine Bewertungen
- Long Covid - The Long Covid Book for Clinicians and Sufferers - Away from Despair and Towards UnderstandingVon EverandLong Covid - The Long Covid Book for Clinicians and Sufferers - Away from Despair and Towards UnderstandingNoch keine Bewertungen
- Clinical Updates in the Management of Severe Asthma: New Strategies for Individualizing Long-term CareVon EverandClinical Updates in the Management of Severe Asthma: New Strategies for Individualizing Long-term CareNoch keine Bewertungen
- Nursing care process in patients with chronic obstructive pulmonary diseaseVon EverandNursing care process in patients with chronic obstructive pulmonary diseaseNoch keine Bewertungen
- Management of Tuberculosis: A guide for clinicians (eBook edition)Von EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)Noch keine Bewertungen
- Beyond One Health: From Recognition to ResultsVon EverandBeyond One Health: From Recognition to ResultsJohn A. HerrmannNoch keine Bewertungen
- Fundamental Aspects of Infection Prevention and ControlVon EverandFundamental Aspects of Infection Prevention and ControlNoch keine Bewertungen
- Dr. BoenDokument81 SeitenDr. BoenOktavian Rizki IlahiNoch keine Bewertungen
- Brosur Organization ProfileDokument5 SeitenBrosur Organization ProfileOktavian Rizki IlahiNoch keine Bewertungen
- Kumpulan Resep Obat OsceDokument62 SeitenKumpulan Resep Obat OsceOktavian Rizki Ilahi100% (2)
- NefrolitiasisDokument45 SeitenNefrolitiasisOktavian Rizki IlahiNoch keine Bewertungen
- Diagnostic and Management Approach of Bardycardia - DR - YuliDokument35 SeitenDiagnostic and Management Approach of Bardycardia - DR - YuliOktavian Rizki IlahiNoch keine Bewertungen
- Urinary Stone SurgeryDokument20 SeitenUrinary Stone SurgeryOktavian Rizki IlahiNoch keine Bewertungen
- Patologi Klinik Kelainan GinjalDokument21 SeitenPatologi Klinik Kelainan GinjalOktavian Rizki IlahiNoch keine Bewertungen
- Indikasi Bedah Pada StrokeDokument41 SeitenIndikasi Bedah Pada StrokeOktavian Rizki IlahiNoch keine Bewertungen
- Clinical Aspects of Benign and Malignant Soft TissueDokument68 SeitenClinical Aspects of Benign and Malignant Soft TissueOktavian Rizki IlahiNoch keine Bewertungen
- Diarrhea and DehydrationDokument27 SeitenDiarrhea and DehydrationOktavian Rizki IlahiNoch keine Bewertungen
- Diare Dan DehidrasiDokument61 SeitenDiare Dan DehidrasiOktavian Rizki IlahiNoch keine Bewertungen
- English Revision Notes XIIDokument41 SeitenEnglish Revision Notes XIIRämíz MêmóñNoch keine Bewertungen
- Audit ChecklistDokument21 SeitenAudit ChecklistRob WillestoneNoch keine Bewertungen
- Holistic Retreat, Doi Saket, Chiang MaiDokument4 SeitenHolistic Retreat, Doi Saket, Chiang MaiShireenNoch keine Bewertungen
- 5 All India Mobile Database SampleDokument15 Seiten5 All India Mobile Database Sampleali khan Saifi100% (1)
- Kerala University of Health Sciences Faculty of Dentistry BDS Course Regulations and Syllabus 2010Dokument125 SeitenKerala University of Health Sciences Faculty of Dentistry BDS Course Regulations and Syllabus 2010Shyam KrishnanNoch keine Bewertungen
- Handout 2Dokument3 SeitenHandout 2Cale CynthiaNoch keine Bewertungen
- SLM125Dokument5 SeitenSLM125k2kkhanna105Noch keine Bewertungen
- Earned Value Management Systems ANSI/EIA-748-C Intent GuideDokument59 SeitenEarned Value Management Systems ANSI/EIA-748-C Intent Guidekarditobambang23Noch keine Bewertungen
- FMFM 1-ADokument35 SeitenFMFM 1-AcvbnNoch keine Bewertungen
- PR Out of Nothing by Kate BurvillDokument11 SeitenPR Out of Nothing by Kate BurvillCulture Comms0% (1)
- BengzonDokument5 SeitenBengzonmceline19Noch keine Bewertungen
- Periodical Exam Science 9Dokument2 SeitenPeriodical Exam Science 9Jhey EmNoch keine Bewertungen
- The Lair of Arachas - A Mausritter AdventureDokument8 SeitenThe Lair of Arachas - A Mausritter AdventureGladstone PinheiroNoch keine Bewertungen
- FNHA First Nations Health Benefits Mental Health Provider ListDokument17 SeitenFNHA First Nations Health Benefits Mental Health Provider ListJoel PanganibanNoch keine Bewertungen
- Minutes of Meeting 12-09-17Dokument3 SeitenMinutes of Meeting 12-09-17MykaNoch keine Bewertungen
- Surviving A Zombie ApocalypseDokument4 SeitenSurviving A Zombie ApocalypseSarah SmithNoch keine Bewertungen
- Environmental Sustainability Assessment of An Academic Institution in Calamba CityDokument29 SeitenEnvironmental Sustainability Assessment of An Academic Institution in Calamba CityAmadeus Fernando M. PagenteNoch keine Bewertungen
- Mr. Doherty Builds His Dream LifeDokument32 SeitenMr. Doherty Builds His Dream LifeglacenatNoch keine Bewertungen
- Pasyon and RevolutionDokument2 SeitenPasyon and RevolutionBilly JoeNoch keine Bewertungen
- Investigation Into Failure Phenomena of Water Meter in The Kingdom of BahrainDokument118 SeitenInvestigation Into Failure Phenomena of Water Meter in The Kingdom of BahrainJabnon NonjabNoch keine Bewertungen
- Mod Is A 27112013Dokument8 SeitenMod Is A 27112013Garankuwa HiphopCommiteeNoch keine Bewertungen
- Me Desires-Erotic PoetryDokument21 SeitenMe Desires-Erotic PoetrygamahucherNoch keine Bewertungen
- 11Dokument24 Seiten11anil.gelra5140100% (1)
- FSLDMDokument5 SeitenFSLDMaiabbasi9615Noch keine Bewertungen
- Sample OMR Sheet Marking PDFDokument1 SeiteSample OMR Sheet Marking PDFMuraliNoch keine Bewertungen
- Unit 11 Multiple Correlation: StructureDokument18 SeitenUnit 11 Multiple Correlation: StructurePranav ViswanathanNoch keine Bewertungen
- Students' Perception of Online English Learning During Covid-19 PandemicDokument5 SeitenStudents' Perception of Online English Learning During Covid-19 Pandemicfadhilah santriNoch keine Bewertungen
- Customer Preferences For Restaurant Technology InnovationsDokument22 SeitenCustomer Preferences For Restaurant Technology InnovationsDeepankar SinghNoch keine Bewertungen
- Enhancing Health and Emotion: Mindfulness As A Missing Link Between Cognitive Therapy and Positive PsychologyDokument14 SeitenEnhancing Health and Emotion: Mindfulness As A Missing Link Between Cognitive Therapy and Positive PsychologyTeresa ChuecaNoch keine Bewertungen
- HF7E16HKEHDokument9 SeitenHF7E16HKEHMarc Gerald TorresNoch keine Bewertungen