Das könnte Ihnen auch gefallen
- The Impact of Whole Body Vibration Therapy On Spasticity and Disability of The Patients With Poststroke HemiplegiaDokument6 SeitenThe Impact of Whole Body Vibration Therapy On Spasticity and Disability of The Patients With Poststroke HemiplegialabsoneducationNoch keine Bewertungen
- 24 - JPTS 2012 156Dokument4 Seiten24 - JPTS 2012 156Βιβιλάκη ΓεωργίαNoch keine Bewertungen
- Impact of PNF-based Walking Exercise On A Ramp On Gait Performance of Stroke PatientsDokument4 SeitenImpact of PNF-based Walking Exercise On A Ramp On Gait Performance of Stroke PatientsCristian Florin CrasmaruNoch keine Bewertungen
- The Effects of CI Technique in PNF On The Muscle Activity, Fatigue, and Balance in Hemiplegic PatientsDokument8 SeitenThe Effects of CI Technique in PNF On The Muscle Activity, Fatigue, and Balance in Hemiplegic PatientsIsaias AlmeidaNoch keine Bewertungen
- PNF 22 The Effects of PNF and Trunk Stabilization Robot Training On Trunk Stability and Balance in Patients With Chronic StrokeDokument11 SeitenPNF 22 The Effects of PNF and Trunk Stabilization Robot Training On Trunk Stability and Balance in Patients With Chronic StrokeAnonymous j0xAgHs3Noch keine Bewertungen
- Neuromuscular Training in PFPS Protocol BMC 2014Dokument10 SeitenNeuromuscular Training in PFPS Protocol BMC 2014Michele GonçalvesNoch keine Bewertungen
- JurnalDokument8 SeitenJurnalSelingan SenjaNoch keine Bewertungen
- 9 - 5 - The Effect of Mirror Therapy On Balance Ability of Subacute Stroke Patients - Bella Syafitri PDFDokument6 Seiten9 - 5 - The Effect of Mirror Therapy On Balance Ability of Subacute Stroke Patients - Bella Syafitri PDFAkhyar FtNoch keine Bewertungen
- PNFpresentationDokument32 SeitenPNFpresentationNarkeesh ArumugamNoch keine Bewertungen
- PNF 11 The Effect of Stabilizing Reversal and Rhythmic Stabilization in PNF On Walking and Balance in Patient With StrokeDokument11 SeitenPNF 11 The Effect of Stabilizing Reversal and Rhythmic Stabilization in PNF On Walking and Balance in Patient With StrokeAnonymous j0xAgHs3Noch keine Bewertungen
- BestDokument3 SeitenBestRitika JangraNoch keine Bewertungen
- ABJS Volume 8 Issue 4 Pages 479-501Dokument23 SeitenABJS Volume 8 Issue 4 Pages 479-501Nurul Misna LestariNoch keine Bewertungen
- The immediate effects of specific-myofascial release technique versus Proprioceptive neuromuscular facilitation Hold-relax technique on hamstring flexibility in sub-acute and chronic stroke patients–An experimental studyDokument5 SeitenThe immediate effects of specific-myofascial release technique versus Proprioceptive neuromuscular facilitation Hold-relax technique on hamstring flexibility in sub-acute and chronic stroke patients–An experimental studyjerrin jacobNoch keine Bewertungen
- Ijerph 16 03509Dokument11 SeitenIjerph 16 03509Chloe BujuoirNoch keine Bewertungen
- Effect of NMES Vs Isometric Exercise in OA of Knee-With-Cover-Page-V2 Removed RemovedDokument5 SeitenEffect of NMES Vs Isometric Exercise in OA of Knee-With-Cover-Page-V2 Removed RemovedZahra SativaniNoch keine Bewertungen
- PnfpresentationDokument32 SeitenPnfpresentationCherry RipeNoch keine Bewertungen
- MPT Dissertation PPT CorrectedDokument30 SeitenMPT Dissertation PPT CorrectedPradeep Kumar BhuvaneshwaranNoch keine Bewertungen
- RPG Na Recuperação de Pacientes Com Cervicalgia PDFDokument9 SeitenRPG Na Recuperação de Pacientes Com Cervicalgia PDFHildemar ShirataNoch keine Bewertungen
- 1001Dokument12 Seiten1001Edo Orlando Galicia PinazoNoch keine Bewertungen
- A Comparison Between Two Active Stretching Techniques On Hamstrings Flexibility in Asymptomatic IndividualsDokument5 SeitenA Comparison Between Two Active Stretching Techniques On Hamstrings Flexibility in Asymptomatic IndividualsIOSRjournalNoch keine Bewertungen
- Rehabilitasi Post Op Spine Surgery: Kobal Sangaji Dokter Spesialis Rehabilitasi Medik RS Awalbros PekanbaruDokument27 SeitenRehabilitasi Post Op Spine Surgery: Kobal Sangaji Dokter Spesialis Rehabilitasi Medik RS Awalbros PekanbarukurniaNoch keine Bewertungen
- Vikranth .G .R Lawrence Mathias Mohd Meraj Ghori: BackgroundDokument8 SeitenVikranth .G .R Lawrence Mathias Mohd Meraj Ghori: BackgroundSekar AyuNoch keine Bewertungen
- Original Original Original Original Article Article Article Article 2010, 4 (1) : 41-46Dokument6 SeitenOriginal Original Original Original Article Article Article Article 2010, 4 (1) : 41-46sulis tiyowatiNoch keine Bewertungen
- Effect of Lumbar Stabilization Exercise On Disc Herniation Index, Sacral Angle, and Functional Improvement in Patients With Lumbar Disc HerniationDokument5 SeitenEffect of Lumbar Stabilization Exercise On Disc Herniation Index, Sacral Angle, and Functional Improvement in Patients With Lumbar Disc HerniationMuhammad Ridha Al JinaniNoch keine Bewertungen
- 79b6 PDFDokument5 Seiten79b6 PDFcnsatishNoch keine Bewertungen
- (Folia Medica) Rehabilitation of Patients With Hip Joint Arthroplasty (Late Post-Surgery Period Hospital Rehabilitation)Dokument5 Seiten(Folia Medica) Rehabilitation of Patients With Hip Joint Arthroplasty (Late Post-Surgery Period Hospital Rehabilitation)manuel velasquezNoch keine Bewertungen
- 23 247Dokument4 Seiten23 247Ita MagdalenaNoch keine Bewertungen
- Effects of Trunk Rehabilitation With Kinesio and Placebo TapingDokument15 SeitenEffects of Trunk Rehabilitation With Kinesio and Placebo TapingShania BaraqbahNoch keine Bewertungen
- High Load Lifting Exercise and Low Load Motor Control Exercises As Interventions For Patients With Mechanical Low Back Pain: A Randomized Controlled Trial With 24-Month Follow-UpDokument8 SeitenHigh Load Lifting Exercise and Low Load Motor Control Exercises As Interventions For Patients With Mechanical Low Back Pain: A Randomized Controlled Trial With 24-Month Follow-UpbellaNoch keine Bewertungen
- TensDokument9 SeitenTensRiri NandaNoch keine Bewertungen
- Pillastrini 2016Dokument41 SeitenPillastrini 2016alonsoNoch keine Bewertungen
- E Vects of Three Diverent Training Modalities On The Cross Sectional Area of The Lumbar Multifidus Muscle in Patients With Chronic Low Back PainDokument6 SeitenE Vects of Three Diverent Training Modalities On The Cross Sectional Area of The Lumbar Multifidus Muscle in Patients With Chronic Low Back PainGary LeeNoch keine Bewertungen
- Active Release TechniquesDokument15 SeitenActive Release TechniquesPhysiotherapist Ali100% (1)
- Task Oriented Improves Strength - Stroke PatientsDokument7 SeitenTask Oriented Improves Strength - Stroke PatientsPedro FonsecaNoch keine Bewertungen
- Kiper2015 Propio PDFDokument6 SeitenKiper2015 Propio PDFJuan Pedro BarrientosNoch keine Bewertungen
- 10 Jpts 27 1455Dokument3 Seiten10 Jpts 27 1455mustafasacarNoch keine Bewertungen
- Dharam Pani Pandey, Dr. Uday Shankar Sharma, Dr. Ram Babu. Electrical Muscle Stimulation (EMS) Improve Functional Independence in Critically Ill PatientsDokument8 SeitenDharam Pani Pandey, Dr. Uday Shankar Sharma, Dr. Ram Babu. Electrical Muscle Stimulation (EMS) Improve Functional Independence in Critically Ill PatientsDr. Krishna N. SharmaNoch keine Bewertungen
- Effectiveness of Spencer Muscle Energy Technique On Periarthritis ShoulderDokument5 SeitenEffectiveness of Spencer Muscle Energy Technique On Periarthritis Shoulderplaboni banerjeeNoch keine Bewertungen
- Aluko2013 2Dokument11 SeitenAluko2013 2Dr Ahmed NabilNoch keine Bewertungen
- PNF SimplifiedDokument3 SeitenPNF SimplifiedsaswepakNoch keine Bewertungen
- 165-Article Text-385-1-10-20190423Dokument7 Seiten165-Article Text-385-1-10-20190423Deva GeofahniNoch keine Bewertungen
- Controlled Study of Neuroprosthetic Functional Electrical Stimulation in Sub-Acute Post-Stroke RehabilitationDokument5 SeitenControlled Study of Neuroprosthetic Functional Electrical Stimulation in Sub-Acute Post-Stroke RehabilitationAiry MercadoNoch keine Bewertungen
- PTH 662 - Literature Review PaperDokument8 SeitenPTH 662 - Literature Review Paperapi-551757456Noch keine Bewertungen
- Effects of Intensive Repetition of A New Facilitation Technique On Motor Functional Recovery of The Hemiplegic Upper Limb and HandDokument13 SeitenEffects of Intensive Repetition of A New Facilitation Technique On Motor Functional Recovery of The Hemiplegic Upper Limb and Handpunit lakraNoch keine Bewertungen
- Added Value of Gluteus Medius and Quadratus Lumborum Dry Needling in Improving Knee Pain and Function in Female Athletes With Patellofemoral Pain Syndrome: A Randomized Clinical TrialDokument10 SeitenAdded Value of Gluteus Medius and Quadratus Lumborum Dry Needling in Improving Knee Pain and Function in Female Athletes With Patellofemoral Pain Syndrome: A Randomized Clinical Trialريما ميماNoch keine Bewertungen
- SciDokument9 SeitenSciCathyCarltonNoch keine Bewertungen
- 10 1016@j Physio 2019 11 002Dokument27 Seiten10 1016@j Physio 2019 11 002Milton Ricardo de Medeiros FernandesNoch keine Bewertungen
- Pasiv and ActiveDokument4 SeitenPasiv and ActiveAna wulandariNoch keine Bewertungen
- The Effect of Spinal Exercises On H-Reflex in Subjects With Lumbosacral RadiculopathyDokument5 SeitenThe Effect of Spinal Exercises On H-Reflex in Subjects With Lumbosacral RadiculopathyInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- Effectiveness of Mulligan's Mobilization Technique Versus Eccentric Exercises On Pain, Hand Grip Strength and Function in Subjects With Lateral EpicondylitisDokument8 SeitenEffectiveness of Mulligan's Mobilization Technique Versus Eccentric Exercises On Pain, Hand Grip Strength and Function in Subjects With Lateral EpicondylitisInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- Added Effect of Muscle Energy TechniqueDokument6 SeitenAdded Effect of Muscle Energy Techniquesriram gopalNoch keine Bewertungen
- To Compare The Effect of Core Stability Exercises and Muscle Energy Techniques On Low Back Pain PatientsDokument7 SeitenTo Compare The Effect of Core Stability Exercises and Muscle Energy Techniques On Low Back Pain PatientsDr Ahmed NabilNoch keine Bewertungen
- The Long-Term Effect of 2 PostoperativeDokument9 SeitenThe Long-Term Effect of 2 Postoperativeahmed K.Abd el SaterNoch keine Bewertungen
- Art 1Dokument10 SeitenArt 1ALEJANDRA GARZÓN CUELLAR.Noch keine Bewertungen
- Fulltext - SMJCM v3 1021 PDFDokument6 SeitenFulltext - SMJCM v3 1021 PDFNERS ANGKATAN 8Noch keine Bewertungen
- 1385 FullDokument10 Seiten1385 FullSetiaty PandiaNoch keine Bewertungen
- Cervical StretchingDokument5 SeitenCervical StretchingSulthan PhysioNoch keine Bewertungen
- Giray 2019Dokument13 SeitenGiray 2019Felix LoaizaNoch keine Bewertungen
- Stroke 2 RCTDokument6 SeitenStroke 2 RCTArdhyan ArdhyanNoch keine Bewertungen
- Principles of Manual Medicine for Sacroiliac Joint Dysfunction: Arthrokinematic Approach-Hakata MethodVon EverandPrinciples of Manual Medicine for Sacroiliac Joint Dysfunction: Arthrokinematic Approach-Hakata MethodShigehiko KatadaNoch keine Bewertungen
- F115a'12 Fl115a'12: (68VB) (68WB)Dokument96 SeitenF115a'12 Fl115a'12: (68VB) (68WB)AlexDiazNoch keine Bewertungen
- Relay Identification: Example CDG31FF002SACHDokument5 SeitenRelay Identification: Example CDG31FF002SACHRohit RanaNoch keine Bewertungen
- History of Journalism With Whiteboard StyleDokument56 SeitenHistory of Journalism With Whiteboard StyleXeon JupiterNoch keine Bewertungen
- NSO SPRDokument9 SeitenNSO SPRADITYA SINGHNoch keine Bewertungen
- MCQ Unit 3Dokument15 SeitenMCQ Unit 3gaur1234Noch keine Bewertungen
- NoahDokument2 SeitenNoahapi-302505193Noch keine Bewertungen
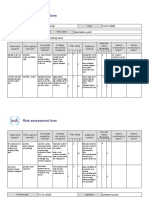
- Risk Assessment Project Iosh - MsDokument2 SeitenRisk Assessment Project Iosh - MsSanjeev Kumar75% (32)
- EDO ScriptDokument59 SeitenEDO ScriptThais Andrés JiménezNoch keine Bewertungen
- 6.m.tech-Ece-Vlsi, Vlsi Systems, Vlsi System Design (Vlsi, Vlsis, Vlsisd) r17 Course Structure & SyllabiDokument35 Seiten6.m.tech-Ece-Vlsi, Vlsi Systems, Vlsi System Design (Vlsi, Vlsis, Vlsisd) r17 Course Structure & SyllabiravibabukancharlaNoch keine Bewertungen
- Ferrozine Rapid Liquid Method Method 8147 0.009 To 1.400 MG/L Fe Pour-Thru CellDokument6 SeitenFerrozine Rapid Liquid Method Method 8147 0.009 To 1.400 MG/L Fe Pour-Thru CellCarlos Andres MedinaNoch keine Bewertungen
- Urgent Medical Device CorrectionDokument4 SeitenUrgent Medical Device CorrectionVladimir OsunaNoch keine Bewertungen
- Amendment No. 2 To AS 2047-2014 Windows and External Glazed Doors in BuildingsDokument2 SeitenAmendment No. 2 To AS 2047-2014 Windows and External Glazed Doors in BuildingsTommy AndersNoch keine Bewertungen
- Case Study Oil and Gas - PowerpointDokument8 SeitenCase Study Oil and Gas - PowerpointYaxssNoch keine Bewertungen
- Revision For The First 1 English 8Dokument6 SeitenRevision For The First 1 English 8hiidaxneee urrrmNoch keine Bewertungen
- Notes On Peck&Coyle Practical CriticismDokument10 SeitenNotes On Peck&Coyle Practical CriticismLily DameNoch keine Bewertungen
- How To Make FireworksDokument14 SeitenHow To Make FireworksLeonardo BiancoNoch keine Bewertungen
- What Is Geyi - V MairDokument31 SeitenWhat Is Geyi - V MairbodhitanNoch keine Bewertungen
- Semicounductors & Pn-Junction (Complete)Dokument47 SeitenSemicounductors & Pn-Junction (Complete)Khalid AliNoch keine Bewertungen
- VK-53 (ВК-53) Erecting Cut-Out Switch: Maintenance ManualDokument76 SeitenVK-53 (ВК-53) Erecting Cut-Out Switch: Maintenance ManualhaileNoch keine Bewertungen
- CCNP 300 410 ENARSI NetworkTUT 26 5 2021Dokument104 SeitenCCNP 300 410 ENARSI NetworkTUT 26 5 2021Olga BradyNoch keine Bewertungen
- Lesson 4Dokument10 SeitenLesson 4Nagiri MuraliNoch keine Bewertungen
- 0 Act Sunum 2020 NewwDokument58 Seiten0 Act Sunum 2020 NewwPınar AdsızNoch keine Bewertungen
- Kim, KDM, Sim, SDM PDFDokument12 SeitenKim, KDM, Sim, SDM PDFKavan Gt12Noch keine Bewertungen
- Think Before Buying: ReadingDokument1 SeiteThink Before Buying: ReadingadrianmaiarotaNoch keine Bewertungen
- Nukote Aegis SubmittalDokument112 SeitenNukote Aegis SubmittalMarco Dos Santos NevesNoch keine Bewertungen
- Häggloader 10HR-B: Atlas CopcoDokument2 SeitenHäggloader 10HR-B: Atlas CopcoHayam BaşaranNoch keine Bewertungen
- Prepared by (Hospital Pharmacist) Primary & Secondary Healthcare DepartmentDokument11 SeitenPrepared by (Hospital Pharmacist) Primary & Secondary Healthcare DepartmentwaqasNoch keine Bewertungen
- Bendable ConcreteDokument21 SeitenBendable ConcreteJulia Sebastian0% (1)
- 100% Chemical-Free Solution For Organic Farming: Where Health Is A HabitDokument2 Seiten100% Chemical-Free Solution For Organic Farming: Where Health Is A Habitamit4118Noch keine Bewertungen
- Fagor CNC 8025 - 8030Dokument255 SeitenFagor CNC 8025 - 8030alvhann_1Noch keine Bewertungen