Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Fundamentals of Occlusion: Reference: Shillingburg Funamentals of Fixed Prosthodontics, Third Edition Chapter TwoDokument44 SeitenFundamentals of Occlusion: Reference: Shillingburg Funamentals of Fixed Prosthodontics, Third Edition Chapter Twoوا إسلاماه100% (2)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- @MedicalBooksStore 2016 Self AssessmentDokument457 Seiten@MedicalBooksStore 2016 Self AssessmentSera Qua100% (3)
- Final Na PaDokument54 SeitenFinal Na PaShiara Ruth EdrosoloNoch keine Bewertungen
- Anatomy of EarDokument42 SeitenAnatomy of EarHesti hasanNoch keine Bewertungen
- SOAL BAILEY OTOLOGI: Hearing and Balance Multiple Choice QuestionsDokument12 SeitenSOAL BAILEY OTOLOGI: Hearing and Balance Multiple Choice QuestionsRowley GeoffNoch keine Bewertungen
- A To Z Orthodontics Vol 24 Orthodontic Practical NotesDokument83 SeitenA To Z Orthodontics Vol 24 Orthodontic Practical Notesdent in dentist100% (2)
- Questions ENT 2021Dokument28 SeitenQuestions ENT 2021Ranjan Prasad100% (1)
- 2 Upper Airway Disorders PDFDokument33 Seiten2 Upper Airway Disorders PDFMonica BorjaNoch keine Bewertungen
- BPPVDokument4 SeitenBPPVAndromeda AjahNoch keine Bewertungen
- Core Radiology - Head & Neck ImagingDokument106 SeitenCore Radiology - Head & Neck ImagingefqsdfqsNoch keine Bewertungen
- Student Name: - Date: - Evaluator Name: - Skill Performance Checklist: HEENT ExaminationDokument2 SeitenStudent Name: - Date: - Evaluator Name: - Skill Performance Checklist: HEENT ExaminationAji PicanteNoch keine Bewertungen
- Anastomosis Around The ScapulaDokument1 SeiteAnastomosis Around The ScapulaYusri Arif67% (3)
- CEPHalometryDokument107 SeitenCEPHalometrydisha 146jandialNoch keine Bewertungen
- Acute Otitis Media: Definition, Causes, Symptoms, TreatmentDokument3 SeitenAcute Otitis Media: Definition, Causes, Symptoms, TreatmentMalvinder Singh DhillonNoch keine Bewertungen
- Muscles of Mastication Sumana SeminarDokument68 SeitenMuscles of Mastication Sumana SeminarSumana AryaNoch keine Bewertungen
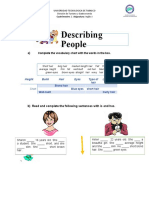
- Describing People: Complete The Vocabulary Chart With The Words in The BoxDokument2 SeitenDescribing People: Complete The Vocabulary Chart With The Words in The BoxJesus Jimenez SalomeNoch keine Bewertungen
- Med 1 - 1st Shift - Lec - HEENT Neck ExaminationDokument3 SeitenMed 1 - 1st Shift - Lec - HEENT Neck ExaminationRJLeddaNoch keine Bewertungen
- Iloilo DoctorsDokument21 SeitenIloilo DoctorsChristopher BellezaNoch keine Bewertungen
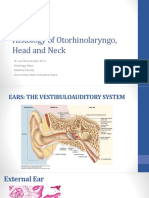
- Histologi Kepala Leher THTDokument38 SeitenHistologi Kepala Leher THTWidya ParamitaNoch keine Bewertungen
- The Ventricular SystemDokument6 SeitenThe Ventricular SystemM Arsalan TariqNoch keine Bewertungen
- Neural Control of MasticationDokument34 SeitenNeural Control of MasticationAnonymous k8rDEsJsU10% (1)
- 12 Physiology EyelidsDokument119 Seiten12 Physiology EyelidsYoussefNoch keine Bewertungen
- Notes On Eye of RabbitDokument3 SeitenNotes On Eye of RabbitShailesh NiroulaNoch keine Bewertungen
- Human DentitionDokument62 SeitenHuman DentitionWidi Marsha Fadila100% (1)
- Report (Chap 10)Dokument81 SeitenReport (Chap 10)Field StudyNoch keine Bewertungen
- Nasal Mucociliary Clearance in Adenoid Hypertrophy with or without Otitis MediaDokument4 SeitenNasal Mucociliary Clearance in Adenoid Hypertrophy with or without Otitis MediaHanifa AdaniNoch keine Bewertungen
- Senses HandoutsDokument13 SeitenSenses HandoutsxylentknightNoch keine Bewertungen
- Anatomy of Head Subs Robert Acland AnatomyDokument8 SeitenAnatomy of Head Subs Robert Acland AnatomysmohandesNoch keine Bewertungen
- Vestibular PhysiologyDokument30 SeitenVestibular PhysiologyArdiya OktamaNoch keine Bewertungen
- Good Shampo For Wavy Hair - Google SearchDokument1 SeiteGood Shampo For Wavy Hair - Google SearchJose Ajanel-SuarNoch keine Bewertungen