Das könnte Ihnen auch gefallen
- Lecture 1: Lumbar: Indirect ObjectivesDokument11 SeitenLecture 1: Lumbar: Indirect ObjectiveseugeniaNoch keine Bewertungen
- TECH 614 Full Spine I (Castellucci)Dokument10 SeitenTECH 614 Full Spine I (Castellucci)Robert StraubNoch keine Bewertungen
- Facilitated Positional Release FPRDokument12 SeitenFacilitated Positional Release FPRcoahuiltecoNoch keine Bewertungen
- Alex Brandao - MSCDokument50 SeitenAlex Brandao - MSCAlex BrandãoNoch keine Bewertungen
- CLIN 4801 Tutorials On Descriptive ListingsDokument5 SeitenCLIN 4801 Tutorials On Descriptive Listingsjoe joeNoch keine Bewertungen
- Cat 2Dokument5 SeitenCat 2Edgardo BivimasNoch keine Bewertungen
- Roods ApprochDokument59 SeitenRoods Approchsridhar_physioNoch keine Bewertungen
- Understanding The Stretch ReflexDokument2 SeitenUnderstanding The Stretch ReflexJingyan ZhangNoch keine Bewertungen
- Trigger Point: A Luc Fortesque AdventureVon EverandTrigger Point: A Luc Fortesque AdventureBewertung: 5 von 5 Sternen5/5 (1)
- Passive Scapular Adduction TestDokument15 SeitenPassive Scapular Adduction Testapi-468597987Noch keine Bewertungen
- Turocy StainCounterstrain LabPATS06ADokument53 SeitenTurocy StainCounterstrain LabPATS06Awillone08Noch keine Bewertungen
- Joint Mobilizations PDFDokument1 SeiteJoint Mobilizations PDFErik TellezNoch keine Bewertungen
- OPP Course Review: John Garlitz, DO Deborah Schmidt, DO Opp 2 April 15, 2015 8:10 AMDokument248 SeitenOPP Course Review: John Garlitz, DO Deborah Schmidt, DO Opp 2 April 15, 2015 8:10 AMmina botross100% (1)
- ManualDokument95 SeitenManualcristina_c_43Noch keine Bewertungen
- Clinical Examination of The Shoulder: Chapter Contents Referred PainDokument13 SeitenClinical Examination of The Shoulder: Chapter Contents Referred Painvein94Noch keine Bewertungen
- Pubid 1172335382Dokument9 SeitenPubid 1172335382locoproanimal0% (1)
- The Dislocated Brain: Innovation in Traumatic Brain Injury and IrrigationVon EverandThe Dislocated Brain: Innovation in Traumatic Brain Injury and IrrigationBewertung: 5 von 5 Sternen5/5 (2)
- A Unifying Neuro-Fasciagenic Model of Somatic Dysfunction e Underlying Q6 Mechanisms and Treatment e Part IIDokument19 SeitenA Unifying Neuro-Fasciagenic Model of Somatic Dysfunction e Underlying Q6 Mechanisms and Treatment e Part IITameemNoch keine Bewertungen
- Tendon Neuroplastic TrainingDokument9 SeitenTendon Neuroplastic TrainingLara VitorNoch keine Bewertungen
- Interactions between the Craniomandibular System and Cervical Spine: The influence of an unilateral change of occlusion on the upper cervical range of motionVon EverandInteractions between the Craniomandibular System and Cervical Spine: The influence of an unilateral change of occlusion on the upper cervical range of motionNoch keine Bewertungen
- Scapular-Stabilization Exercises - Early-Intervention PrescriptionDokument6 SeitenScapular-Stabilization Exercises - Early-Intervention PrescriptionJohnnySnow100% (1)
- Tissue Provocation TherapiesDokument7 SeitenTissue Provocation TherapiesdracoscribdNoch keine Bewertungen
- Temporal Sphenoidal Line T2Dokument3 SeitenTemporal Sphenoidal Line T2taichi7Noch keine Bewertungen
- ConstipationDokument22 SeitenConstipationash ash100% (1)
- Pemeriksaan SensorisDokument13 SeitenPemeriksaan SensorisDex RayNoch keine Bewertungen
- Kinetic Control Cap1Dokument17 SeitenKinetic Control Cap1Yennifer Serna MoncadaNoch keine Bewertungen
- 1400 - Still Technique For OOADokument17 Seiten1400 - Still Technique For OOAFinish Your WorkNoch keine Bewertungen
- Intro To OMT: Stacia Sloane, DODokument37 SeitenIntro To OMT: Stacia Sloane, DOJeremy100% (1)
- Peripheral Nerve Disorders & ManagementDokument60 SeitenPeripheral Nerve Disorders & ManagementJibreel Alban100% (1)
- Osteokinematics and Arthrokinematics of The Hip: Nationalfitnesscenter Ko, KwangjunDokument30 SeitenOsteokinematics and Arthrokinematics of The Hip: Nationalfitnesscenter Ko, KwangjunSai RamNoch keine Bewertungen
- Apostila de Tantsu CradleDokument10 SeitenApostila de Tantsu CradlereikianosNoch keine Bewertungen
- 2014 Helsinki Workshop Material ShacklockDokument43 Seiten2014 Helsinki Workshop Material ShacklockAl100% (1)
- Chapman S Points PDFDokument40 SeitenChapman S Points PDFPiquetaNoch keine Bewertungen
- A Simple Guide to Meniscus with Acl Injury, Diagnosis, Treatment and Related ConditionsVon EverandA Simple Guide to Meniscus with Acl Injury, Diagnosis, Treatment and Related ConditionsNoch keine Bewertungen
- 20998044B6D069 PDFDokument24 Seiten20998044B6D069 PDFjfjjfjfjjfjfNoch keine Bewertungen
- M1 Introduction To Manual TherapyDokument101 SeitenM1 Introduction To Manual TherapySylvia LoongNoch keine Bewertungen
- SBAR ExampleDokument1 SeiteSBAR Examplekellymk2584100% (1)
- Myths of The SIJ 2006Dokument14 SeitenMyths of The SIJ 2006César Alejandro Martínez RetamalNoch keine Bewertungen
- Kyusho Jitsu Alarm Points WorkshopDokument3 SeitenKyusho Jitsu Alarm Points Workshopfernando serrano reyesNoch keine Bewertungen
- Ligamentous Articular Strain - Osteopathic ManipulativeDokument20 SeitenLigamentous Articular Strain - Osteopathic Manipulativeisa_martínezNoch keine Bewertungen
- Full Spine ListingsDokument3 SeitenFull Spine ListingsMatthew DriscollNoch keine Bewertungen
- Chiropractic Line AnalysisDokument10 SeitenChiropractic Line AnalysisD N BidNoch keine Bewertungen
- BJ Palmer Clinic GenFinal CompressedDokument105 SeitenBJ Palmer Clinic GenFinal CompressedMaria Vitoria CarvalhoNoch keine Bewertungen
- PNF ConceptDokument8 SeitenPNF ConceptSolrac Adle B. SevillaNoch keine Bewertungen
- Chiropractic - in New Zealand - Report 1979Dokument398 SeitenChiropractic - in New Zealand - Report 1979vicarofskeptic100% (1)
- WWW - Chiropractic SportsDokument5 SeitenWWW - Chiropractic Sportsapi-3714923Noch keine Bewertungen
- InterX 5002 Professional - InterXClinicDokument4 SeitenInterX 5002 Professional - InterXClinicsalmazzNoch keine Bewertungen
- Osteopathy ProspectusDokument20 SeitenOsteopathy Prospectussdun7Noch keine Bewertungen
- MM SS Bruggers Seated StretchDokument1 SeiteMM SS Bruggers Seated StretchFernandoNoch keine Bewertungen
- 2014 SAAO Forum For 10-18-11 Cranial IntroDokument5 Seiten2014 SAAO Forum For 10-18-11 Cranial IntroRoger NakataNoch keine Bewertungen
- MagnetotherapyDokument42 SeitenMagnetotherapyDr.Holistic HealerNoch keine Bewertungen
- LymphaticDokument52 SeitenLymphaticlemuel_queNoch keine Bewertungen
- Terra Rosa E-Magazine No. 12Dokument33 SeitenTerra Rosa E-Magazine No. 12Terra RosaNoch keine Bewertungen
- 4th Lecture HeadNeck and LympaticsDokument77 Seiten4th Lecture HeadNeck and LympaticsJeffrey Valdez Esteron100% (1)
- Sensory ExamDokument2 SeitenSensory ExamShannen Christelle AndradeNoch keine Bewertungen
- Melatonin Biological Basis of Its Function in Health and Disease 2006 PDFDokument303 SeitenMelatonin Biological Basis of Its Function in Health and Disease 2006 PDFNoorAkNoch keine Bewertungen
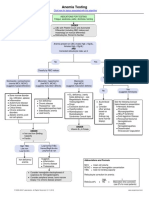
- Anemia Testing Algorithm PDFDokument1 SeiteAnemia Testing Algorithm PDFBilly AuNoch keine Bewertungen
- Weeknight Magic Vol. 1: Masha Sullivan and Anya KassoffDokument48 SeitenWeeknight Magic Vol. 1: Masha Sullivan and Anya KassoffNoorAkNoch keine Bewertungen
- 15 Minute Psych Assessment Presentation PDFDokument65 Seiten15 Minute Psych Assessment Presentation PDFUnedited revealations100% (1)
- Hydrochloric AcidDokument3 SeitenHydrochloric AcidNoorAkNoch keine Bewertungen
- Peat Therapy 2014 01 16Dokument16 SeitenPeat Therapy 2014 01 16NoorAkNoch keine Bewertungen
- Nutrition and Benign Prostatic Hyperplasia: ReviewDokument4 SeitenNutrition and Benign Prostatic Hyperplasia: ReviewNoorAkNoch keine Bewertungen
- Food Sources of IronDokument5 SeitenFood Sources of IrondogenvNoch keine Bewertungen
- 2011-Treating Clostridium Difficile Infection With Fecal Microbiota Transplantation, Fecal Microbiota Transplantation Workgroup, Clin Gastroenterol and HepDokument6 Seiten2011-Treating Clostridium Difficile Infection With Fecal Microbiota Transplantation, Fecal Microbiota Transplantation Workgroup, Clin Gastroenterol and HepNoorAkNoch keine Bewertungen
- The Faces of Low Dose Naltrexone PDFDokument116 SeitenThe Faces of Low Dose Naltrexone PDFElenaMatsnevaNoch keine Bewertungen
- Drugs Metabolized by CYP450s PDFDokument4 SeitenDrugs Metabolized by CYP450s PDFNoorAkNoch keine Bewertungen
- Chronic Fatigue Syndrome: - A Toolkit For ProvidersDokument17 SeitenChronic Fatigue Syndrome: - A Toolkit For ProvidersNoorAkNoch keine Bewertungen
- Hydrochloric AcidDokument3 SeitenHydrochloric AcidNoorAkNoch keine Bewertungen
- SIBO Summit 2016 - Key TakeawaysDokument1 SeiteSIBO Summit 2016 - Key TakeawaysNoorAkNoch keine Bewertungen
- 1 s2.0 S0306453016301482 MainDokument9 Seiten1 s2.0 S0306453016301482 MainNoorAkNoch keine Bewertungen
- BF3 Pocket Guide - Final PDFDokument88 SeitenBF3 Pocket Guide - Final PDFNoorAkNoch keine Bewertungen
- 2016 Zachariae Complementary and Alternative Medicine Use Among Patients With Cancer - A Challenge in The Oncologist-Patient RelationshipDokument2 Seiten2016 Zachariae Complementary and Alternative Medicine Use Among Patients With Cancer - A Challenge in The Oncologist-Patient RelationshipNoorAkNoch keine Bewertungen
- Sibo QuestionnaireDokument2 SeitenSibo QuestionnaireNoorAk0% (1)
- 1 s2.0 S096007601630108X MainDokument10 Seiten1 s2.0 S096007601630108X MainNoorAkNoch keine Bewertungen
- Emma 3 Week OldgirlDokument3 SeitenEmma 3 Week OldgirlNoorAkNoch keine Bewertungen
- Venipuncture and Blood Collection ExerciseDokument2 SeitenVenipuncture and Blood Collection ExerciseNoorAkNoch keine Bewertungen
- Athletic & Sport NutritionDokument2 SeitenAthletic & Sport NutritionNoorAk100% (1)
- 1 s2.0 S2213422015003170 MainDokument1 Seite1 s2.0 S2213422015003170 MainNoorAkNoch keine Bewertungen
- ASMDecFinal CompleteDokument24 SeitenASMDecFinal CompleteNoorAk100% (1)
- Basic Study TipsDokument5 SeitenBasic Study TipsNoorAkNoch keine Bewertungen
- Am J Clin Nutr 2000 Azaïs Braesco 1325s 33sDokument9 SeitenAm J Clin Nutr 2000 Azaïs Braesco 1325s 33sNoorAkNoch keine Bewertungen
- NaturoPathic Medicine Study NotesDokument13 SeitenNaturoPathic Medicine Study NotesNoorAkNoch keine Bewertungen
- 10 Rules of RepertorizationDokument3 Seiten10 Rules of RepertorizationNoorAkNoch keine Bewertungen
- The Art of Case TakingDokument41 SeitenThe Art of Case Takingasyabatool100% (2)
- Snell's Clinical Anatomy 1 - IntroductionDokument3 SeitenSnell's Clinical Anatomy 1 - IntroductionAnna Dominique Jimenez40% (5)
- Kriya - Kantha Padma Kriya: (Level One Teacher Training Manual (Old Version), Pp. 409-410)Dokument6 SeitenKriya - Kantha Padma Kriya: (Level One Teacher Training Manual (Old Version), Pp. 409-410)Moisés Jonathan Saldaña Salazar100% (1)
- Positioning and Moving of Hemiplegic Pt. Bed Mobility ExercisesDokument133 SeitenPositioning and Moving of Hemiplegic Pt. Bed Mobility Exercisesktin17100% (1)
- Biology 8 Frog Dissection GuideDokument10 SeitenBiology 8 Frog Dissection GuideRyan SantosNoch keine Bewertungen
- Horgoláshoz Kéz BemelegítésDokument1 SeiteHorgoláshoz Kéz BemelegítésKrisztaNoch keine Bewertungen
- Cardinal Points in AcupunctureDokument2 SeitenCardinal Points in Acupuncturemonicq77100% (1)
- Anatomy 1.1 - Anatomicomedical TerminologyDokument2 SeitenAnatomy 1.1 - Anatomicomedical Terminologylovelots1234Noch keine Bewertungen
- Mandarin TeachingDokument30 SeitenMandarin TeachingLai KangshengNoch keine Bewertungen
- A. Bron, R. Tripathi, B. Tripathi - Wolff's Anatomy of The Eye and Orbit-CRC Press (1998) PDFDokument724 SeitenA. Bron, R. Tripathi, B. Tripathi - Wolff's Anatomy of The Eye and Orbit-CRC Press (1998) PDFPS NI100% (1)
- Anatomy of Maxilla and Its Development - ORIGINALDokument68 SeitenAnatomy of Maxilla and Its Development - ORIGINALHoang NhanNoch keine Bewertungen
- Oblique MovementDokument1 SeiteOblique MovementBevan Low Kee0% (1)
- OIADokument8 SeitenOIACloie Anne RabinetasNoch keine Bewertungen
- Median (Third) Occipital CondyleDokument4 SeitenMedian (Third) Occipital Condylespin_echoNoch keine Bewertungen
- Muscle Palpation Assessment and Orthopedic MassageDokument3 SeitenMuscle Palpation Assessment and Orthopedic MassageAdilah ZakiyatiNoch keine Bewertungen
- Month 20 20 Months To A Champion Physique by Bill PearlDokument8 SeitenMonth 20 20 Months To A Champion Physique by Bill PearlHarsha Vardhan100% (1)
- 1.1 Human Breathing Mechanism (A)Dokument20 Seiten1.1 Human Breathing Mechanism (A)Sselvi SubramoniamNoch keine Bewertungen
- Anatomy of LarynxDokument61 SeitenAnatomy of LarynxNovianita AnggreiniNoch keine Bewertungen
- Voice ProductionDokument16 SeitenVoice ProductionAnj De Luna AlbaNoch keine Bewertungen
- Mandibular Nerve, Chorda Tympani Nerve, Otic GanglionDokument33 SeitenMandibular Nerve, Chorda Tympani Nerve, Otic Ganglionwaniya irumNoch keine Bewertungen
- Dim Mak AnatomyDokument6 SeitenDim Mak Anatomyloy7100% (6)
- Chi Kung Five Animals FrolicDokument99 SeitenChi Kung Five Animals Frolicslsbs1100% (1)
- Science Long Test Grade 1Dokument4 SeitenScience Long Test Grade 1Mitch-ChedyLanoriaNoch keine Bewertungen
- Organization of NSDokument20 SeitenOrganization of NSnadine azmyNoch keine Bewertungen
- Bab 4 Topazian, Oral and Maxillofacial Infection PDFDokument37 SeitenBab 4 Topazian, Oral and Maxillofacial Infection PDFiradatullah suyuti100% (1)
- The Pericardium Channel of Hand Jueyi NDokument5 SeitenThe Pericardium Channel of Hand Jueyi Nray72roNoch keine Bewertungen
- Anatomy-1 PDFDokument50 SeitenAnatomy-1 PDFSaransh Ghimire100% (1)
- Lumbar Plexus (Grays Anatomy)Dokument12 SeitenLumbar Plexus (Grays Anatomy)Joemar ReveloNoch keine Bewertungen
- Muscles of Upper LimbsDokument6 SeitenMuscles of Upper LimbsplanarshiftsNoch keine Bewertungen
- HEALTH ASSESSMENT (Head & Neck)Dokument38 SeitenHEALTH ASSESSMENT (Head & Neck)April Mae Magos Labrador100% (1)
- FRCR Part 1 Anatomy March 2011Dokument2 SeitenFRCR Part 1 Anatomy March 2011drramki27100% (1)