Das könnte Ihnen auch gefallen
- Valadi - Guillain-Barré SyndromeDokument5 SeitenValadi - Guillain-Barré SyndromeMarcelo BedoyaNoch keine Bewertungen
- MCQ NeuroDokument21 SeitenMCQ NeuroMasayu Mutiara UtiNoch keine Bewertungen
- Dr. Kiki Mohammad Iqbal, SPS: Departemen Neurologi FK Usu / Rsup H. Adam Malik MedanDokument35 SeitenDr. Kiki Mohammad Iqbal, SPS: Departemen Neurologi FK Usu / Rsup H. Adam Malik MedangracedumaNoch keine Bewertungen
- Guillain Barré SyndromeDokument17 SeitenGuillain Barré SyndromeMahesa RamadhiantoNoch keine Bewertungen
- Dasar-Dasar Membaca Elektroensefalografi - Gea Pandhita SDokument84 SeitenDasar-Dasar Membaca Elektroensefalografi - Gea Pandhita Sgea pandhita sNoch keine Bewertungen
- Neurologi: Lamotrigine and Baclofen 3 Line: GabapentinDokument9 SeitenNeurologi: Lamotrigine and Baclofen 3 Line: GabapentinRyan Haryana Darajatun100% (1)
- Emergency Neurological Life Support Status Epilepticus ProtocolDokument12 SeitenEmergency Neurological Life Support Status Epilepticus ProtocolFransiskus MikaelNoch keine Bewertungen
- Diagnosis Skdi Neuro NewDokument49 SeitenDiagnosis Skdi Neuro NewmerrykartikaNoch keine Bewertungen
- Acute and Chronic Chorea in Childhood: Donald L. Gilbert, MD, MSDokument6 SeitenAcute and Chronic Chorea in Childhood: Donald L. Gilbert, MD, MSKalindraParahitaNoch keine Bewertungen
- Abnormal Pupil, How To DoDokument8 SeitenAbnormal Pupil, How To DoUNHAS OphthalmologyNoch keine Bewertungen
- Motor Neuron Disease 1Dokument95 SeitenMotor Neuron Disease 1La Ode Rinaldi100% (1)
- Neurotoksikologi: DR - Sandi Lesmana, SP.SDokument48 SeitenNeurotoksikologi: DR - Sandi Lesmana, SP.Sdita anisya putriNoch keine Bewertungen
- BallismusDokument9 SeitenBallismusLee East Sea DonghaeNoch keine Bewertungen
- Large Exotropia Surgery Using Hangback TechniqueDokument10 SeitenLarge Exotropia Surgery Using Hangback TechniqueBlack Clover IdNoch keine Bewertungen
- Guillain Barre SyndromeDokument6 SeitenGuillain Barre SyndromeErtania NirmalaNoch keine Bewertungen
- 3rd Announcement Konas-IX PerdossiDokument30 Seiten3rd Announcement Konas-IX PerdossiA Hadid FirdiyanshahNoch keine Bewertungen
- Kaplan, Sadock, Grebb. 1997. Sinopsis Psikiatri Ilmu Pengetahuan Perilaku Psikiatri Klinis Jilid Satu. Jakarta: Binarupa AksaraDokument2 SeitenKaplan, Sadock, Grebb. 1997. Sinopsis Psikiatri Ilmu Pengetahuan Perilaku Psikiatri Klinis Jilid Satu. Jakarta: Binarupa AksaraLordeNoch keine Bewertungen
- Neuroanatomi 2011Dokument51 SeitenNeuroanatomi 2011Farah MuthiaNoch keine Bewertungen
- k20 - Stroke IskemikDokument35 Seitenk20 - Stroke IskemikZikri Putra Lan LubisNoch keine Bewertungen
- Spondiloartritis Diagnosis 2017 222234456Dokument40 SeitenSpondiloartritis Diagnosis 2017 222234456Alexandra BalanNoch keine Bewertungen
- Spondylitis TBDokument33 SeitenSpondylitis TBYohana KoliNoch keine Bewertungen
- Abdul Gofir Bagian Neurologi FK-UGM Klinik Memori & Unit Stroke RS SardjitoDokument48 SeitenAbdul Gofir Bagian Neurologi FK-UGM Klinik Memori & Unit Stroke RS SardjitoIyou Mistitans100% (1)
- EEG - Basic Principles and Application in EpilepsyDokument19 SeitenEEG - Basic Principles and Application in Epilepsyemilio9fernandez9gatNoch keine Bewertungen
- OphthalmoplegiaDokument5 SeitenOphthalmoplegiaPatricia Feliani SitohangNoch keine Bewertungen
- Rule of 4 brainstem stroke syndromesDokument2 SeitenRule of 4 brainstem stroke syndromesTracie TanNoch keine Bewertungen
- Understanding Neurobehavioral Disorders and DementiaDokument54 SeitenUnderstanding Neurobehavioral Disorders and DementiaWiratmono RahmadiNoch keine Bewertungen
- MNJ ToastDokument4 SeitenMNJ ToastRichard SuherlimNoch keine Bewertungen
- Low Back PainDokument34 SeitenLow Back PainFAMED RESIDENTS CESMEDNoch keine Bewertungen
- Neurobehavior Disorder: Diatri Nari LastriDokument104 SeitenNeurobehavior Disorder: Diatri Nari LastriKurniati HatmiNoch keine Bewertungen
- Hurler Syndrome (Biochem Repot)Dokument5 SeitenHurler Syndrome (Biochem Repot)Kristine Abegail CantillerNoch keine Bewertungen
- Perubahan Fungsional Penyakait Parkinson Dengan Menggunakan Unified Parkinson'S Disease RatingDokument10 SeitenPerubahan Fungsional Penyakait Parkinson Dengan Menggunakan Unified Parkinson'S Disease RatingAfifa NingrumNoch keine Bewertungen
- Transcranial Magnetic Stimulation (TMS) : by Denirae DavisDokument8 SeitenTranscranial Magnetic Stimulation (TMS) : by Denirae Davisapi-490032735Noch keine Bewertungen
- International Journal of Health Sciences and ResearchDokument8 SeitenInternational Journal of Health Sciences and ResearchZhara VidaNoch keine Bewertungen
- Extrapiramidal Symptom Rating Scale PDFDokument11 SeitenExtrapiramidal Symptom Rating Scale PDFsisca satyaNoch keine Bewertungen
- Ubogu - Inflammatory NeuropathiesDokument24 SeitenUbogu - Inflammatory NeuropathiesMarcelo BedoyaNoch keine Bewertungen
- Karakteristik Gangguan Tidur Pada Penyakit Parkinson Berdasarkan Parkinson Disease SleepDokument8 SeitenKarakteristik Gangguan Tidur Pada Penyakit Parkinson Berdasarkan Parkinson Disease SleepAfifa NingrumNoch keine Bewertungen
- Kuesioner NandaDokument8 SeitenKuesioner NandaAnanda AsmaraNoch keine Bewertungen
- MiopatiDokument7 SeitenMiopatiMarco HutagaolNoch keine Bewertungen
- Ohtahara Syndrome: Corticosteroids (Prednisolone or ACTH) Are Occasionally HelpfulDokument2 SeitenOhtahara Syndrome: Corticosteroids (Prednisolone or ACTH) Are Occasionally HelpfulidscribddotcomNoch keine Bewertungen
- Bronchitis Acute and ChronicDokument3 SeitenBronchitis Acute and Chronicdwi rina putriNoch keine Bewertungen
- Critical Appraisal PrognosisDokument15 SeitenCritical Appraisal PrognosismortazaqNoch keine Bewertungen
- Jurding NeurologiDokument11 SeitenJurding NeurologiHasya KinasihNoch keine Bewertungen
- Guillain BarreDokument12 SeitenGuillain BarreerikaNoch keine Bewertungen
- Lumbar Hernia Nukleus Pulposus: Moderator Prof. Dr. Mi. Widiastuti, Pak, SP.S (K), MSCDokument26 SeitenLumbar Hernia Nukleus Pulposus: Moderator Prof. Dr. Mi. Widiastuti, Pak, SP.S (K), MSCHarris MurdiantoNoch keine Bewertungen
- Enls V 4 0 Protocol Coma FinalDokument16 SeitenEnls V 4 0 Protocol Coma Finalsucipto suciptoNoch keine Bewertungen
- Motor Neuron DiseaseDokument22 SeitenMotor Neuron DiseaseNabin SimkhadaNoch keine Bewertungen
- Focal Cortical Dysplasia (FCD) WebabDokument3 SeitenFocal Cortical Dysplasia (FCD) WebabAyhan BölükNoch keine Bewertungen
- Causes, Symptoms & Types of Cerebral InfarctionDokument2 SeitenCauses, Symptoms & Types of Cerebral InfarctionMarie Aurora Gielbert MarianoNoch keine Bewertungen
- Diabeticum Ketoacidosis: Ach. Najich RF, DRDokument16 SeitenDiabeticum Ketoacidosis: Ach. Najich RF, DRAch Najich RfNoch keine Bewertungen
- Pott's DiseaseDokument34 SeitenPott's DiseaseNicole Marin-ChingNoch keine Bewertungen
- Gangguan Mental OrganikDokument27 SeitenGangguan Mental Organikmiftahul jannahNoch keine Bewertungen
- Referat Osteogenesis ImperfectaDokument21 SeitenReferat Osteogenesis ImperfectaArdhian RamadhanNoch keine Bewertungen
- DR Atitya-Epilepsi ILAE PDFDokument25 SeitenDR Atitya-Epilepsi ILAE PDFRayvan StudioTVNoch keine Bewertungen
- Trauma Kapitis RevisiDokument54 SeitenTrauma Kapitis RevisiRatika Ayu PiliangNoch keine Bewertungen
- Differences Between Myelopathy and Radiculopathy ExplainedDokument4 SeitenDifferences Between Myelopathy and Radiculopathy ExplainedWidiana KosasihNoch keine Bewertungen
- Anatomy of The Mental and Neurobehavior DisordersDokument57 SeitenAnatomy of The Mental and Neurobehavior DisordersiqiqiqiqiqNoch keine Bewertungen
- Neuro FinalDokument70 SeitenNeuro FinalOmar HatemNoch keine Bewertungen
- An Evidence-Based Approach to the Management of Nasopharyngeal Cancer: From Basic Science to Clinical Presentation and TreatmentVon EverandAn Evidence-Based Approach to the Management of Nasopharyngeal Cancer: From Basic Science to Clinical Presentation and TreatmentBaharudin AbdullahNoch keine Bewertungen
- Assessment of Current Diagnostic Criteria for Guillain-Barré SyndromeDokument4 SeitenAssessment of Current Diagnostic Criteria for Guillain-Barré SyndromeWening Hapsari100% (1)
- Ptosis Without Ophthalmoplegia: A Rare Manifestation of Guillain-Barré SyndromeDokument5 SeitenPtosis Without Ophthalmoplegia: A Rare Manifestation of Guillain-Barré SyndromeMosNoch keine Bewertungen
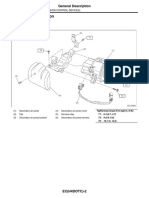
- Emission Control DevicesDokument27 SeitenEmission Control DevicesMarcelo BedoyaNoch keine Bewertungen
- Music BooksDokument1 SeiteMusic BooksMarcelo BedoyaNoch keine Bewertungen
- Lolli - Increased Reactivity To HTLV-1 in Inflammatory Nervous System DiseasesDokument5 SeitenLolli - Increased Reactivity To HTLV-1 in Inflammatory Nervous System DiseasesMarcelo BedoyaNoch keine Bewertungen
- Karak - Pseudo GBS Masking Acute Myeloid Leukemia RelapseDokument3 SeitenKarak - Pseudo GBS Masking Acute Myeloid Leukemia RelapseMarcelo BedoyaNoch keine Bewertungen
- Sejvar - GBS and Fisher Syndrome - Case Definitions and GuidelinesDokument15 SeitenSejvar - GBS and Fisher Syndrome - Case Definitions and GuidelinesMarcelo BedoyaNoch keine Bewertungen
- Saito - Increased Expression of OX40 in HTLV-1 Associated MyelopathyDokument15 SeitenSaito - Increased Expression of OX40 in HTLV-1 Associated MyelopathyMarcelo BedoyaNoch keine Bewertungen
- Kusumi - Epidemiology of Inflammatory Neurological and Inflamatory Neuromuscular Diseases in Tottori, JapanDokument6 SeitenKusumi - Epidemiology of Inflammatory Neurological and Inflamatory Neuromuscular Diseases in Tottori, JapanMarcelo BedoyaNoch keine Bewertungen
- Uncini - 99 Years of Guillain Barre SyndromeDokument2 SeitenUncini - 99 Years of Guillain Barre SyndromeMarcelo BedoyaNoch keine Bewertungen
- Ubogu - Inflammatory NeuropathiesDokument24 SeitenUbogu - Inflammatory NeuropathiesMarcelo BedoyaNoch keine Bewertungen
- Abbi - Guillain-Barré Syndrome After Use of Alemtuzumab (Campath) in A Patient With HTLV-I With ATLL (Case Report)Dokument3 SeitenAbbi - Guillain-Barré Syndrome After Use of Alemtuzumab (Campath) in A Patient With HTLV-I With ATLL (Case Report)Marcelo BedoyaNoch keine Bewertungen
- Brizzi - Peripheral Nerve in Infectious DiseasesDokument12 SeitenBrizzi - Peripheral Nerve in Infectious DiseasesMarcelo BedoyaNoch keine Bewertungen
- Abbi - Guillain-Barré Syndrome After Use of Alemtuzumab (Campath) in A Patient With HTLV-I With ATLL (Case Report)Dokument3 SeitenAbbi - Guillain-Barré Syndrome After Use of Alemtuzumab (Campath) in A Patient With HTLV-I With ATLL (Case Report)Marcelo BedoyaNoch keine Bewertungen
- CDC - Suerveillance For Guillain-Barré SyndromeDokument5 SeitenCDC - Suerveillance For Guillain-Barré SyndromeMarcelo BedoyaNoch keine Bewertungen
- 20 Ronchetti - Lead Neurotoxicity in Children - Prenatal or Postnatal ExposureDokument8 Seiten20 Ronchetti - Lead Neurotoxicity in Children - Prenatal or Postnatal ExposureMarcelo BedoyaNoch keine Bewertungen
- 2014 Fokke GBS Brighton Brain 2014Dokument11 Seiten2014 Fokke GBS Brighton Brain 2014Hikmat SatriaNoch keine Bewertungen
- Guillian Barre SyndromeDokument11 SeitenGuillian Barre SyndromemohamedNoch keine Bewertungen
- CDC Response Lead Exposure RecsDokument16 SeitenCDC Response Lead Exposure RecsAyu Wedhani SpcNoch keine Bewertungen
- Pokemon: Opening Theme: XylophoneDokument17 SeitenPokemon: Opening Theme: XylophoneMarcelo BedoyaNoch keine Bewertungen
- Posibles Temas 2016 - IIDokument1 SeitePosibles Temas 2016 - IIMarcelo BedoyaNoch keine Bewertungen
- Pokémon Theme (2 Pianos)Dokument7 SeitenPokémon Theme (2 Pianos)Marcelo BedoyaNoch keine Bewertungen
- +09 US Geological Survey - Mineral Commodity Summaries 2016Dokument205 Seiten+09 US Geological Survey - Mineral Commodity Summaries 2016Marcelo BedoyaNoch keine Bewertungen
- 18 - Schnaas - Reduced Intellectual Development in Children With Prenatal Lead ExposureDokument7 Seiten18 - Schnaas - Reduced Intellectual Development in Children With Prenatal Lead ExposureMarcelo BedoyaNoch keine Bewertungen
- 13 Patrick - Lead Toxicity - Exposure, Evaluation Adn TreatmentDokument21 Seiten13 Patrick - Lead Toxicity - Exposure, Evaluation Adn TreatmentMarcelo BedoyaNoch keine Bewertungen
- 02 WHO - Childhood Lead PoisoningDokument74 Seiten02 WHO - Childhood Lead PoisoningMarcelo BedoyaNoch keine Bewertungen
- Guidelines 2012 2013Dokument169 SeitenGuidelines 2012 2013Marcelo BedoyaNoch keine Bewertungen
- CG54 MigratedDokument34 SeitenCG54 MigratedMarcelo BedoyaNoch keine Bewertungen
- Otomicroscopy (Adult, Peds)Dokument4 SeitenOtomicroscopy (Adult, Peds)Carmen EneaNoch keine Bewertungen
- Effect of Aging On The ElectrocardiogramDokument4 SeitenEffect of Aging On The ElectrocardiogramHesbon MomanyiNoch keine Bewertungen
- British Homeopathic AssociationDokument195 SeitenBritish Homeopathic AssociationNasarMahmoodNoch keine Bewertungen
- Annotated Bibliography FormatDokument2 SeitenAnnotated Bibliography FormatJohn TerryNoch keine Bewertungen
- Multiple SclerosisDokument35 SeitenMultiple SclerosisJc SeguiNoch keine Bewertungen
- Medical CertificateDokument126 SeitenMedical CertificateAnonymous mummYD0% (1)
- Seminar 5 - Thyroid Disease in PregnancyDokument25 SeitenSeminar 5 - Thyroid Disease in PregnancyHakimah K. SuhaimiNoch keine Bewertungen
- Ointments, Creams and GelsDokument109 SeitenOintments, Creams and GelsAllyson Carlos100% (1)
- III. Nursing Care Plan: Assessment Diagnosis Goal Intervention EvaluationDokument4 SeitenIII. Nursing Care Plan: Assessment Diagnosis Goal Intervention EvaluationSTEPHANIE JOSUENoch keine Bewertungen
- 110 TOP SURGERY Multiple Choice Questions and Answers PDF - Medical Multiple Choice Questions PDFDokument11 Seiten110 TOP SURGERY Multiple Choice Questions and Answers PDF - Medical Multiple Choice Questions PDFaziz0% (1)
- The All India Services (Med Att Rules) - Misc InstructionsDokument22 SeitenThe All India Services (Med Att Rules) - Misc InstructionsJitendra Suraaj TripathiNoch keine Bewertungen
- Strength and Limitations of Early Warning ScoreDokument33 SeitenStrength and Limitations of Early Warning ScorePerawat CPNS 2018 RSUP Dr. KariadiNoch keine Bewertungen
- Corneal Foreign Body: Causes, Symptoms & TreatmentDokument2 SeitenCorneal Foreign Body: Causes, Symptoms & Treatmentmegayani santosoNoch keine Bewertungen
- Lois - Pemicu 5Dokument143 SeitenLois - Pemicu 5anggita tri lestariNoch keine Bewertungen
- SC Athletic Commission Medical FormDokument2 SeitenSC Athletic Commission Medical FormWilliam LowickNoch keine Bewertungen
- QaDokument16 SeitenQaAnn Caroline FerrerNoch keine Bewertungen
- By-Col Varughese Daniel Mba (Ha) 1 Yr (2 Sem.) : ST NDDokument46 SeitenBy-Col Varughese Daniel Mba (Ha) 1 Yr (2 Sem.) : ST NDAjayNoch keine Bewertungen
- Intersect ENT Investor Presentation - $XENTDokument28 SeitenIntersect ENT Investor Presentation - $XENTmedtechyNoch keine Bewertungen
- Effects of Kinesio Taping For Stroke Patients WithDokument8 SeitenEffects of Kinesio Taping For Stroke Patients WithBias HerkawentarNoch keine Bewertungen
- CetirizineDokument2 SeitenCetirizinelintangNoch keine Bewertungen
- Mind-Body Skills For Regulating The Autonomic Nervous SystemDokument60 SeitenMind-Body Skills For Regulating The Autonomic Nervous Systemnorociel8132100% (4)
- Pycnogenol For Cardiovascular Health - V2010Dokument12 SeitenPycnogenol For Cardiovascular Health - V2010LubimOffNoch keine Bewertungen
- Figure FaultsDokument17 SeitenFigure FaultsMichael SimpsonNoch keine Bewertungen
- Lateralizing Value of Todd's PalsyDokument3 SeitenLateralizing Value of Todd's PalsyLakshya J BasumataryNoch keine Bewertungen
- United States Complaint in Intervention in False Claims Act Lawsuits Accusing Insys Therapeutics of Paying Kickbacks and Engaging in Other Unlawful Practices to Promote Subsys, A Powerful Opioid PainkillerDokument37 SeitenUnited States Complaint in Intervention in False Claims Act Lawsuits Accusing Insys Therapeutics of Paying Kickbacks and Engaging in Other Unlawful Practices to Promote Subsys, A Powerful Opioid PainkillerBeverly Tran100% (1)
- Disseminated Intravascular CoagulationDokument4 SeitenDisseminated Intravascular CoagulationHendra SshNoch keine Bewertungen
- Strickland PresentationDokument1 SeiteStrickland Presentationmariopi2495Noch keine Bewertungen
- Anaesthesia in Pre-Eclampsia and Eclampsia 2Dokument52 SeitenAnaesthesia in Pre-Eclampsia and Eclampsia 2Lee June LyngNoch keine Bewertungen
- Auditory Processing DisorderDokument4 SeitenAuditory Processing DisorderRuztiqa Kasih Pramudya Vardani100% (1)
- Morales-Roman ResumeDokument2 SeitenMorales-Roman Resumeapi-301624882Noch keine Bewertungen