Das könnte Ihnen auch gefallen
- WHT Is A VeneerDokument3 SeitenWHT Is A VeneeruhvyasNoch keine Bewertungen
- Orthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentVon EverandOrthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentFederico BrugnamiNoch keine Bewertungen
- Case Report 2: Feldspathic Veneers: What Are Their Indications?Dokument6 SeitenCase Report 2: Feldspathic Veneers: What Are Their Indications?Nol H. CenaNoch keine Bewertungen
- Vsip - Info - Anterior Wax Up PDF Free PDFDokument3 SeitenVsip - Info - Anterior Wax Up PDF Free PDFMekideche dental officeNoch keine Bewertungen
- Advantages of Adhesive in DentistryDokument29 SeitenAdvantages of Adhesive in DentistryAnonymous CY62A9Noch keine Bewertungen
- Innovative Trending Topics Dentistry.: Stay in Touch With The Most and inDokument44 SeitenInnovative Trending Topics Dentistry.: Stay in Touch With The Most and inSachinSharmaNoch keine Bewertungen
- DentureDokument80 SeitenDentureDrShweta SainiNoch keine Bewertungen
- Cosmetic Dentistry CSD 2013Dokument3 SeitenCosmetic Dentistry CSD 2013Rodrigo Daniel Vela RiveraNoch keine Bewertungen
- IJEDe 15 03 Rocca 852 2Dokument22 SeitenIJEDe 15 03 Rocca 852 2hannaly estradaNoch keine Bewertungen
- 2 - Evaluation of Bond Strength and Thickness of Adhesive Layer According To The Techniques of Applying Adhesives in Composite Resin RestorationsDokument7 Seiten2 - Evaluation of Bond Strength and Thickness of Adhesive Layer According To The Techniques of Applying Adhesives in Composite Resin RestorationskochikaghochiNoch keine Bewertungen
- Blanqueamiento No Vital PDFDokument11 SeitenBlanqueamiento No Vital PDFPatricio Alejandro Cornejo Mutizabal100% (1)
- PDFDokument12 SeitenPDFHugoRoCkstarNoch keine Bewertungen
- Atraumatic Restorative Treatment: Restorative ComponentDokument11 SeitenAtraumatic Restorative Treatment: Restorative ComponentYu Yu Victor ChienNoch keine Bewertungen
- Management of Discoloured ToothDokument8 SeitenManagement of Discoloured ToothAnurtha AnuNoch keine Bewertungen
- Denu 2017 44 9 821Dokument7 SeitenDenu 2017 44 9 821Yolanda EvansNoch keine Bewertungen
- 11 - Soft Tissue Waxup and Mock-Up and Key Factors inDokument15 Seiten11 - Soft Tissue Waxup and Mock-Up and Key Factors inPablo BenitezNoch keine Bewertungen
- Posterior CompositeDokument21 SeitenPosterior CompositeNaji Z. ArandiNoch keine Bewertungen
- Cosmetic Dentistry & Aesthetic Restorative Dentistry: Comprehensive One-Year CourseDokument21 SeitenCosmetic Dentistry & Aesthetic Restorative Dentistry: Comprehensive One-Year CourseMariusNONoch keine Bewertungen
- Advance in MaterialsDokument10 SeitenAdvance in Materialssami robalinoNoch keine Bewertungen
- Direct Cuspal-Coverage Posterior Resin Composite Restorations: A Case ReportDokument8 SeitenDirect Cuspal-Coverage Posterior Resin Composite Restorations: A Case ReportDinar ArdhananeswariNoch keine Bewertungen
- Copy Dentures: Presenter DR Obiero Moderator DR Omondi 2/3/2021Dokument58 SeitenCopy Dentures: Presenter DR Obiero Moderator DR Omondi 2/3/2021elishaNoch keine Bewertungen
- Direct Posterior Composite Restorations. FinalDokument8 SeitenDirect Posterior Composite Restorations. FinalJana AliNoch keine Bewertungen
- 20 2003 - Magne - Anatomic Crown Width LengthDokument9 Seiten20 2003 - Magne - Anatomic Crown Width LengthSilvia KriNoch keine Bewertungen
- Posterior Inlay and Onlay: Ibrahim Nabil AzizDokument42 SeitenPosterior Inlay and Onlay: Ibrahim Nabil AzizRaul MurgNoch keine Bewertungen
- Digital Smile Design: A Tool For Treatment Planning and Communication in Esthetic DentistryDokument10 SeitenDigital Smile Design: A Tool For Treatment Planning and Communication in Esthetic Dentistrygilberto69Noch keine Bewertungen
- CPR For The Worn DentitionDokument17 SeitenCPR For The Worn DentitionGustavo A OrtegonNoch keine Bewertungen
- Bonding To Caries Affected DentinDokument13 SeitenBonding To Caries Affected DentinJoshua Valdez100% (1)
- BoptloiDokument14 SeitenBoptloiSonea M100% (1)
- Bringing Composite To An Art Form in The Anterior SegmentDokument4 SeitenBringing Composite To An Art Form in The Anterior SegmentMohamed Ibrahem MohamedNoch keine Bewertungen
- Recent Advances in Materials For All-Ceramic RestorationsDokument19 SeitenRecent Advances in Materials For All-Ceramic RestorationsManishak YessayanNoch keine Bewertungen
- 3c. The Effect of A Fiber Reinforced Cavity Configuration On Load Bearing Capacity and Failure Mode of Endodontically Treated Molars Restored With CAD-CAM Resin Composite Overlay Restorations PDFDokument10 Seiten3c. The Effect of A Fiber Reinforced Cavity Configuration On Load Bearing Capacity and Failure Mode of Endodontically Treated Molars Restored With CAD-CAM Resin Composite Overlay Restorations PDFAnisha AnilNoch keine Bewertungen
- Impact of Lateral Occlusion Schemes: A Systematic ReviewDokument12 SeitenImpact of Lateral Occlusion Schemes: A Systematic ReviewCristobalVeraNoch keine Bewertungen
- Modern Dental Ceramics An OverviewDokument6 SeitenModern Dental Ceramics An OverviewDilesh PradhanNoch keine Bewertungen
- Clinical Techniques For Composite PlacementDokument4 SeitenClinical Techniques For Composite PlacementRizta RiztiaNoch keine Bewertungen
- Teflon Tape TechniqueDokument6 SeitenTeflon Tape TechniqueJuan K. J. Shin100% (1)
- Case Report Konser 2Dokument22 SeitenCase Report Konser 2Nisa Ulil AmriNoch keine Bewertungen
- Clinical Evaluation of Abutment Teeth of Removable PartialDokument7 SeitenClinical Evaluation of Abutment Teeth of Removable PartialAlex KwokNoch keine Bewertungen
- 7-All-Ceramics Try in & CementationDokument56 Seiten7-All-Ceramics Try in & Cementationhassan.h.h.elhusseiny100% (1)
- Laminates and Veneer Endodontics.Dokument19 SeitenLaminates and Veneer Endodontics.shayeestahNoch keine Bewertungen
- Venus Fahl PPAD 20061018Dokument6 SeitenVenus Fahl PPAD 20061018RedhabAbbassNoch keine Bewertungen
- Bleaching Tray FabricationDokument5 SeitenBleaching Tray FabricationVishal MalusareNoch keine Bewertungen
- Cement System and Surface Treatment Selection For Fiber Post LutingDokument8 SeitenCement System and Surface Treatment Selection For Fiber Post LutingHitesh ChopraNoch keine Bewertungen
- Goldstein Re Esthetics in DentistryDokument3 SeitenGoldstein Re Esthetics in DentistryMichaelNoch keine Bewertungen
- PeekDokument8 SeitenPeeksalmaNoch keine Bewertungen
- Existing Restoration - Clinical Status: Secondary Caries Marginal Integrity Biomechanical FormDokument47 SeitenExisting Restoration - Clinical Status: Secondary Caries Marginal Integrity Biomechanical FormDaniel WangNoch keine Bewertungen
- Tooth Carving Exercise As A Foundation For Future Dental Career - A ReviewDokument3 SeitenTooth Carving Exercise As A Foundation For Future Dental Career - A ReviewRik ChatterjeeNoch keine Bewertungen
- Biologic Interfaces in Esthetic Dentistry. Part I: The Perio/restorative InterfaceDokument21 SeitenBiologic Interfaces in Esthetic Dentistry. Part I: The Perio/restorative InterfaceRoopa BabannavarNoch keine Bewertungen
- Indirect Composite Inlay and OnlaysDokument6 SeitenIndirect Composite Inlay and OnlaysAdrian DjohanNoch keine Bewertungen
- Dental Ceramics For Restoration and Metal VeneeringDokument23 SeitenDental Ceramics For Restoration and Metal VeneeringMichael XuNoch keine Bewertungen
- Direct Posterior Restoration PDFDokument14 SeitenDirect Posterior Restoration PDFياسر نادر حسين فليحNoch keine Bewertungen
- Additive Contour of Porcelain Veneers A Key Element in Enamel PreservationDokument13 SeitenAdditive Contour of Porcelain Veneers A Key Element in Enamel PreservationPablo BenitezNoch keine Bewertungen
- Fiber Post System - Critical ReviewDokument7 SeitenFiber Post System - Critical ReviewKirti SharmaNoch keine Bewertungen
- V9n3a17 PDFDokument6 SeitenV9n3a17 PDFRossye MpfNoch keine Bewertungen
- IPS E.maxDokument32 SeitenIPS E.maxKhaled ElshabrawyNoch keine Bewertungen
- Hesham Porcelain Laminate VeneersDokument67 SeitenHesham Porcelain Laminate VeneersHesham Sabet 'Backlawiz'Noch keine Bewertungen
- Composite in Everyday Practice - How To Choose The Right Material and Simplify Application Techniques in The Anterior TeethDokument24 SeitenComposite in Everyday Practice - How To Choose The Right Material and Simplify Application Techniques in The Anterior TeethTania Azuara100% (1)
- Bonded Composites Versus Ceramic Veneers PDFDokument7 SeitenBonded Composites Versus Ceramic Veneers PDFAnnaAffandieNoch keine Bewertungen
- Tooth ColoredDokument11 SeitenTooth Coloredmekit_13Noch keine Bewertungen
- Removable Partial Dentures: The Clinical Need For InnovationDokument8 SeitenRemovable Partial Dentures: The Clinical Need For InnovationNetra TaleleNoch keine Bewertungen
- Prevalence of Tooth Forms and Their Gender CorrelationDokument6 SeitenPrevalence of Tooth Forms and Their Gender CorrelationPablo BenitezNoch keine Bewertungen
- Layperson 'S Perception of Axial Midline Angulation in Asymmetric FacesDokument7 SeitenLayperson 'S Perception of Axial Midline Angulation in Asymmetric FacesPablo BenitezNoch keine Bewertungen
- Chromatic Influence of Value Resin Composites: Operative Dentistry, 2010Dokument6 SeitenChromatic Influence of Value Resin Composites: Operative Dentistry, 2010Pablo BenitezNoch keine Bewertungen
- Ultimate Ceramic Veneers: A Laboratory-Guided Preparation Technique For Minimally Invasive RestorationsDokument17 SeitenUltimate Ceramic Veneers: A Laboratory-Guided Preparation Technique For Minimally Invasive RestorationsPablo BenitezNoch keine Bewertungen
- Jopr B1Dokument13 SeitenJopr B1Pablo BenitezNoch keine Bewertungen
- JCDR - B2Dokument10 SeitenJCDR - B2Pablo BenitezNoch keine Bewertungen
- Virtual Smile Design Tip: From 2D To 3D Design With Free SoftwareDokument2 SeitenVirtual Smile Design Tip: From 2D To 3D Design With Free SoftwarePablo BenitezNoch keine Bewertungen
- Inhibitory Effect of Toothbrush Monofilament Containing Surface Pre Reacted Glass Ionomer (S PRG) Filler On Streptococcus MutansDokument12 SeitenInhibitory Effect of Toothbrush Monofilament Containing Surface Pre Reacted Glass Ionomer (S PRG) Filler On Streptococcus MutansPablo BenitezNoch keine Bewertungen
- Grupo 1Dokument6 SeitenGrupo 1Pablo BenitezNoch keine Bewertungen
- Acquired Salivary Pellicle and Oral Diseases: A Literature ReviewDokument7 SeitenAcquired Salivary Pellicle and Oral Diseases: A Literature ReviewPablo BenitezNoch keine Bewertungen
- Acquired Salivary Pellicle and Oral Diseases: A Literature ReviewDokument7 SeitenAcquired Salivary Pellicle and Oral Diseases: A Literature ReviewPablo BenitezNoch keine Bewertungen
- Partial Caries Removal Increases The Survival of Permanent Tooth: A 14-Year Case ReportDokument4 SeitenPartial Caries Removal Increases The Survival of Permanent Tooth: A 14-Year Case ReportPablo BenitezNoch keine Bewertungen
- Partial Caries Removal Increases The Survival of Permanent Tooth: A 14-Year Case ReportDokument4 SeitenPartial Caries Removal Increases The Survival of Permanent Tooth: A 14-Year Case ReportPablo BenitezNoch keine Bewertungen
- When To Intervene in The Caries Process? An Expert Delphi Consensus StatementDokument13 SeitenWhen To Intervene in The Caries Process? An Expert Delphi Consensus StatementPablo BenitezNoch keine Bewertungen
- Partial Caries Removal Increases The Survival of Permanent Tooth: A 14-Year Case ReportDokument4 SeitenPartial Caries Removal Increases The Survival of Permanent Tooth: A 14-Year Case ReportPablo BenitezNoch keine Bewertungen
- Nyvad CriteriaDokument9 SeitenNyvad CriteriaKarin SumNoch keine Bewertungen
- Breast and Bottle Feeding As Risk Factors For Dental Caries A Systematic Review and Meta-AnalysisDokument14 SeitenBreast and Bottle Feeding As Risk Factors For Dental Caries A Systematic Review and Meta-AnalysisHandiniNoch keine Bewertungen
- Caries PDFDokument10 SeitenCaries PDFMilton David Rios SerratoNoch keine Bewertungen
- Acquired Salivary Pellicle and Oral Diseases: A Literature ReviewDokument7 SeitenAcquired Salivary Pellicle and Oral Diseases: A Literature ReviewPablo BenitezNoch keine Bewertungen
- Recuperación Sem 1 CamilaDokument5 SeitenRecuperación Sem 1 CamilaPablo BenitezNoch keine Bewertungen
- Demineralization-Remineralization Dynamics in Teeth and BoneDokument21 SeitenDemineralization-Remineralization Dynamics in Teeth and BonePablo BenitezNoch keine Bewertungen
- Grupo 3 Rev5Dokument10 SeitenGrupo 3 Rev5Pablo BenitezNoch keine Bewertungen
- Grupo 2Dokument6 SeitenGrupo 2Pablo BenitezNoch keine Bewertungen
- Dental Caries: Infectious and Transmissible DiseaseDokument19 SeitenDental Caries: Infectious and Transmissible DiseasePablo BenitezNoch keine Bewertungen
- Fejerskov-1997-Community Dentistry and Oral EpidemiologyDokument9 SeitenFejerskov-1997-Community Dentistry and Oral Epidemiologylarissa costaNoch keine Bewertungen
- Grupo 4 Rev1Dokument4 SeitenGrupo 4 Rev1Pablo BenitezNoch keine Bewertungen
- Caries DentalDokument9 SeitenCaries DentalMaría Victoria Ordóñez VerdesotoNoch keine Bewertungen
- Dental Caries in The Second Millennium: Conference PapersDokument7 SeitenDental Caries in The Second Millennium: Conference PapersPablo BenitezNoch keine Bewertungen
- CariologiaDokument8 SeitenCariologiaMarie Meléndez FalcónNoch keine Bewertungen
- Dental Caries in The Second Millennium: Conference PapersDokument7 SeitenDental Caries in The Second Millennium: Conference PapersPablo BenitezNoch keine Bewertungen
- Report BeetrootDokument11 SeitenReport BeetrootSya Subi100% (3)
- Module 2 - Drug AbuseDokument35 SeitenModule 2 - Drug AbuseMark Johnuel DuavisNoch keine Bewertungen
- NTK O2 Sensor HistoryDokument9 SeitenNTK O2 Sensor Historyonukvedat7219Noch keine Bewertungen
- TB400 Painting and Corrosion ProtectionDokument21 SeitenTB400 Painting and Corrosion ProtectionAliZenatiNoch keine Bewertungen
- 772838Dokument2 Seiten772838Wilder Atalaya ChavezNoch keine Bewertungen
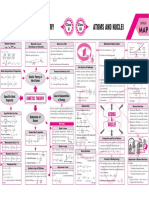
- KInatics Theory and Atom and Nuclie MMDokument1 SeiteKInatics Theory and Atom and Nuclie MMSanjay GuptaNoch keine Bewertungen
- Stimulation Manual ONGC 2008Dokument306 SeitenStimulation Manual ONGC 2008rahul_storm100% (3)
- Selective Oxidation of Secondary AlcoholsDokument24 SeitenSelective Oxidation of Secondary AlcoholsFernando Silva BetimNoch keine Bewertungen
- Eazistrip Reinforcement Continuity SystemsDokument12 SeitenEazistrip Reinforcement Continuity SystemscormolioNoch keine Bewertungen
- Laxatives1 and PurgativesDokument38 SeitenLaxatives1 and PurgativesGareth Bale100% (1)
- METALS Structured Questions and Worked SolutionsDokument9 SeitenMETALS Structured Questions and Worked SolutionsYoviNoch keine Bewertungen
- Threshold Limit Values (TLV)Dokument7 SeitenThreshold Limit Values (TLV)chem_taNoch keine Bewertungen
- NeutralisationDokument12 SeitenNeutralisationBank Yossy WoluslaweNoch keine Bewertungen
- Applications and Impact of Nanocellulose Based AdsorbentsDokument24 SeitenApplications and Impact of Nanocellulose Based AdsorbentsLuiz CardNoch keine Bewertungen
- Resilon 4301 Polyurethane Specs ResourcesDokument2 SeitenResilon 4301 Polyurethane Specs ResourcesAdolfo CarellaNoch keine Bewertungen
- Lectures TheoryofStructures1 Chapter1 PDFDokument27 SeitenLectures TheoryofStructures1 Chapter1 PDFMikoy TicmonNoch keine Bewertungen
- Carbon Structural Steel: Standardspecification ForDokument4 SeitenCarbon Structural Steel: Standardspecification ForlinaNoch keine Bewertungen
- Good Introduction To ElastomerDokument12 SeitenGood Introduction To ElastomerAnirudhreddy SafalNoch keine Bewertungen
- Conservation Equations and Modeling of Chemical and Biochemical ProcessesDokument650 SeitenConservation Equations and Modeling of Chemical and Biochemical ProcessesArman BasmacıoğluNoch keine Bewertungen
- Module 1Dokument15 SeitenModule 1venugopal_aeroNoch keine Bewertungen
- T105 Trojan Data SheetsDokument126 SeitenT105 Trojan Data SheetsJose Luis PandoNoch keine Bewertungen
- Nama Obat Saluran CernaDokument4 SeitenNama Obat Saluran Cernadewi puspitaNoch keine Bewertungen
- B31.3 Course Handout IntroDokument0 SeitenB31.3 Course Handout IntroNeily LiuNoch keine Bewertungen
- Lied Mann 2017Dokument8 SeitenLied Mann 2017Chandra SekarNoch keine Bewertungen
- Adapaleno - Clindamicina Gel HPLCDokument5 SeitenAdapaleno - Clindamicina Gel HPLCDavid SanabriaNoch keine Bewertungen
- Octostat 50Dokument1 SeiteOctostat 50chayanunNoch keine Bewertungen
- Rinnai 26e Service Manual PDFDokument68 SeitenRinnai 26e Service Manual PDFteddiprintNoch keine Bewertungen
- Concentration Term Jee Main Selected 2Dokument3 SeitenConcentration Term Jee Main Selected 2aebafbigiNoch keine Bewertungen
- Algal Oil Production: Modeling and Evaluation Using Superpro DesignerDokument26 SeitenAlgal Oil Production: Modeling and Evaluation Using Superpro DesignerMira FazziraNoch keine Bewertungen
- United States Patent: (45) Date of Patent: Aug - 21, 2018Dokument22 SeitenUnited States Patent: (45) Date of Patent: Aug - 21, 2018RiskaNoch keine Bewertungen
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaVon EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Roxane Gay & Everand Originals Presents: Good Girl: Notes on Dog RescueVon EverandRoxane Gay & Everand Originals Presents: Good Girl: Notes on Dog RescueBewertung: 5 von 5 Sternen5/5 (3)
- Roxane Gay & Everand Originals Presents: Good Girl: Notes on Dog RescueVon EverandRoxane Gay & Everand Originals Presents: Good Girl: Notes on Dog RescueBewertung: 4.5 von 5 Sternen4.5/5 (26)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisVon EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisBewertung: 4.5 von 5 Sternen4.5/5 (42)
- Gut: the new and revised Sunday Times bestsellerVon EverandGut: the new and revised Sunday Times bestsellerBewertung: 4 von 5 Sternen4/5 (393)
- The Obesity Code: Unlocking the Secrets of Weight LossVon EverandThe Obesity Code: Unlocking the Secrets of Weight LossBewertung: 4 von 5 Sternen4/5 (6)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisVon EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisBewertung: 5 von 5 Sternen5/5 (8)
- Sugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthVon EverandSugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthBewertung: 4 von 5 Sternen4/5 (6)
- Peak: The New Science of Athletic Performance That is Revolutionizing SportsVon EverandPeak: The New Science of Athletic Performance That is Revolutionizing SportsBewertung: 5 von 5 Sternen5/5 (97)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisVon EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisBewertung: 4 von 5 Sternen4/5 (9)
- Alex & Me: How a Scientist and a Parrot Discovered a Hidden World of Animal Intelligence—and Formed a Deep Bond in the ProcessVon EverandAlex & Me: How a Scientist and a Parrot Discovered a Hidden World of Animal Intelligence—and Formed a Deep Bond in the ProcessNoch keine Bewertungen
- 10% Human: How Your Body's Microbes Hold the Key to Health and HappinessVon Everand10% Human: How Your Body's Microbes Hold the Key to Health and HappinessBewertung: 4 von 5 Sternen4/5 (33)
- All That Remains: A Renowned Forensic Scientist on Death, Mortality, and Solving CrimesVon EverandAll That Remains: A Renowned Forensic Scientist on Death, Mortality, and Solving CrimesBewertung: 4.5 von 5 Sternen4.5/5 (397)
- Critical Care: A New Nurse Faces Death, Life, and Everything in BetweenVon EverandCritical Care: A New Nurse Faces Death, Life, and Everything in BetweenBewertung: 3.5 von 5 Sternen3.5/5 (159)
- Tales from Both Sides of the Brain: A Life in NeuroscienceVon EverandTales from Both Sides of the Brain: A Life in NeuroscienceBewertung: 3 von 5 Sternen3/5 (18)
- Crooked: Outwitting the Back Pain Industry and Getting on the Road to RecoveryVon EverandCrooked: Outwitting the Back Pain Industry and Getting on the Road to RecoveryBewertung: 3.5 von 5 Sternen3.5/5 (9)
- Gut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Von EverandGut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Bewertung: 4 von 5 Sternen4/5 (411)
- Molecules of Emotion: Why You Feel the Way You FeelVon EverandMolecules of Emotion: Why You Feel the Way You FeelBewertung: 4 von 5 Sternen4/5 (128)
- The Egoscue Method of Health Through Motion: A Revolutionary Program That Lets You Rediscover the Body's Power to Protect and Rejuvenate ItselfVon EverandThe Egoscue Method of Health Through Motion: A Revolutionary Program That Lets You Rediscover the Body's Power to Protect and Rejuvenate ItselfBewertung: 4 von 5 Sternen4/5 (8)
- Merle's Door: Lessons from a Freethinking DogVon EverandMerle's Door: Lessons from a Freethinking DogBewertung: 4 von 5 Sternen4/5 (326)
- Uncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicVon EverandUncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicNoch keine Bewertungen
- Will's Red Coat: The Story of One Old Dog Who Chose to Live AgainVon EverandWill's Red Coat: The Story of One Old Dog Who Chose to Live AgainBewertung: 4.5 von 5 Sternen4.5/5 (18)
- The Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyVon EverandThe Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyNoch keine Bewertungen
- Summary: Breath: The New Science of a Lost Art by James Nestor: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: Breath: The New Science of a Lost Art by James Nestor: Key Takeaways, Summary & Analysis IncludedBewertung: 4.5 von 5 Sternen4.5/5 (5)
- Become a Magnet of Positive Things Hypnosis: With sleep hypnosis and subliminal affirmationsVon EverandBecome a Magnet of Positive Things Hypnosis: With sleep hypnosis and subliminal affirmationsNoch keine Bewertungen
- DSM-5-TR Diagnostic And Statistical Manual Of Mental Disorders: DSM 5 TR Desk Reference to the Diagnostic CriteriaVon EverandDSM-5-TR Diagnostic And Statistical Manual Of Mental Disorders: DSM 5 TR Desk Reference to the Diagnostic CriteriaNoch keine Bewertungen
- The Dog Listener: Learn How to Communicate with Your Dog for Willing CooperationVon EverandThe Dog Listener: Learn How to Communicate with Your Dog for Willing CooperationBewertung: 4 von 5 Sternen4/5 (37)