Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1091)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Disclaimer of Interest Form PDFDokument2 SeitenDisclaimer of Interest Form PDFSpiritually GiftedNoch keine Bewertungen
- MatlaB Lab Manual APDokument63 SeitenMatlaB Lab Manual APVarun SahaniNoch keine Bewertungen
- Pipe Rack DesignDokument51 SeitenPipe Rack Designsur50% (2)
- 3 - Cellular Respiration NotesDokument22 Seiten3 - Cellular Respiration Notesapi-375285021Noch keine Bewertungen
- Quantum Physics Exam Questions 69 QuestionsDokument145 SeitenQuantum Physics Exam Questions 69 QuestionsVedant BhardwajNoch keine Bewertungen
- Low Back Pain A Comprehensive Review Pathophysiology 2019Dokument10 SeitenLow Back Pain A Comprehensive Review Pathophysiology 2019Victor Andrés Olivares IbarraNoch keine Bewertungen
- Soalan Tugasan 2 HBEC4403 OUMDokument7 SeitenSoalan Tugasan 2 HBEC4403 OUMTutor EvonNoch keine Bewertungen
- 2022 Red and White FlagsDokument4 Seiten2022 Red and White FlagsVictor Andrés Olivares IbarraNoch keine Bewertungen
- Red Flag Screening For Low Back PainDokument5 SeitenRed Flag Screening For Low Back PainVictor Andrés Olivares IbarraNoch keine Bewertungen
- Red Flags Presented in Current Low Back Pain Guidelines: A ReviewDokument15 SeitenRed Flags Presented in Current Low Back Pain Guidelines: A ReviewVictor Andrés Olivares IbarraNoch keine Bewertungen
- MRI Hip Findings in Asymptomatic Blankenstein 2019Dokument7 SeitenMRI Hip Findings in Asymptomatic Blankenstein 2019Victor Andrés Olivares IbarraNoch keine Bewertungen
- Entrenamiento IsoinercialDokument9 SeitenEntrenamiento IsoinercialVictor Andrés Olivares IbarraNoch keine Bewertungen
- 2016 Muscle Activation Comparisons Between Elastic and Isoinertial ResistanceDokument10 Seiten2016 Muscle Activation Comparisons Between Elastic and Isoinertial ResistanceVictor Andrés Olivares IbarraNoch keine Bewertungen
- Dolor Radicular y Pseudo Dolor Radicular Freynhagen 2008Dokument10 SeitenDolor Radicular y Pseudo Dolor Radicular Freynhagen 2008Victor Andrés Olivares IbarraNoch keine Bewertungen
- Sensibilizacion Central 2020 JosptDokument8 SeitenSensibilizacion Central 2020 JosptVictor Andrés Olivares IbarraNoch keine Bewertungen
- Treating Tendonopathy 2015Dokument12 SeitenTreating Tendonopathy 2015Victor Andrés Olivares IbarraNoch keine Bewertungen
- Clinical Anatomy of The Knee PDFDokument7 SeitenClinical Anatomy of The Knee PDFJuan Victor Briceno OrtizNoch keine Bewertungen
- Lasegue Sign 2017Dokument2 SeitenLasegue Sign 2017Victor Andrés Olivares IbarraNoch keine Bewertungen
- Tendon 2017Dokument3 SeitenTendon 2017Victor Andrés Olivares IbarraNoch keine Bewertungen
- Tendonopathy in Athletes PDFDokument8 SeitenTendonopathy in Athletes PDFVictor Andrés Olivares IbarraNoch keine Bewertungen
- Flywheel Paradigm IsoinercialDokument10 SeitenFlywheel Paradigm IsoinercialVictor Andrés Olivares IbarraNoch keine Bewertungen
- Diagnosis and Management of Superior Labral Anterior Posterior Tears in Throwing AthletesDokument18 SeitenDiagnosis and Management of Superior Labral Anterior Posterior Tears in Throwing AthletesVictor Andrés Olivares IbarraNoch keine Bewertungen
- 180-SCF-3314 - Job DescriptionDokument17 Seiten180-SCF-3314 - Job DescriptionUmair AshfaqNoch keine Bewertungen
- Solid State Broadband High Power Amplifier: 1 - 30 MHZ / 50 WattsDokument3 SeitenSolid State Broadband High Power Amplifier: 1 - 30 MHZ / 50 Wattskhanafzaal2576Noch keine Bewertungen
- 曼昆《经济学原理第三版》宏观分册原版中英文双语PPT课件Chap 25Dokument76 Seiten曼昆《经济学原理第三版》宏观分册原版中英文双语PPT课件Chap 25Jia Wei MiaoNoch keine Bewertungen
- Security Analysis: Kumar SaurabhDokument11 SeitenSecurity Analysis: Kumar Saurabhakhil vermaNoch keine Bewertungen
- Descriptive Lab Report GuideDokument3 SeitenDescriptive Lab Report GuideOluwafisayomi LawaniNoch keine Bewertungen
- If ClauseDokument13 SeitenIf Clausemadeleine mmdNoch keine Bewertungen
- Class 12 Chemistry Project (Electochemistry)Dokument10 SeitenClass 12 Chemistry Project (Electochemistry)Raghvendra Pandey0% (1)
- Open CVDokument11 SeitenOpen CVXavier Ibarra CorteNoch keine Bewertungen
- ENGLISH PAGE - Verb Tense Exercise 3Dokument1 SeiteENGLISH PAGE - Verb Tense Exercise 3Eka BeradzeNoch keine Bewertungen
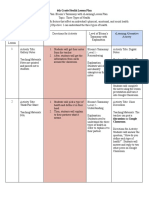
- 6th Grade Health Lesson Plan - Portfolio - BloomsDokument3 Seiten6th Grade Health Lesson Plan - Portfolio - Bloomsapi-475320683Noch keine Bewertungen
- DefinitionsDokument7 SeitenDefinitionsJazmine ButuhanNoch keine Bewertungen
- Cable Subjected To Concentrated Loads CaDokument41 SeitenCable Subjected To Concentrated Loads CaIcy MakerNoch keine Bewertungen
- Minimum Drag Velocity ExplainedDokument4 SeitenMinimum Drag Velocity ExplainedpersesutiNoch keine Bewertungen
- 3 ReviewsDokument14 Seiten3 ReviewsGabriela ZambranoNoch keine Bewertungen
- Optics and Lasers in EngineeringDokument5 SeitenOptics and Lasers in EngineeringsenthilNoch keine Bewertungen
- Z370 AORUS Gaming 3: User's ManualDokument48 SeitenZ370 AORUS Gaming 3: User's ManualAtrocitus RedNoch keine Bewertungen
- BOQ New Store Plumbing MDokument10 SeitenBOQ New Store Plumbing MMd. Mominul IslamNoch keine Bewertungen
- On PDMSDokument7 SeitenOn PDMSatorresh090675Noch keine Bewertungen
- Loom SettingsDokument4 SeitenLoom SettingsAnonymous Pt7NHkat9Noch keine Bewertungen
- BOSS GLOBAL CONCEPTS LTD - AML Policy-UpdatedDokument46 SeitenBOSS GLOBAL CONCEPTS LTD - AML Policy-UpdatedtwaseemdttNoch keine Bewertungen
- Trigon 4to3 SecDokument11 SeitenTrigon 4to3 SecmalcommmNoch keine Bewertungen
- Class 10 RespirationDokument3 SeitenClass 10 RespirationHimanshu singh100% (1)
- My Beamer TalkDokument85 SeitenMy Beamer TalkOtmane El ouardiNoch keine Bewertungen
- Paul Brunton - WikipediaDokument3 SeitenPaul Brunton - WikipediaShabd_MysticNoch keine Bewertungen