Das könnte Ihnen auch gefallen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Action Research PreseantationDokument29 SeitenAction Research PreseantationKusrini Kadar SyamsalamNoch keine Bewertungen
- Tiket Seminar FixedDokument2 SeitenTiket Seminar FixedKusrini Kadar SyamsalamNoch keine Bewertungen
- Output - ArtikelDokument13 SeitenOutput - ArtikelKusrini Kadar SyamsalamNoch keine Bewertungen
- A Journey Across An Unwelcoming Field A Qualitative Study Exploring The Factors Influencing Nursing Students Clinical EducationDokument6 SeitenA Journey Across An Unwelcoming Field A Qualitative Study Exploring The Factors Influencing Nursing Students Clinical EducationKusrini Kadar SyamsalamNoch keine Bewertungen
- Educating Nursing Students About Health Literacy - From The Classroom To The Patient BedsideDokument11 SeitenEducating Nursing Students About Health Literacy - From The Classroom To The Patient BedsideKusrini Kadar SyamsalamNoch keine Bewertungen
- Understanding Cultural and Linguistic Barriers To Health LiteracyDokument11 SeitenUnderstanding Cultural and Linguistic Barriers To Health LiteracyKusrini Kadar SyamsalamNoch keine Bewertungen
- Assessing Health Literacy: Diagnostic TipsDokument2 SeitenAssessing Health Literacy: Diagnostic TipsKusrini Kadar SyamsalamNoch keine Bewertungen
- A Systematic Review of The Literature On Health Literacy in Nursing EducationDokument5 SeitenA Systematic Review of The Literature On Health Literacy in Nursing EducationKusrini Kadar SyamsalamNoch keine Bewertungen
- 1.1. Core Competencies Diagram - 1Dokument1 Seite1.1. Core Competencies Diagram - 1Kusrini Kadar SyamsalamNoch keine Bewertungen
- The Perspective of Healthcare Providers and Patients On Health Literacy - A Systematic Review of The Quantitative and Qualitative StudiesDokument11 SeitenThe Perspective of Healthcare Providers and Patients On Health Literacy - A Systematic Review of The Quantitative and Qualitative StudiesKusrini Kadar SyamsalamNoch keine Bewertungen
- Giving and Receiving Feedback Participant GuideDokument72 SeitenGiving and Receiving Feedback Participant GuideKusrini Kadar Syamsalam0% (1)
- Surat DekanDokument1 SeiteSurat DekanKusrini Kadar SyamsalamNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Es 335 emDokument6 SeitenEs 335 emFirdosh Khan100% (2)
- 1 PBDokument17 Seiten1 PBaantiti12Noch keine Bewertungen
- Seven Elements For Capacity Development For Disaster Risk ReductionDokument4 SeitenSeven Elements For Capacity Development For Disaster Risk ReductionPer BeckerNoch keine Bewertungen
- The Teochew Chinese of ThailandDokument7 SeitenThe Teochew Chinese of ThailandbijsshrjournalNoch keine Bewertungen
- CBC1501-TL-101 2015 3 BDokument64 SeitenCBC1501-TL-101 2015 3 BJanke Van Niekerk50% (2)
- A Short Survey On The Usage of Choquet Integral and Its Associated Fuzzy Measure in Multiple Attribute AnalysisDokument8 SeitenA Short Survey On The Usage of Choquet Integral and Its Associated Fuzzy Measure in Multiple Attribute AnalysisfarisNoch keine Bewertungen
- Student Leave Management System Ijariie6549Dokument8 SeitenStudent Leave Management System Ijariie6549SteffenNoch keine Bewertungen
- Think Global and British Council The Global Skills GapDokument12 SeitenThink Global and British Council The Global Skills GapSherry LeeNoch keine Bewertungen
- CIK - msl.00166 ReportDokument3 SeitenCIK - msl.00166 ReportChristopher Edward Martin FlanaganNoch keine Bewertungen
- Impact of E-Bills Payment On Customer Satisfaction in Uganda: Stanbic Bank Uganda Limited As The Case StudyDokument8 SeitenImpact of E-Bills Payment On Customer Satisfaction in Uganda: Stanbic Bank Uganda Limited As The Case Study21-38010Noch keine Bewertungen
- OrganizingDokument46 SeitenOrganizingViswajeet BiswalNoch keine Bewertungen
- Model Question Paper AnsDokument19 SeitenModel Question Paper Ansnavadeep saiNoch keine Bewertungen
- University of Auckland PHD Thesis GuidelinesDokument6 SeitenUniversity of Auckland PHD Thesis Guidelinesygadgcgld100% (1)
- Pantaloons Employee Satisfaction Towards CompensationDokument61 SeitenPantaloons Employee Satisfaction Towards CompensationkaurArshpreet57% (7)
- CHIFAMBA MELBAH R213866M .Test InclassDokument3 SeitenCHIFAMBA MELBAH R213866M .Test InclasswilsonNoch keine Bewertungen
- Dhaka Ashulia Pre Feasibility ReportDokument332 SeitenDhaka Ashulia Pre Feasibility ReportAdeev El AzizNoch keine Bewertungen
- Zamoras Group Research About GAS StudentsDokument17 SeitenZamoras Group Research About GAS StudentsLenard ZamoraNoch keine Bewertungen
- ModelingDokument18 SeitenModelingLibya TripoliNoch keine Bewertungen
- Oklahoma State University Findings On MorgellonsDokument4 SeitenOklahoma State University Findings On MorgellonsSpace_Hulker100% (5)
- ArchanaDokument6 SeitenArchanaArchana DeviNoch keine Bewertungen
- Constructing ProbabilityDokument25 SeitenConstructing ProbabilityBianca BucsitNoch keine Bewertungen
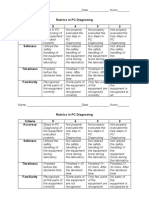
- Rubrics in PC Diagnosing Criteria 5 4 3 2 Accuracy: Name - Date - ScoreDokument2 SeitenRubrics in PC Diagnosing Criteria 5 4 3 2 Accuracy: Name - Date - Scorejhun ecleoNoch keine Bewertungen
- Ey The Indian Organic Market Report Online Version 21 March 2018Dokument52 SeitenEy The Indian Organic Market Report Online Version 21 March 2018Kamalaganesh Thirumeni100% (2)
- Critique Paper BSUDokument4 SeitenCritique Paper BSUAndrei Dela CruzNoch keine Bewertungen
- How To List Masters Thesis On ResumeDokument4 SeitenHow To List Masters Thesis On Resumebk4h4gbd100% (2)
- DR Dilip Pawar - Clinical Research in IndiaDokument37 SeitenDR Dilip Pawar - Clinical Research in IndiaRahul NairNoch keine Bewertungen
- Cost and Benefit Analysis of Solar Panels at HomeDokument8 SeitenCost and Benefit Analysis of Solar Panels at HomePoonam KilaniyaNoch keine Bewertungen
- Predicting Advertising Success Beyond Traditional Measures: New Insights From Neurophysiological Methods and Market Response ModelingDokument19 SeitenPredicting Advertising Success Beyond Traditional Measures: New Insights From Neurophysiological Methods and Market Response ModelingRccg DestinySanctuaryNoch keine Bewertungen
- Entrepreneurial Intentions and Corporate EntrepreneurshipDokument22 SeitenEntrepreneurial Intentions and Corporate Entrepreneurshipprojects_masterzNoch keine Bewertungen