Das könnte Ihnen auch gefallen
- A Systematic Approach To Adult Hip PainDokument12 SeitenA Systematic Approach To Adult Hip Pain69016Noch keine Bewertungen
- Trendelenberg's Test: DR - Ajit DeshmukhDokument16 SeitenTrendelenberg's Test: DR - Ajit DeshmukhStar CruiseNoch keine Bewertungen
- Trochanteric Bursitis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandTrochanteric Bursitis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- Low Back PainDokument8 SeitenLow Back PainLev KalikaNoch keine Bewertungen
- Clinical Examination: Acute Adductor InjuriesDokument18 SeitenClinical Examination: Acute Adductor Injuriessofianos100% (1)
- IvdpDokument89 SeitenIvdpFelix SabuNoch keine Bewertungen
- Hip and Groin Pain Radiological AssessmentDokument13 SeitenHip and Groin Pain Radiological AssessmentOscar NgNoch keine Bewertungen
- Scapular DyskinesisDokument24 SeitenScapular DyskinesisbarbaraNoch keine Bewertungen
- Joint Mobilizations PDFDokument1 SeiteJoint Mobilizations PDFErik TellezNoch keine Bewertungen
- Hip Impingement FaiDokument8 SeitenHip Impingement FaiLev KalikaNoch keine Bewertungen
- Distal Biceps Repair Rehabilitation Protocol by Tendayi MutsopotsiDokument5 SeitenDistal Biceps Repair Rehabilitation Protocol by Tendayi MutsopotsiPhysiotherapy Care SpecialistsNoch keine Bewertungen
- Hip and Buttock PainDokument26 SeitenHip and Buttock PainEdy SetiawanNoch keine Bewertungen
- Reinold - Glenohumeral and Scapulothoracic RehabDokument45 SeitenReinold - Glenohumeral and Scapulothoracic Rehabshivnair100% (2)
- Examination of The Upper Cervical Spine PDFDokument22 SeitenExamination of The Upper Cervical Spine PDFiikemNoch keine Bewertungen
- Foot and Ankle BiomechanicsDokument25 SeitenFoot and Ankle BiomechanicsSanh NguyễnNoch keine Bewertungen
- Musculoskeletal TraumaDokument103 SeitenMusculoskeletal TraumaJona Kristin EnclunaNoch keine Bewertungen
- Anterior Cruciate Ligament InjuriesDokument35 SeitenAnterior Cruciate Ligament InjuriesAhmad Hakim Al-ashrafNoch keine Bewertungen
- PostureDokument2 SeitenPostureNader MorrisNoch keine Bewertungen
- Iliopsoas Syndrome - The Hidden Root of PainDokument13 SeitenIliopsoas Syndrome - The Hidden Root of Painpeter1234u0% (1)
- The Shoulder PainDokument14 SeitenThe Shoulder PainLev KalikaNoch keine Bewertungen
- Cervical Spine CYRIAXDokument16 SeitenCervical Spine CYRIAXCarlos TavaresNoch keine Bewertungen
- Achilles Tendon Repair Protocol-PDF-EnDokument2 SeitenAchilles Tendon Repair Protocol-PDF-Enckpravin7754Noch keine Bewertungen
- ICF-Ankle Trimalleolar FractureDokument18 SeitenICF-Ankle Trimalleolar FracturedvenumohanNoch keine Bewertungen
- Scapular Dyskinesis PDFDokument24 SeitenScapular Dyskinesis PDFPablo Sentis DiazNoch keine Bewertungen
- KyphosisDokument32 SeitenKyphosisBeniamin CostinașNoch keine Bewertungen
- Shoulder Knee WristDokument110 SeitenShoulder Knee Wriststevebravo81100% (1)
- Upper C Spine FractureDokument54 SeitenUpper C Spine FracturekiranbcNoch keine Bewertungen
- Neck PainDokument1 SeiteNeck PainHasan RahmanNoch keine Bewertungen
- Spine Fractures and Spinal Cord InjuryDokument54 SeitenSpine Fractures and Spinal Cord InjuryAloy PudeNoch keine Bewertungen
- Scoliosis: Degenerative & IdiopathicDokument34 SeitenScoliosis: Degenerative & IdiopathicClaudia MariscaNoch keine Bewertungen
- Hemiarthroplasty Hip - Apr20Dokument10 SeitenHemiarthroplasty Hip - Apr20Shalu OjhaNoch keine Bewertungen
- Spine: HistoryDokument6 SeitenSpine: HistorySham SundarNoch keine Bewertungen
- Knee Biomechanics: Mark Arthur Martinez Trauma 1 April 5, 2018Dokument7 SeitenKnee Biomechanics: Mark Arthur Martinez Trauma 1 April 5, 2018Juan Alvaro EstradaNoch keine Bewertungen
- Achilles RuptureDokument23 SeitenAchilles RupturePhysiotherapist AliNoch keine Bewertungen
- Spine Examination: Mario Johan Heryputra 11.2012.208Dokument29 SeitenSpine Examination: Mario Johan Heryputra 11.2012.208Mario Johan Heryputra100% (1)
- 2018 Hip Program FINALDokument119 Seiten2018 Hip Program FINALJafild Fild riverNoch keine Bewertungen
- Slipped Capital Femoral Epiphysis - SCFEDokument3 SeitenSlipped Capital Femoral Epiphysis - SCFEyosua_edwin100% (1)
- Entrapments CadDokument3 SeitenEntrapments Cadapi-467743065100% (1)
- Cervical Spine Stomatognatic System and CraniofacialDokument40 SeitenCervical Spine Stomatognatic System and CraniofacialDenise MathreNoch keine Bewertungen
- Zones of Hand: Rose Mary AntonyDokument36 SeitenZones of Hand: Rose Mary AntonyFatra FasyaNoch keine Bewertungen
- Dr. Ankit Gujarathi DMH PuneDokument32 SeitenDr. Ankit Gujarathi DMH PuneAnkit GujarathiNoch keine Bewertungen
- Sport Injuries: ShoulderDokument67 SeitenSport Injuries: ShoulderNabiha AjmalNoch keine Bewertungen
- Full Project PDFDokument39 SeitenFull Project PDFmohiiieNoch keine Bewertungen
- Prevelance of Piriformis Syndrome in Chronic Low Back Pain Patients. A Clinical Diagnosis With Modified FAIR Test PainPractice20121 PDFDokument9 SeitenPrevelance of Piriformis Syndrome in Chronic Low Back Pain Patients. A Clinical Diagnosis With Modified FAIR Test PainPractice20121 PDFAuliadi AnsharNoch keine Bewertungen
- Assessment of Back Pain-BMJDokument30 SeitenAssessment of Back Pain-BMJMarco Paulo Reyes NaoeNoch keine Bewertungen
- Red Flag: MSK Services Pathway - Shoulder PathologyDokument11 SeitenRed Flag: MSK Services Pathway - Shoulder PathologyMuhammed ElgasimNoch keine Bewertungen
- Knee BiomechanicsDokument32 SeitenKnee BiomechanicsnishantsinghbmeNoch keine Bewertungen
- Assessment of Posture: Prepared By: Floriza P. de Leon, PTRPDokument17 SeitenAssessment of Posture: Prepared By: Floriza P. de Leon, PTRPFloriza de Leon100% (1)
- Physical Therapy Management of Thoracic Outlet SyndromeDokument4 SeitenPhysical Therapy Management of Thoracic Outlet SyndromeYashaswi ANoch keine Bewertungen
- Rotator Cuff Tears Orthoinfo - Aaos.org TopicDokument7 SeitenRotator Cuff Tears Orthoinfo - Aaos.org TopicMontserrat LandaNoch keine Bewertungen
- Lumbar Spine AssessmentDokument26 SeitenLumbar Spine Assessmentyoyo_pt2007100% (1)
- Bahan Kuliah Fractures in ElderlyDokument27 SeitenBahan Kuliah Fractures in ElderlyhazelelNoch keine Bewertungen
- ShoulderDokument51 SeitenShoulderIts LaraNoch keine Bewertungen
- 香港脊醫 Hong Kong Chiropractors Sep 2016Dokument6 Seiten香港脊醫 Hong Kong Chiropractors Sep 2016CDAHKNoch keine Bewertungen
- Evaluation and Management of Hip Pain An Algorithmic Approach PDFDokument2 SeitenEvaluation and Management of Hip Pain An Algorithmic Approach PDFEulaNoch keine Bewertungen
- Pes Planus - Synopsis of CausationDokument14 SeitenPes Planus - Synopsis of CausationSari HestiyariniNoch keine Bewertungen
- Lower Limb Fracture..MeDokument142 SeitenLower Limb Fracture..MeWorku KifleNoch keine Bewertungen
- Tests of Examination of CervicalDokument10 SeitenTests of Examination of CervicalAde Yahya NasutionNoch keine Bewertungen
- Mask Ventilation During Induction of General Anesthesia: Influences of Obstructive Sleep ApneaDokument11 SeitenMask Ventilation During Induction of General Anesthesia: Influences of Obstructive Sleep ApneaannisaNoch keine Bewertungen
- Allah PatofDokument6 SeitenAllah PatofannisaNoch keine Bewertungen
- Effects of Muscle Relaxants On Mask Ventilation in Anesthetized Persons With Normal Upper Airway AnatomyDokument7 SeitenEffects of Muscle Relaxants On Mask Ventilation in Anesthetized Persons With Normal Upper Airway AnatomyannisaNoch keine Bewertungen
- Dafpus DokkelDokument2 SeitenDafpus DokkelannisaNoch keine Bewertungen
- HBDokument1 SeiteHBannisaNoch keine Bewertungen
- High Intraoperative Inspired Oxygen Does Not Increase Postoperative Supplemental Oxygen RequirementsDokument9 SeitenHigh Intraoperative Inspired Oxygen Does Not Increase Postoperative Supplemental Oxygen RequirementsannisaNoch keine Bewertungen
- Ballard ScoreDokument1 SeiteBallard ScoreFikriyah FuadiyahNoch keine Bewertungen
- MainDokument9 SeitenMainannisaNoch keine Bewertungen
- Jabbar V and 2015Dokument7 SeitenJabbar V and 2015annisaNoch keine Bewertungen
- Finalmodulechronicmalnutrition in Children PDFDokument116 SeitenFinalmodulechronicmalnutrition in Children PDFannisaNoch keine Bewertungen
- Coba Baca 36634-130622-2-PBDokument5 SeitenCoba Baca 36634-130622-2-PBannisaNoch keine Bewertungen
- Ticagrelor Versus Aspirin in Acute Stroke or Transient Ischemic AttackDokument9 SeitenTicagrelor Versus Aspirin in Acute Stroke or Transient Ischemic AttackTara WandhitaNoch keine Bewertungen
- Case 45279-86917-1-SMDokument4 SeitenCase 45279-86917-1-SMannisaNoch keine Bewertungen
- Prevention of Endophthalmitis: Kurt Buzard, MD, Stergios Liapis, MDDokument7 SeitenPrevention of Endophthalmitis: Kurt Buzard, MD, Stergios Liapis, MDannisaNoch keine Bewertungen
- Endophthalmitis: Major ReviewDokument5 SeitenEndophthalmitis: Major ReviewannisaNoch keine Bewertungen
- Coba Baca 456209Dokument8 SeitenCoba Baca 456209annisaNoch keine Bewertungen
- Clinical Study: Outcome and Prognostic Factors For Traumatic Endophthalmitis Over A 5-Year PeriodDokument8 SeitenClinical Study: Outcome and Prognostic Factors For Traumatic Endophthalmitis Over A 5-Year PeriodannisaNoch keine Bewertungen
- Lapscopy 3Dokument5 SeitenLapscopy 3Dinika DinNoch keine Bewertungen
- Risk Factors For Otitis Media in ChildrenDokument6 SeitenRisk Factors For Otitis Media in ChildrenRisandy DitiaNoch keine Bewertungen
- Melatonin Amiptriptilin and PlaceboDokument7 SeitenMelatonin Amiptriptilin and PlaceboannisaNoch keine Bewertungen
- Patient Outcomes 15 Years PoststrokeDokument9 SeitenPatient Outcomes 15 Years PoststrokeannisaNoch keine Bewertungen
- Nej Mo A 1506930Dokument11 SeitenNej Mo A 1506930chemptnkNoch keine Bewertungen
- J Neurol Neurosurg Psychiatry 2016 Firbank JNNP 2016 313918Dokument8 SeitenJ Neurol Neurosurg Psychiatry 2016 Firbank JNNP 2016 313918annisaNoch keine Bewertungen
- J Neurol Neurosurg Psychiatry 2016 Hedström 454 60Dokument8 SeitenJ Neurol Neurosurg Psychiatry 2016 Hedström 454 60annisaNoch keine Bewertungen
- Gestational Diabetes Mellitus: Science in MedicineDokument7 SeitenGestational Diabetes Mellitus: Science in MedicineannisaNoch keine Bewertungen
- 4.4.7.5 Apec PDM Guidelines 3-25-13Dokument11 Seiten4.4.7.5 Apec PDM Guidelines 3-25-13annisaNoch keine Bewertungen
- Morport 5 Sept - 6 Sept 2016Dokument19 SeitenMorport 5 Sept - 6 Sept 2016annisaNoch keine Bewertungen
- 1039 Full PDFDokument19 Seiten1039 Full PDFannisaNoch keine Bewertungen
- Consequences of Gestational and Pregestational Diabetes On Placental Function and Birth WeightDokument8 SeitenConsequences of Gestational and Pregestational Diabetes On Placental Function and Birth WeightannisaNoch keine Bewertungen
- 4.4.7.5 Apec PDM Guidelines 3-25-13Dokument11 Seiten4.4.7.5 Apec PDM Guidelines 3-25-13annisaNoch keine Bewertungen
- TreesDokument69 SeitenTreesADITYA GEHLAWATNoch keine Bewertungen
- A Year On A FarmDokument368 SeitenA Year On A FarmvehapkolaNoch keine Bewertungen
- Assignment 2 Mat435Dokument2 SeitenAssignment 2 Mat435Arsene LupinNoch keine Bewertungen
- Keiilf: Training ManualDokument53 SeitenKeiilf: Training ManualGary GouveiaNoch keine Bewertungen
- Niir Integrated Organic Farming Handbook PDFDokument13 SeitenNiir Integrated Organic Farming Handbook PDFNatalieNoch keine Bewertungen
- Hopeless PlacesDokument1.304 SeitenHopeless Placesmoreblessingmarvellous659Noch keine Bewertungen
- Updated Factory Profile of Aleya Apparels LTDDokument25 SeitenUpdated Factory Profile of Aleya Apparels LTDJahangir Hosen0% (1)
- EXP4 The Diels Alder ReactionsDokument3 SeitenEXP4 The Diels Alder ReactionsLaura GuidoNoch keine Bewertungen
- Improve On-Time DeliveriesDokument24 SeitenImprove On-Time DeliveriesUdayNoch keine Bewertungen
- Solutions GoldsteinDokument10 SeitenSolutions GoldsteinAnyiNoch keine Bewertungen
- AssessmentDokument9 SeitenAssessmentJuan Miguel Sapad AlpañoNoch keine Bewertungen
- Safe Lorry Loader Crane OperationsDokument4 SeitenSafe Lorry Loader Crane Operationsjdmultimodal sdn bhdNoch keine Bewertungen
- Provision of EPCI Services For EPCIC Sidayu Wellhead Platforms and Pipelines Sidayu Field DevelopmentDokument7 SeitenProvision of EPCI Services For EPCIC Sidayu Wellhead Platforms and Pipelines Sidayu Field Developmentriandi100% (1)
- MarbiehistoryDokument6 SeitenMarbiehistoryMarbie DalanginNoch keine Bewertungen
- Awakened Citizen Programme-Report-class VII-2014Dokument4 SeitenAwakened Citizen Programme-Report-class VII-2014bhsgeneral r m saraswathi50% (4)
- Owner'S Manual: 2023 Chassis CabDokument444 SeitenOwner'S Manual: 2023 Chassis CabDmitry DimasNoch keine Bewertungen
- FRP Handrail Fittings CatalogDokument6 SeitenFRP Handrail Fittings CatalogAl Adel MorenoNoch keine Bewertungen
- American BreakfastDokument4 SeitenAmerican BreakfastHamilton Valenzuela ChipongianNoch keine Bewertungen
- SambongDokument3 SeitenSambongNica Del GallegoNoch keine Bewertungen
- The Acceptability of Rubber Tree Sap (A As An Alternative Roof SealantDokument7 SeitenThe Acceptability of Rubber Tree Sap (A As An Alternative Roof SealantHannilyn Caldeo100% (2)
- 41z S4hana2021 Set-Up en XXDokument46 Seiten41z S4hana2021 Set-Up en XXHussain MulthazimNoch keine Bewertungen
- Ficha Tecnica-Skyjack SJ3219 8mtDokument2 SeitenFicha Tecnica-Skyjack SJ3219 8mtLESLY MILENA MORENO CORALNoch keine Bewertungen
- Inverse of One-To-One FunctionDokument4 SeitenInverse of One-To-One FunctionKathFaye EdaNoch keine Bewertungen
- Potassium Fixation As Affected by Alternate Wetting and Drying in Some Soil Series of JharkhandDokument4 SeitenPotassium Fixation As Affected by Alternate Wetting and Drying in Some Soil Series of JharkhandDr Amrit Kumar JhaNoch keine Bewertungen
- Assessment Questions: 1: Wash - Rinse and SanitizeDokument3 SeitenAssessment Questions: 1: Wash - Rinse and SanitizeAna Margarita AycochoNoch keine Bewertungen
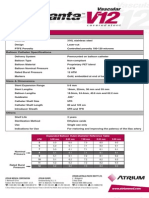
- Advanta V12 Data SheetDokument2 SeitenAdvanta V12 Data SheetJuliana MiyagiNoch keine Bewertungen
- Contemporary Philippine Arts From The Regions: Quarter 2 - Module 9 Different Contemporary Art Techniques and PerformanceDokument25 SeitenContemporary Philippine Arts From The Regions: Quarter 2 - Module 9 Different Contemporary Art Techniques and PerformanceGrace06 Labin100% (7)
- Oil Whirl and Whip Instabilities - Within Journal BearingsDokument27 SeitenOil Whirl and Whip Instabilities - Within Journal BearingsTalha AamirNoch keine Bewertungen
- Sales 20: Years Advertising Expense (Millions) X Sales (Thousands) yDokument8 SeitenSales 20: Years Advertising Expense (Millions) X Sales (Thousands) ybangNoch keine Bewertungen
- Food Taste Panel Evaluation Form 2Dokument17 SeitenFood Taste Panel Evaluation Form 2Akshat JainNoch keine Bewertungen
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Von EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Bewertung: 3 von 5 Sternen3/5 (1)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDVon EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDBewertung: 5 von 5 Sternen5/5 (2)
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (29)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionVon EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionBewertung: 4 von 5 Sternen4/5 (404)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsVon EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNoch keine Bewertungen
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedBewertung: 5 von 5 Sternen5/5 (81)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeVon EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeBewertung: 2 von 5 Sternen2/5 (1)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessVon EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessBewertung: 4.5 von 5 Sternen4.5/5 (328)
- The Obesity Code: Unlocking the Secrets of Weight LossVon EverandThe Obesity Code: Unlocking the Secrets of Weight LossBewertung: 4 von 5 Sternen4/5 (6)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaVon EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisVon EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisBewertung: 4.5 von 5 Sternen4.5/5 (42)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsVon EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsBewertung: 3.5 von 5 Sternen3.5/5 (3)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsVon EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsBewertung: 5 von 5 Sternen5/5 (1)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeVon EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeBewertung: 4.5 von 5 Sternen4.5/5 (253)
- The Comfort of Crows: A Backyard YearVon EverandThe Comfort of Crows: A Backyard YearBewertung: 4.5 von 5 Sternen4.5/5 (23)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Von EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Bewertung: 4.5 von 5 Sternen4.5/5 (110)
- Why We Die: The New Science of Aging and the Quest for ImmortalityVon EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityBewertung: 4 von 5 Sternen4/5 (5)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisVon EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisBewertung: 4 von 5 Sternen4/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryVon EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryBewertung: 4 von 5 Sternen4/5 (45)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsVon EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsBewertung: 4.5 von 5 Sternen4.5/5 (170)
- Summary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedBewertung: 4 von 5 Sternen4/5 (61)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesVon EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesBewertung: 4.5 von 5 Sternen4.5/5 (1412)
- How to ADHD: The Ultimate Guide and Strategies for Productivity and Well-BeingVon EverandHow to ADHD: The Ultimate Guide and Strategies for Productivity and Well-BeingBewertung: 1 von 5 Sternen1/5 (1)
- The Marshmallow Test: Mastering Self-ControlVon EverandThe Marshmallow Test: Mastering Self-ControlBewertung: 4.5 von 5 Sternen4.5/5 (59)