Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- M5 - Talons of NightDokument54 SeitenM5 - Talons of NightThiago PedrozaNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Neuroscience - A Historical Introduction by Mitchell Glickstein PDFDokument418 SeitenNeuroscience - A Historical Introduction by Mitchell Glickstein PDFjavaldezr100% (2)
- Lecture Notes For Introduction To Safety and Health PDFDokument216 SeitenLecture Notes For Introduction To Safety and Health PDFTeshome Dengiso100% (1)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Abortion II ND Yr MSC NursingDokument121 SeitenAbortion II ND Yr MSC Nursingesthereugenia100% (1)
- MigraineDokument38 SeitenMigraineManju PriyaNoch keine Bewertungen
- Fermented BiocharDokument81 SeitenFermented Biocharstar662100% (1)
- Essentials 4eDokument874 SeitenEssentials 4eJehada AbdukadilNoch keine Bewertungen
- Ocumentation: Analysis of The Situation and Trends in Sunscreen ProductsDokument4 SeitenOcumentation: Analysis of The Situation and Trends in Sunscreen ProductsEvelyn GómezNoch keine Bewertungen
- Second Announcement JASS RevisiDokument28 SeitenSecond Announcement JASS RevisiPoco BlueNoch keine Bewertungen
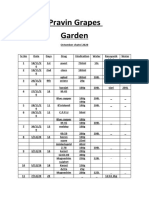
- Pravin Grapes Garden Octomber chatni 2020 recordsDokument9 SeitenPravin Grapes Garden Octomber chatni 2020 recordsPravin ShindeNoch keine Bewertungen
- Dr. Sterling Clarren Retirement AnnouncementDokument1 SeiteDr. Sterling Clarren Retirement AnnouncementfasdunitedNoch keine Bewertungen
- 11 Examples of Japanese Etiquette That Would Drive Us Crazy: 11. Addressing PeopleDokument9 Seiten11 Examples of Japanese Etiquette That Would Drive Us Crazy: 11. Addressing PeopleJuliooooNoch keine Bewertungen
- Novel Alzheimer's Drug Targets Multiple PathwaysDokument4 SeitenNovel Alzheimer's Drug Targets Multiple PathwaysIndra HedarNoch keine Bewertungen
- Causas de Pancitopenia Canina y FelinaDokument12 SeitenCausas de Pancitopenia Canina y FelinaMarisol AsakuraNoch keine Bewertungen
- Hyperbaric Oxygen Therapy For A Pediatric Electrical BurnDokument3 SeitenHyperbaric Oxygen Therapy For A Pediatric Electrical Burnsarah iriamanaNoch keine Bewertungen
- Shalini Yerukala, Et AlDokument12 SeitenShalini Yerukala, Et AlKian BaulaNoch keine Bewertungen
- LRD DIV SPE FM 001a RITM Lab Test Request Form - Clinical Lab 1Dokument1 SeiteLRD DIV SPE FM 001a RITM Lab Test Request Form - Clinical Lab 1Megen PLCNoch keine Bewertungen
- Revised syllabus for anatomy and physiology coursesDokument40 SeitenRevised syllabus for anatomy and physiology coursesSrikutty DevuNoch keine Bewertungen
- Gestational Hypertension and Preeclampsia ACOG Practice Bulletin, Number 222 1605448006Dokument24 SeitenGestational Hypertension and Preeclampsia ACOG Practice Bulletin, Number 222 1605448006xibalba.edNoch keine Bewertungen
- The Human Body Frequency: March 2020Dokument3 SeitenThe Human Body Frequency: March 2020Dejya CordoraNoch keine Bewertungen
- (Developments in Plant Pathology 1) Roy Johnson (Auth.), R. Johnson, G. J. Jellis (Eds.) - Breeding For Disease Resistance-Springer Netherlands (1992)Dokument199 Seiten(Developments in Plant Pathology 1) Roy Johnson (Auth.), R. Johnson, G. J. Jellis (Eds.) - Breeding For Disease Resistance-Springer Netherlands (1992)Sultan Ahmad KhanNoch keine Bewertungen
- Full Report A-1Dokument35 SeitenFull Report A-1assssadfNoch keine Bewertungen
- Boron DeficiencyDokument2 SeitenBoron DeficiencyManu MandaNoch keine Bewertungen
- The Thalidomide HistoryDokument11 SeitenThe Thalidomide HistoryJesus VuelvasNoch keine Bewertungen
- Discrimination Resource Dec. 2020Dokument33 SeitenDiscrimination Resource Dec. 2020Fiorella CastilloNoch keine Bewertungen
- Routine Medical Checkup PublicationDokument11 SeitenRoutine Medical Checkup Publication백만호Noch keine Bewertungen
- Reading - Age With Moderate DehydrationDokument8 SeitenReading - Age With Moderate DehydrationSophia IbuyanNoch keine Bewertungen
- Managing Medical and Pharmacological CareDokument33 SeitenManaging Medical and Pharmacological CareZNEROLNoch keine Bewertungen
- Retraction: Retracted: Detection of Abnormal Hemoglobin Variants by HPLC Method: Common Problems With Suggested SolutionsDokument11 SeitenRetraction: Retracted: Detection of Abnormal Hemoglobin Variants by HPLC Method: Common Problems With Suggested SolutionsHaziq WahidNoch keine Bewertungen
- Aura ArticleDokument6 SeitenAura ArticleDharmaMaya ChandrahasNoch keine Bewertungen