Das könnte Ihnen auch gefallen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Common Cardiac MedicationsDokument1 SeiteCommon Cardiac MedicationsPaige HardekopfNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- IFIC Basic Concepts of Infection ControlDokument196 SeitenIFIC Basic Concepts of Infection ControlYULI22280% (5)
- Admission and DischargeDokument4 SeitenAdmission and DischargeTribhuwan KushwahaNoch keine Bewertungen
- Adaptive Method For SchizoidsDokument3 SeitenAdaptive Method For SchizoidsAntxon7850% (2)
- A Century of Influence - Part 1. Orthodontic PioneersDokument6 SeitenA Century of Influence - Part 1. Orthodontic PioneersmutansNoch keine Bewertungen
- Gastrointestinal MCQDokument25 SeitenGastrointestinal MCQLương Thế Đoàn100% (2)
- How To Conduct A Mock TracerDokument10 SeitenHow To Conduct A Mock Tracerngurah_wardana100% (1)
- 58f6anesthesia For Laparoscopic SurgeriesDokument56 Seiten58f6anesthesia For Laparoscopic SurgeriesSayed NourNoch keine Bewertungen
- Inference Based Therapy Fo BDD PDFDokument10 SeitenInference Based Therapy Fo BDD PDFGeniefe VivendaNoch keine Bewertungen
- HepatitisDokument8 SeitenHepatitisudaybujjiNoch keine Bewertungen
- Various Intrusive ArchsDokument10 SeitenVarious Intrusive ArchsmutansNoch keine Bewertungen
- Krohn v. CADokument2 SeitenKrohn v. CAKaren PanisalesNoch keine Bewertungen
- The 6-Elements Orthodontic PhilosophyDokument5 SeitenThe 6-Elements Orthodontic PhilosophymutansNoch keine Bewertungen
- Upper Midline CorrectionDokument5 SeitenUpper Midline CorrectionmutansNoch keine Bewertungen
- Gingiva and Orthodontic Treatment PDFDokument15 SeitenGingiva and Orthodontic Treatment PDFmutansNoch keine Bewertungen
- Dentition and Occlusal Development in ChildrenDokument9 SeitenDentition and Occlusal Development in ChildrenmutansNoch keine Bewertungen
- Orthodontically Induced Inflammatory Root ResorptionDokument15 SeitenOrthodontically Induced Inflammatory Root ResorptionmutansNoch keine Bewertungen
- NullDokument11 SeitenNullapi-26468957Noch keine Bewertungen
- Ideal Arch Force Systems - A Center-Of-resistance PerspectiveDokument9 SeitenIdeal Arch Force Systems - A Center-Of-resistance PerspectivemutansNoch keine Bewertungen
- CL II SubDokument6 SeitenCL II SubmutansNoch keine Bewertungen
- Biomechanics Chapter1Dokument11 SeitenBiomechanics Chapter1mutansNoch keine Bewertungen
- Conduct DisorderDokument7 SeitenConduct DisorderSenka Nenadov100% (1)
- Ivp Dari WikipediaDokument6 SeitenIvp Dari Wikipediabellatrix orionNoch keine Bewertungen
- Fulminant Hepatic FailureDokument9 SeitenFulminant Hepatic FailurerazerxxxNoch keine Bewertungen
- Therapeutic Relationships and Communication Skills Assignment 1Dokument6 SeitenTherapeutic Relationships and Communication Skills Assignment 1api-238869728Noch keine Bewertungen
- Strickland PresentationDokument1 SeiteStrickland Presentationmariopi2495Noch keine Bewertungen
- J Am Dent Assoc 2003 Christens en 241 3Dokument3 SeitenJ Am Dent Assoc 2003 Christens en 241 3Steffi Setiawan PrawokoNoch keine Bewertungen
- Therapy in TuberculosisDokument4 SeitenTherapy in TuberculosisSamir SkejicNoch keine Bewertungen
- Obstetric Abdominal Examination OSCE GuideDokument16 SeitenObstetric Abdominal Examination OSCE GuideMuhammad Aamir IqbalNoch keine Bewertungen
- Temporo-Mandibular Joint Complex Exercise SuggestionsDokument9 SeitenTemporo-Mandibular Joint Complex Exercise SuggestionsClaudia LeperaNoch keine Bewertungen
- Lap InstrumentsDokument7 SeitenLap InstrumentskhaleeltahaNoch keine Bewertungen
- Presented By: Don Leo M Dela Pe A BSN Ii-BDokument17 SeitenPresented By: Don Leo M Dela Pe A BSN Ii-BDon Leo Dela PeñaNoch keine Bewertungen
- PDSA Examples: PlanDokument6 SeitenPDSA Examples: PlanTrà My Lê MỹNoch keine Bewertungen
- DCB Canhao Sho2012 AbDokument508 SeitenDCB Canhao Sho2012 Abford027Noch keine Bewertungen
- Chapter 38:: Urticaria and Angioedema:: Allen P. KaplanDokument2 SeitenChapter 38:: Urticaria and Angioedema:: Allen P. KaplanSyamsi KubangunNoch keine Bewertungen
- Patogenesis TBDokument46 SeitenPatogenesis TBJaya Semara PutraNoch keine Bewertungen
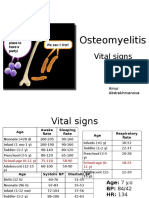
- PBL 2 - OsteomyelitisDokument10 SeitenPBL 2 - OsteomyelitisAinur AbdrakhmanovaNoch keine Bewertungen
- Dlau LVN Resume 1Dokument1 SeiteDlau LVN Resume 1api-571772305Noch keine Bewertungen
- Revised Instrument Packet 2Dokument44 SeitenRevised Instrument Packet 2Abdiaziz Walhad0% (1)
- 5 Vol3 Issue3 MS 15175Dokument8 Seiten5 Vol3 Issue3 MS 15175kanna_dhasan25581Noch keine Bewertungen