Das könnte Ihnen auch gefallen
- USMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsVon EverandUSMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsBewertung: 5 von 5 Sternen5/5 (9)
- Brittney Gilliam, Et Al., v. City of Aurora, Et Al.Dokument42 SeitenBrittney Gilliam, Et Al., v. City of Aurora, Et Al.Michael_Roberts2019Noch keine Bewertungen
- Clinical Management Review 2023-2024: Volume 1: USMLE Step 3 and COMLEX-USA Level 3Von EverandClinical Management Review 2023-2024: Volume 1: USMLE Step 3 and COMLEX-USA Level 3Bewertung: 5 von 5 Sternen5/5 (1)
- Nicolas-Lewis vs. ComelecDokument3 SeitenNicolas-Lewis vs. ComelecJessamine OrioqueNoch keine Bewertungen
- ASRM COVID-19 Vaccine GuidanceDokument4 SeitenASRM COVID-19 Vaccine GuidancePatricia FernándezNoch keine Bewertungen
- Paul Smith - Discerning The SubjectDokument226 SeitenPaul Smith - Discerning The SubjectdisconnectaNoch keine Bewertungen
- Germ TheoryDokument15 SeitenGerm TheoryjackjugNoch keine Bewertungen
- Adult Combined ScheduleDokument5 SeitenAdult Combined SchedulelcmurilloNoch keine Bewertungen
- Adult Immunization Schedule and RecommendationsDokument3 SeitenAdult Immunization Schedule and RecommendationsdrmanojvimalNoch keine Bewertungen
- Adult Immunization ScheduleDokument3 SeitenAdult Immunization ScheduleBryan Mae H. DegorioNoch keine Bewertungen
- Adult Pocafeket SizeDokument2 SeitenAdult Pocafeket SizedadfNoch keine Bewertungen
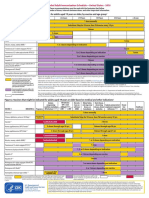
- Figure 1. Recommended Immunization Schedule For Adults Aged 19 Years or Older, by Vaccine and Age GroupDokument2 SeitenFigure 1. Recommended Immunization Schedule For Adults Aged 19 Years or Older, by Vaccine and Age GroupmsarasNoch keine Bewertungen
- Adult ScheduleDokument3 SeitenAdult SchedulelcmurilloNoch keine Bewertungen
- Adult Schedule 11x17Dokument2 SeitenAdult Schedule 11x17lcmurilloNoch keine Bewertungen
- Vacunas 2012Dokument7 SeitenVacunas 2012dr.alexisleon9124Noch keine Bewertungen
- States, 2011 United Recommended Childhood and Adolescent Immunization SchedulesDokument7 SeitenStates, 2011 United Recommended Childhood and Adolescent Immunization SchedulesDolores KilpatrickNoch keine Bewertungen
- CDC adult immunization schedule recommendationsDokument33 SeitenCDC adult immunization schedule recommendationshatsuneNoch keine Bewertungen
- Adult Combined ScheduleDokument6 SeitenAdult Combined ScheduleAstrid Elaine RosalesNoch keine Bewertungen
- Practice Changing UpDates - UpToDateDokument13 SeitenPractice Changing UpDates - UpToDatemayteveronica1000Noch keine Bewertungen
- Summary of Recommendations For Adult Immunization: (Age 19 Years & Older)Dokument4 SeitenSummary of Recommendations For Adult Immunization: (Age 19 Years & Older)gyna_2002Noch keine Bewertungen
- ScheduleDokument2 SeitenScheduleapi-286634335Noch keine Bewertungen
- The Sinovac VaccineDokument4 SeitenThe Sinovac VaccineMontasir BalambagNoch keine Bewertungen
- Vaccination Requirements and Form I-693: Mary Naughton, MD, MPHDokument55 SeitenVaccination Requirements and Form I-693: Mary Naughton, MD, MPHErinaNoch keine Bewertungen
- Immunization Programs For Infants, Children, Adolescents, and Adults: Clinical Practice Guidelines by The Infectious Diseases Society of AmericaDokument24 SeitenImmunization Programs For Infants, Children, Adolescents, and Adults: Clinical Practice Guidelines by The Infectious Diseases Society of AmericaEugene YeboahNoch keine Bewertungen
- COVID-19 Vaccine in Patients With Haematological Disorders British Society For HaematologyDokument10 SeitenCOVID-19 Vaccine in Patients With Haematological Disorders British Society For HaematologydrToikNoch keine Bewertungen
- BIMA Oxford AZ Vaccine Detailed Position StatementDokument5 SeitenBIMA Oxford AZ Vaccine Detailed Position StatementVegha NedyaNoch keine Bewertungen
- Recommended Immunizations FS enDokument2 SeitenRecommended Immunizations FS enirfanmajeed1987Noch keine Bewertungen
- 07 Childschd 6x4.5 1-Page PRDokument2 Seiten07 Childschd 6x4.5 1-Page PRSteluta GalbenusNoch keine Bewertungen
- MMWR HiB PDFDokument20 SeitenMMWR HiB PDFworksheetbookNoch keine Bewertungen
- WHO 2019 NCoV Vaccines SAGE Recommendation Sinovac CoronaVac 2021.1 EngDokument7 SeitenWHO 2019 NCoV Vaccines SAGE Recommendation Sinovac CoronaVac 2021.1 EngMartha Gatica GuevaraNoch keine Bewertungen
- Clinical Guideline: Recommended Adult Immunization Schedule: United States, 2011Dokument8 SeitenClinical Guideline: Recommended Adult Immunization Schedule: United States, 2011Hery PriyantoNoch keine Bewertungen
- CDC Vaccination Program for U.S.-bound RefugeesDokument4 SeitenCDC Vaccination Program for U.S.-bound RefugeesPedro Julian Tenorio ApesteguiNoch keine Bewertungen
- WHO Immunization RecommendationsDokument9 SeitenWHO Immunization RecommendationsMeeKo VideñaNoch keine Bewertungen
- Protocolo CanadaDokument5 SeitenProtocolo Canadashluly23Noch keine Bewertungen
- iNMUNIZACIONES Adulto ACIP2022 aNNALSDokument14 SeiteniNMUNIZACIONES Adulto ACIP2022 aNNALSEmilio Ulises Napoles LealNoch keine Bewertungen
- Complete Summary: Guideline TitleDokument30 SeitenComplete Summary: Guideline TitleAlexandre MedeirosNoch keine Bewertungen
- WHO 2019 nCoV Vaccines SAGE Recommendation BIBP 2021.1 EngDokument7 SeitenWHO 2019 nCoV Vaccines SAGE Recommendation BIBP 2021.1 EngDiane LigmanNoch keine Bewertungen
- Adult Immunization: It's Your Best Shot!Dokument40 SeitenAdult Immunization: It's Your Best Shot!minerva_stanciuNoch keine Bewertungen
- Guidelines for Vaccination in Normal Adults in India - PMCDokument14 SeitenGuidelines for Vaccination in Normal Adults in India - PMCSKMH INSURANCENoch keine Bewertungen
- InfuenzaDokument30 SeitenInfuenzaChandra_INHU_RiauNoch keine Bewertungen
- Adult Immunization Recommendations SummaryDokument5 SeitenAdult Immunization Recommendations SummaryHannah Caburian RemoNoch keine Bewertungen
- Human Papillomavirus Bivalent Vaccin1Dokument8 SeitenHuman Papillomavirus Bivalent Vaccin1alejandro fernandezNoch keine Bewertungen
- SOGC Guideline on Immunization in PregnancyDokument6 SeitenSOGC Guideline on Immunization in PregnancyMohamed SulimanNoch keine Bewertungen
- ImmunizationsDokument2 SeitenImmunizationsSonny KusumaNoch keine Bewertungen
- Annex 48 Clinical Guidelines For Covid in Malaysia 4th Edition 19102021 FinaleDokument175 SeitenAnnex 48 Clinical Guidelines For Covid in Malaysia 4th Edition 19102021 FinaleEfendi AnuarNoch keine Bewertungen
- HPV Vaccination Recommendations Updated for Adults Through Age 26Dokument5 SeitenHPV Vaccination Recommendations Updated for Adults Through Age 26Tiara RahmanandaNoch keine Bewertungen
- What's New On The Child and Adolescent Immunization SchedulesDokument30 SeitenWhat's New On The Child and Adolescent Immunization SchedulesMark ReinhardtNoch keine Bewertungen
- Public FAQDokument15 SeitenPublic FAQIan WeberNoch keine Bewertungen
- Antiviral Summary ClinicianDokument20 SeitenAntiviral Summary ClinicianPurpleeyoreNoch keine Bewertungen
- 2006 118 1774 Subcommittee On Diagnosis and Management of BronchiolitisDokument22 Seiten2006 118 1774 Subcommittee On Diagnosis and Management of BronchiolitisAuliaRahmanNoch keine Bewertungen
- 2006 118 1774-1793 Subcommittee On Diagnosis and Management of BronchiolitisDokument22 Seiten2006 118 1774-1793 Subcommittee On Diagnosis and Management of BronchiolitisAlejandra Castro Salas エールNoch keine Bewertungen
- Annals of Medicine - HPV VaccineDokument12 SeitenAnnals of Medicine - HPV VaccineJudicial Watch, Inc.100% (3)
- Guia de Vacunacion FelinaDokument5 SeitenGuia de Vacunacion FelinaRaul KimNoch keine Bewertungen
- 2019 Guide For ImmunizationDokument195 Seiten2019 Guide For ImmunizationReigner paul DavidNoch keine Bewertungen
- Research Paper in English: Perception On COVID-19 Vaccines of Residents in Barangay Canlapwas, Pagsanghan SamarDokument10 SeitenResearch Paper in English: Perception On COVID-19 Vaccines of Residents in Barangay Canlapwas, Pagsanghan SamarDivina CacheroNoch keine Bewertungen
- Antiviral Summary Clinicians InfluenzaDokument8 SeitenAntiviral Summary Clinicians InfluenzaSylvia GonzalezNoch keine Bewertungen
- Guidelines for HIV Treatment: Lab Tests and Drug ResistanceDokument48 SeitenGuidelines for HIV Treatment: Lab Tests and Drug ResistanceAgus OrtNoch keine Bewertungen
- Recommended Childhood and Adolescent Immunization Schedule: United States, 2020Dokument5 SeitenRecommended Childhood and Adolescent Immunization Schedule: United States, 2020nanaNoch keine Bewertungen
- Can You Outline in A Few Sentences What Gardasil Does? and Why It Is Administered To 13 Year Olds?Dokument6 SeitenCan You Outline in A Few Sentences What Gardasil Does? and Why It Is Administered To 13 Year Olds?api-249115191Noch keine Bewertungen
- Guidelines for HIV TreatmentDokument132 SeitenGuidelines for HIV TreatmentAlvi MuldaniNoch keine Bewertungen
- AA Tables PDFDokument133 SeitenAA Tables PDFRafaelNoch keine Bewertungen
- General Recs PDFDokument197 SeitenGeneral Recs PDFLupe BeltranNoch keine Bewertungen
- The Vaccine Handbook: A Practical Guide for Clinicians, Twelfth EditionVon EverandThe Vaccine Handbook: A Practical Guide for Clinicians, Twelfth EditionNoch keine Bewertungen
- To Aipki 22 Juli 2017 Lokasi Undip PDFDokument79 SeitenTo Aipki 22 Juli 2017 Lokasi Undip PDFVennia Riskia TristiantiNoch keine Bewertungen
- The Relationship Between Nephrolithiasis Risk With Body Fat Measured by Body Composition Analyzer in Obese PeopleDokument4 SeitenThe Relationship Between Nephrolithiasis Risk With Body Fat Measured by Body Composition Analyzer in Obese PeopleAwal Safar MNoch keine Bewertungen
- 10 1097@01 JAA 0000522145 52305 AaDokument2 Seiten10 1097@01 JAA 0000522145 52305 AaAwal Safar M100% (1)
- 10.1007@s00296 017 3788 0 PDFDokument8 Seiten10.1007@s00296 017 3788 0 PDFAwal Safar MNoch keine Bewertungen
- 0 18yrs Child Combined ScheduleDokument6 Seiten0 18yrs Child Combined ScheduleAwal Safar MNoch keine Bewertungen
- Referensi 10 - Pleural Effusion - Background, Anatomy, EtiologyDokument6 SeitenReferensi 10 - Pleural Effusion - Background, Anatomy, EtiologyAwal Safar MNoch keine Bewertungen
- Original Article: Postmenopausal Hormone and The Risk of Nephrolithiasis: A Meta-AnalysisDokument9 SeitenOriginal Article: Postmenopausal Hormone and The Risk of Nephrolithiasis: A Meta-AnalysisAwal Safar MNoch keine Bewertungen
- Personal Branding dan Positioning Mempengaruhi Perilaku Pemilih di Kabupaten Bone BolangoDokument17 SeitenPersonal Branding dan Positioning Mempengaruhi Perilaku Pemilih di Kabupaten Bone BolangoMuhammad Irfan BasriNoch keine Bewertungen
- DU - BSC (H) CS BookletDokument121 SeitenDU - BSC (H) CS BookletNagendra DuhanNoch keine Bewertungen
- Course Outline IST110Dokument4 SeitenCourse Outline IST110zaotrNoch keine Bewertungen
- Evidence Law PDFDokument15 SeitenEvidence Law PDFwanborNoch keine Bewertungen
- All Projects Should Be Typed On A4 SheetsDokument3 SeitenAll Projects Should Be Typed On A4 SheetsNikita AgrawalNoch keine Bewertungen
- A Systematic Literature Review of Empirical Research On ChatGPT in EducationDokument23 SeitenA Systematic Literature Review of Empirical Research On ChatGPT in Educationgraciduttra.profNoch keine Bewertungen
- Existentialism Is A HumanismDokument4 SeitenExistentialism Is A HumanismAlex MendezNoch keine Bewertungen
- As 3778.6.3-1992 Measurement of Water Flow in Open Channels Measuring Devices Instruments and Equipment - CalDokument7 SeitenAs 3778.6.3-1992 Measurement of Water Flow in Open Channels Measuring Devices Instruments and Equipment - CalSAI Global - APACNoch keine Bewertungen
- 2009 IBP ElectionsDokument77 Seiten2009 IBP ElectionsBaldovino VenturesNoch keine Bewertungen
- Signal WordsDokument2 SeitenSignal WordsJaol1976Noch keine Bewertungen
- Notes On Statement AssumptionDokument5 SeitenNotes On Statement Assumptionsangamesh mbNoch keine Bewertungen
- Great Mobile Application Requirement Document: 7 Steps To Write ADokument11 SeitenGreat Mobile Application Requirement Document: 7 Steps To Write AgpchariNoch keine Bewertungen
- Corneal Ulcers: What Is The Cornea?Dokument1 SeiteCorneal Ulcers: What Is The Cornea?me2_howardNoch keine Bewertungen
- Ardipithecus Ramidus Is A Hominin Species Dating To Between 4.5 and 4.2 Million Years AgoDokument5 SeitenArdipithecus Ramidus Is A Hominin Species Dating To Between 4.5 and 4.2 Million Years AgoBianca IrimieNoch keine Bewertungen
- Ass 3 MGT206 11.9.2020Dokument2 SeitenAss 3 MGT206 11.9.2020Ashiqur RahmanNoch keine Bewertungen
- A Study of Outdoor Interactional Spaces in High-Rise HousingDokument13 SeitenA Study of Outdoor Interactional Spaces in High-Rise HousingRekha TanpureNoch keine Bewertungen
- Week C - Fact Vs OpinionDokument7 SeitenWeek C - Fact Vs OpinionCharline A. Radislao100% (1)
- Problems of Education in The 21st Century, Vol. 78, No. 4, 2020Dokument199 SeitenProblems of Education in The 21st Century, Vol. 78, No. 4, 2020Scientia Socialis, Ltd.Noch keine Bewertungen
- Influence of Contours On ArchitectureDokument68 SeitenInfluence of Contours On Architecture蘇蘇Noch keine Bewertungen
- Araminta Spook My Haunted House ExtractDokument14 SeitenAraminta Spook My Haunted House Extractsenuthmi dihansaNoch keine Bewertungen
- Masala Kitchen Menus: Chowpatty ChatDokument6 SeitenMasala Kitchen Menus: Chowpatty ChatAlex ShparberNoch keine Bewertungen
- ECON 121 Principles of MacroeconomicsDokument3 SeitenECON 121 Principles of MacroeconomicssaadianaveedNoch keine Bewertungen
- 01 Oh OverviewDokument50 Seiten01 Oh OverviewJaidil YakopNoch keine Bewertungen
- Earth-Song WorksheetDokument2 SeitenEarth-Song WorksheetMuhammad FarizNoch keine Bewertungen
- Rak Single DentureDokument48 SeitenRak Single Denturerakes0Noch keine Bewertungen
- So Neither or NorDokument2 SeitenSo Neither or NorMita KusniasariNoch keine Bewertungen