Beruflich Dokumente
Kultur Dokumente
Tumores de Celulas Germinales
Hochgeladen von
Rabi Armando Aranda OntiverosCopyright
Verfügbare Formate
Dieses Dokument teilen
Dokument teilen oder einbetten
Stufen Sie dieses Dokument als nützlich ein?
Sind diese Inhalte unangemessen?
Dieses Dokument meldenCopyright:
Verfügbare Formate
Tumores de Celulas Germinales
Hochgeladen von
Rabi Armando Aranda OntiverosCopyright:
Verfügbare Formate
24/4/2016
TheMDAndersonManualofMedicalOncology,2e>
Chapter36.GermCellTumors
HeatherD.BrooksLanceC.PagliaroZitaDubauskasLimLouisL.PistersNizarM.Tannir
Introduction
Germcelltumors(GCTs),themajorityarisingfromthetesticle,areahighlycurablegroupofcancers
primarilyseeninyoungmen.Thisgroupofpatientsshouldpresentaspecialconsiderationforoncologists,as
appropriatemanagementinthefrontlinesettingcanleadtomanyyearsofliferecovered,makingGCTthe
paradigmofthecurablesolidtumors.ThischapterwillprimarilydiscussGCTsarisinginthetesticle,dividing
thiscategoryintoseminomaversusnonseminomagermcelltumors(NSGCTs).Then,therareentityof
extragonadalGCTs,whichcanariseinthemediastinum,retroperitoneum,orpinealbody,willbedescribed.
OverviewofGermCellTumors
Epidemiology
GCTsarethemostcommoncancerinyoungmen.Roughly8400newcaseswerebeingdiagnosedinthe
UnitedStatesin2009,representingonlyafractionofnewgenitourinarycancerswhichareestimatedtobe
over280,000(1).Highlightingthehighcurabilityofthiscancer,GCTsonlyclaimedapproximately380lives
in2009(1)andcarrya5yearoverallsurvival(OS)rateofgreaterthan90%(2,3).GCTshaveabimodalage
distribution,withmostmendiagnosedbetweenages15and25.Thereisasecondpeakofdiagnosisaround
age60,whichlargelyrepresentsseminomahistologyandalowermortalityrisk.Lifetimeriskforthe
developmentofGCTsisapproximately0.5%or1in200(4).
Worldwide,GCTsaresixtimesmorecommonindevelopedcountries,withthelargestincidencereportedin
DenmarkandSwitzerlandandthelowestinJapan,Finland,andIsrael(4).IntheUnitedStates,theoverall
incidenceofGCTsappearstobegraduallyincreasing.TheincidencehasspecificallyincreasedamongAfrican
Americans,withthegreatestincreaseinseminomahistology.Thisdoesnotappeartoberelatedtoscreeningor
earlierdiagnosis.Caucasianmen,althoughstillrepresentingthegroupmostlikelytobediagnosed,aremore
likelytobeidentifiedatanearlierstagethaninthepast(5,6).
RiskFactors
CryptorchidismisoneofthemajoridentifiableriskfactorsforthedevelopmentofGCTs,although
representingonlyabout10%ofcases.Whenpresent,cryptorchidismimpartsarelativeriskbetween2.5and
17.1(7,8).Thisincreasedriskincludesthecontralateraltesticle,evenifdescendednormallyorviaorchiopexy.
ItisuncleariforchiopexyreducesthelifetimeriskofGCTs,althoughdatashowingincreasedincidenceeven
inthecontralateraltesticlesupportsthetheorythattheetiologyofGCTslieinabnormalgonadaldevelopment
ratherthananatomicmalposition(9,10).MenwithapriorhistoryofGCTsalsohaveanincreasedriskofGCTs
inthecontralateraltesticle,suggestingageneticpredisposition,althoughmenwithafamilyhistoryofGCTs
accountforonly1.5%ofpatientswithnewdiagnosis(11).ApersonalhistoryofGCTcarriesanincreased
lifetimeriskofsecondarycancers,irrespectiveofhistologictype(12).
1/42
24/4/2016
TumorBiology
ThemostcommongeneticabnormalityinGCTsisanisochromosomeoftheshortarmofchromosome12,
whichhasbeenidentifiedinapproximately80%ofGCT(13).Thisabnormalitycanbefoundinallhistologic
subtypes,includingintratubulargermcellneoplasia(ITGCN)(14,15).Otherchromosomalanomalieshave
alsobeenidentified.Overexpressionofckitisseeninseminoma(16).Ofnote,p53israrelyalteredinGCTs,a
factthatmayberelatedtothequalitativelydifferentresultsseenwithchemotherapyandradiationwhen
appliedtoGCTscomparedtoothersolidtumors(17).Recently,Korkolaetal.(18)identifiedagene
expressionsignaturewhichmayimprovepredictionofprognosisinGCTs.
Carcinomainsitu(CIS),orITGCN,hasbeenidentifiedastheprecursorlesioninmostGCTs.Itis
histologicallydescribedasatypicalgermcellsintheseminiferoustubules.Suchchangesarefoundadjacentto
mostinvasiveGCTs,withthenotableexceptionofspermatocyticseminoma.TheITGCNcellsexpress
numerousprotooncogenicproteinsthatplayaroleintumorigenesis,includingthereceptortyrosinekinase
CD117orckit,aproteinnormallyinvolvedingermcellmigrationandearlydifferentiation(19,20).
TumorHistology
ThemainhistologiesencounteredinGCTsareseminoma,embryonalcarcinoma,endodermalsinustumor
(EST,alsoknownasyolksactumor),choriocarcinoma,andteratoma.Thelattercanbefurtherclassifiedas
mature,immature,orteratomawithmalignanttransformation.Itisverycommontoseemorethanone
histologicsubtypewithinatumor.Importantly,theclinicalcoursecanbelargelyinferredfromthehistology.
GCTswhichshowexclusivelytheseminomahistologyconstitutepureseminomas,whilethosecontainingany
otherhistologicpatternareclassifiedasNSGCT,evenifthedominanthistologicpatternisseminoma.Thus,
thetermseminomaisusedintwoverydifferentsenses:asahistologicpatternandasamainsubdivisionof
GCT.Thebiologyandclinicalexpressionaredominatedbythenonseminomacomponent,andthusthe
presenceofanyhistologiccomponentotherthanseminomaplacesthetumorinthecategoryofNSGCT.
ClinicalPresentation
MostpatientswithGCTspresentwithpainlesstesticularswellingoranodule.Insomecases,testicular
swellingcanbeaccompaniedbypainsecondarytobleedingorinfarctionwithinthetumor.Inthepresenceof
painorahistoryofinjury,anappropriatedifferentialdiagnosiswouldincludetesticulartorsion,epididymitis,
orchitis,hydrocele,spermatocele,andhematoma.Itisextremelyimportantthatregardlessofpainorother
associatedsymptoms,allscrotalmassesshouldbeapproachedasiftheyweremalignant.Inpatientswho
presentwithgynecomastia,especiallybilateral,GCTsshouldbeconsidered(21).Othersymptomscaninclude
fever,weightloss,backpain,andhemoptysis(mostoftenseeninpatientspresentingwithhighvolume
disease).
Diagnosis
Theimportanceofearlydiagnosiscannotbestressedenoughbecausetheextentofdiseaseatpresentation
predictsoverallprognosis.IncreasedawarenessoftheoccurrenceofGCTsinyoungmenisimportantforboth
generalpractitionersandthegeneralpublic.Radiographicevaluationofasuspectedprimaryshouldinclude
highresolution,transscrotalultrasonographywithcolorDopplerofbothtesticles,andanysuspiciouslesion
shouldbedefinitivelyevaluatedwithradicalorchiectomy.
Transscrotalbiopsyiscontraindicatedinthediagnosticworkupofasuspectedtesticularneoplasm,asthis
procedurecandisruptregionallymphatics,potentiallyalteringtheotherwisepredictablenodalspread.Since
thediagnosisofGCTsisrarelyinquestion,thepreferreddiagnosticandtherapeuticprocedureforatesticular
massisradicalinguinalorchiectomy.Ifatissuediagnosisisfelttobenecessarypriortoorchiectomy,anopen
biopsyshouldbeperformedviaaninguinalincisiontoallowforproperexaminationandtissuesamplingwith
2/42
24/4/2016
minimalriskofinguinalorscrotalcontamination.
TumorMarkers
Serummarkers,specificallyhumanchorionicgonadotropin(hCG),alphafetoprotein(AFP),andlactate
dehydrogenase(LDH),haveuniquediagnosticandprognosticsignificanceinGCTs.Thesemarkersenablethe
cliniciantoinferclinicalbehavior,monitortherapy,decidewhentoapplysurgicalconsolidation,anddetect
residualorrecurrentdisease.
Elevatedinpregnancy,hCGisnotnormallydetectableinmalesexceptinthesettingofGCTs.Withahalflife
of18to36hours,hCGcanalsobemarkedlyelevatedingestationaltrophoblasticdisease,andrarely
detectableinepithelialcancers(22).Itiscomposedoftwosubunits,and,whichexistinmultipleisoforms.
Thesubunitishighlyhomologoustothesubunitofthyroidstimulatinghormone(TSH),follicle
stimulatinghormone(FSH),andluteinizinghormone(LH)whichleadsto"crosstalk"betweenthese
hormonesandhCG.Forthisreason,hCGassaysmeasurethesubunit.This"crosstalk"canbeclinically
significantinhighvolumediseaseaccompaniedbyhighlevelsofhCG,wherehCGbindstotheTSHreceptor.
Prophylacticuseofblockersisoftenneededforsymptommanagementandreliefofclinicalhyperthyroidism
(23).ExtremeelevationofhCGinmalesshouldbeconsideredpathognomonicforGCTs,and,inselectedcases
ofthreateningdisease,justifiesinitiationoftherapyevenbeforetissueconfirmation.
AFPisnormallyproducedbythefetalyolksacandalsoexistsinmultipleisoforms.ItiselevatedinGCTcells
derivedfromtheembryologicalyolksac,includingendodermalsinustumorandembryonalcarcinoma.Ithas
alsobeenfoundtobeelevatedinotherneoplasmssuchashepatocellularcarcinoma,pancreatic,gastric,and
lungcancer,andhasahalflifeofapproximately5days(24).Ingeneral,anypresenceofAFPinthesettingof
GCTsimpliesthatthehistologyisnotthatofapureseminoma(25).
LDHisexpressednormallybymultipletissuesincludingmuscle,liver,brain,andkidneyandiselevatedin
manydiseases,malignantandotherwise.Itisalsofoundinmultipleisoforms,andalthoughelevationofLDH
isanonspecificmarkerforGCTs,LDH1ismostspecificforGCTs.Todate,thereisnoestablishedroutine
useforthefractionationofLDHandprecisemeasurementofLDH1,althoughtotalLDHcanbeusedto
estimatetheprognosisasitrelatestothevolumeofdisease,ortodetectrecurrentdisease(26).
AnatomicProgression
GCTsfollowadistinctpatternofspreadandmetastasis.Thelymphaticdrainagefromthetesticlereflects
embryologicorigin,andthustherighttesticledrainstotheinteraortocavallymphnodesandthelefttesticle
drainstotheleftparaaorticlymphnodes.Theseinitialnodesofspreadaretermedthe"landingzone."
Epididymallymphaticsdrainviatheexternaliliacchainandscrotallymphaticsviathepelvicchaintherefore,
locallyadvanceddisease(involvingtheepididymisandscrotum)canpresentwithinvolvementofthesenodal
basins.Distantmetastasisinvolvesthelungsprincipally,followedbytheliver,brain,andbones.
Staging
Table361showsthemostrecentAmericanJointCommissiononCancer(AJCC)TNMstagingoftesticular
cancer(27).Thissystemisbasedontheanatomiccharacteristicsofthetumor,thepresenceofelevatedtumor
markers,andthepresenceofdistantdisease.Thesewelldefinedriskfactorsareusedtoplacepatientsinrisk
stratificationgroups.Ingeneral,stageIdiseaseisconfinedtothetestes,stageIIdiseaseisconfinedtothe
retroperitoneumwithmarkersinthegoodprognosisrange,andstageIIIdiseaseincludesnodesthatextend
beyondtheretroperitoneum,extranodalmetastases,andelevationoftumormarkerstotheintermediateor
poorprognosisrange.
Table361.GermCellTumor:TheNewAJCCTNMStagingofTesticularCancer
3/42
24/4/2016
PRIMARYTUMOR(T)
Theextentofprimarytumorisusuallyclassifiedafterradicalorchiectomy,andforthisreasonapathologic
stageisassigned.
pTXPrimarytumorcannotbeassessed
pT0Noevidenceofprimarytumor(eg,histologicscarintestis)
pTisIntratubulargermcellneoplasia(carcinomainsitu)
pT1Tumorlimitedtothetestisandepididymiswithoutvascular/lymphaticinvasiontumormayinvadeinto
thetunicaalbugineabutnotthetunicavaginalis
pT2Tumorlimitedtothetestisandepididymiswithvascular/lymphaticinvasion,ortumorextendingthrough
thetunicaalbugineawithinvolvementofthetunicavaginalis
pT3Tumorinvadesthespermaticcordwithorwithoutvascular/lymphaticinvasion
pT4Tumorinvadesthescrotumwithorwithoutvascular/lymphaticinvasion
REGIONALLYMPHNODES(N)CLINICAL
NXRegionallymphnodescannotbeassessed
N0Noregionallymphnodemetastasis
N1Metastasiswithalymphnodemass2cmingreatestdimensionormultiplelymphnodes,none>2cmin
greatestdimension
N2Metastasiswithalymphnodemass>2cmbutnot>5cmingreatestdimensionormultiplelymphnodes,
anyonemass>2cmbutnot>5cmingreatestdimension
N3Metastasiswithalymphnodemass>5cmingreatestdimension
PATHOLOGIC(PN)
pNXRegionallymphnodescannotbeassessed
pN0Noregionallymphnodemetastasis
pN1Metastasiswithalymphnodemass2cmingreatestdimensionand5nodespositive,none>2cmin
greatestdimension
pN2Metastasiswithalymphnodemass>2cmbutnot>5cmingreatestdimensionor>5nodespositive,
none>5cmorevidenceofextranodalextensionoftumor
pN3Metastasiswithalymphnodemass>5cmingreatestdimension
DISTANTMETASTASIS(M)
M0Nodistantmetastasis
M1Distantmetastasis
M1aNonregionalnodalorpulmonarymetastasis
M1bDistantmetastasisotherthantononregionallymphnodesandlungs
SERUMTUMORMARKERS(S)
SXMarkerstudiesnotavailableornotperformed
S0Markerstudylevelswithinnormallimits
S1LDH<1.5NAND
hCG(mIU/mL)<5000AND
AFP(ng/mL)<1000
S2LDH>1.510NOR
hCG(mIU/mL)500050,000OR
AFP(ng/mL)100010,000
S3LDH>10NOR
4/42
24/4/2016
hCG(mIU/mL)>50,000OR
AFP(ng/mL>10,000
NindicatestheupperlimitofnormalfortheLDHassay.
StageGrouping
Stage0
pTis
StageI
pT14
StageIA
pT1
StageIB
pT2
pT3
pT4
StageIS
AnypT/Tx
StageII
AnypT/Tx
StageIIA
AnypT/Tx
AnypT/Tx
StageIIB
AnypT/Tx
AnypT/Tx
StageIIC
AnypT/Tx
AnypT/Tx
StageIII
AnypT/Tx
StageIIIA
AnypT/Tx
AnypT/Tx
StageIIIB
AnypT/Tx
AnypT/Tx
StageIIIC
AnypT/Tx
AnypT/Tx
AnypT/Tx
N0
N0
N0
N0
N0
N0
N0
N13
N1
N1
N2
N2
N3
N3
AnyN
AnyN
AnyN
N13
AnyN
N13
AnyN
AnyN
M0
M0
M0
M0
M0
M0
M0
M0
M0
M0
M0
M0
M0
M0
M1
M1a
M1a
M0
M1a
M0
M1a
M1b
S0
SX
S0
S0
S0
S0
S13
SX
S0
S1
S0
S1
S0
S1
SX
S0
S1
S2
S2
S3
S3
AnyS
Reproduced,withpermission,fromEdgeSB,ByrdDR,ComptonCC,eds.AJCCCancerStagingManual,7th
edition.NewYork,Springer,2010,pp.47577.
ConsiderationofFertilityPreservation
OfparticularimportanceinGCTsisthepreservationoffertility.BoththediagnosisandtreatmentofGCTscan
affectfertilitynegatively,potentiallydecreasingaman'sabilitytoconceiveindefinitely.Itisrecommended
that,ifclinicallyfeasible,thepatientbecounseledaboutandofferedtheopportunitytopursuespermbanking
beforestartingchemotherapy.Itisnotrecommendedtodelaychemotherapyinsymptomaticpoorriskpatients,
aspoorphysicalconditionoftenmakesspermdonationdifficultorevenimpossible(28).
TesticularSeminoma
Histology
Undermicroscopicvisualization,classicseminomahasa"friedegg"appearancedefinedasamonotonous
proliferationoflarge,roundedcellsarrangedinsheetsorcordswithlargecentralizednucleiandnucleoli.
Thesetumorscanbedifficulttodistinguishfromlymphomaifthereisabackgroundoflymphocytic
5/42
24/4/2016
infiltration.Furtherconfirmation(ie,negativityforlymphocytemarkerssuchascommonleukocyteantigen)is
oftenrequired.Althoughnotspecific,seminomasstainpositiveforplacentalalkalinephosphatase(PLAP)and
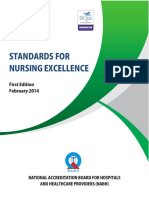
areroutinelynegativeforAFPandhCG.Figure361showsthehistologicalappearanceofclassicseminoma.
Figure361.
Histologicalappearanceofclassicseminoma.
Onpathologicexaminationofthetestis,seminomatendstobeasemisolidtumorthatreadilyoozesontothe
grossexaminationtable.Thismakesthepresenceofmalignantcellsonthesurfaceofthespermaticcordandat
themarginsofresectionaubiquitousfinding.Thus,theclinicianmustbecarefulnottobeundulyinfluenced
byreportsof"marginpositivity"and"involvementofthespermaticcord"inthepathologyreport(29).Figure
362showsthetypicalgrossappearanceofseminoma.
Figure362.
6/42
24/4/2016
Grossappearanceofseminoma.
Eveninthepresenceofsignificantmetastaticdisease,itisnotuncommontofindonlyascarinthetesticle.
Thisphenomenonisknownas"burnedout"seminomaandisnotaprominentfeatureofNSGCTs,except
choriocarcinoma.Thebiologicalbasisforthisspontaneousregressionoftheprimaryisnotknown.Seminomas
aretypicallyassociatedwithasignificantinflammatoryinfiltration,andtheycharacteristicallyleaveadense
desmoplasticresidualmassaftertreatmentoftenmakingthemdifficulttoresect.
ClinicalFeatures
PureseminomaisthemostcommonGCTofthetesticle,accountingforapproximately50%ofGCTs.By
definition,seminomashavenoevidenceofanonseminomacomponentanddonotproduceAFP,butmayhave
modestelevationofhCG.Spermatocyticseminomas,ararevariantcomprisingonly10%ofseminomas,are
notassociatedwithITGCN.Thesetumorstypicallyoccurinmenover50yearsold,instageIdisease,and
havealowmetastaticrate.Thissubtypeportendsanexcellentprognosiswithresectionalone(radiotherapy)
(30).Seminomastendtospreadvialymphaticsinitially,withlatehematogenousspread,andaremorelikelyto
spreadlocally,asevidencedbypositivemarginsandinvolvementofthespermaticcordonhistology.Themost
commonhematogenousspreadistothelungs,andmetastaticseminomasrarelymetastasizetothebrain.
Remarkably,verybulkytumorsrapidlyrespond,withdramaticlossoftumorbulk,buttumorlysissyndromeis
neverencountered.
Prognosis
TheInternationalGermCellCancerCollaborativeGroup(IGCCCG)establishedastandardriskclassification
forbothseminomasandNSGCTs.Patientswithseminomaaredividedintoeithergoodorintermediaterisk
categories,withnodefinablepoorriskcategory.Theonecharacteristicthatpredictedpatientprognosiswas
thepresenceorabsenceofnonpulmonaryvisceralmetastases.Interestingly,prechemotherapytumormarkers
didnotinfluenceprognosis(unlikeinNSGCTstobediscussedlater).Theprognosticcategoriesfromthis
7/42
24/4/2016
researchareoutlinedinTable362.Ninetypercentofpatientswithseminomafellintothegoodprognosis
categoryandhad5yearOSof86%.Patientswithseminomaintheintermediateprognosiscategoryhada5
yearOSof72%(2).
Table362.IGCCCGClassificationPrognosticRiskStratification(2)
Seminoma
Nonseminoma
GOODRISK
Anyprimarysite
Testis/retroperitonealprimary
and
and
Nononpulmonaryvisceral Nononpulmonaryvisceral
metastases
metastases
and
and
NormalAFP,anyhCG,
AFP<1000ng/mL
anyLDH
hCG<5000mIU/mL
LDH<1.5ULN
82%5yearPFS86% 86%5yearPFS90%
5yearOS
5yearOS
INTERMEDIATERISK
Anyprimarysite
Testis/retroperitonealprimary
and
and
Nonpulmonaryvisceral
Nononpulmonaryvisceral
metastases
metastases
and
and
NormalAFP,anyhCG,
AFP100010,000ng/mL
anyLDH
hCG500050,000mIU/mL
LDH1.510ULN
67%5yearPFS72% 75%5yearPFS80%
5yearOS
5yearOS
POORRISK
Mediastinalprimary
or
Nonpulmonaryvisceral
metastases
or
AFP>10,000ng/mL
hCG>50,000mIU/mL
LDH>10ULN
41%5yearPFS48%
5yearOS
ManagementofClinicalStageISeminoma
ClinicalstageIseminomapatients,representing70%ofpatientsatdiagnosis,generallyhavediseaseconfined
tothetesticlewithnoevidenceofnodalordistantmetastasis.Mostpatientswillbecuredbyradical
orchiectomyalone,butbetween12and32%willrecurwithoutfurthertreatment.Definingthepatientswho
8/42
24/4/2016
areathighriskforrecurrentdiseasecouldavoidunnecessaryinterventionandexposuretotreatmentrisks.
ActiveSurveillance
Withthemajorityofpatientscuredpostsurgery,activesurveillanceremainsareasonableoptionforthe
motivatedandreliablepatient.Thebenefitsofsurveillanceincludeavoidanceofunnecessarytreatmentand
riskinpatientswhocanhavediseasecontrolregainedatthefirstsignofrecurrence.Wardeetal.reporteddata
on638patientsmanagedwithsurveillancewithamedianfollowupof7years.Patientswithaprimarytumor
lessthan4cmandwithoutinvasionofretetestishad5yearriskofrelapseof12%.Patientswithbothrisk
factorshadriskofrecurrenceof32%,whileoneofthetworiskfactorsportendsa16%riskofrelapse(31).
Becauseofexcellentoutcomesofpatientslatertreatedforrecurrentdisease,activesurveillanceisstill
consideredareasonableoptioninpatientswithbothriskfactors.
Radiotherapy
Deliveryof20GytotheparaaorticsaloneisastandardmanagementstrategyforclinicalstageIseminoma.
Theradiationfieldtotheparaaorticsisdefinedasa10cmwidefieldbetweenT12andL5.Thiscurrent
standardisbasedondatafromtwotrials.Thefirst,byJonesetal.,randomlyassignedpatientstoeither20Gy
in10fractionsover2weeksor30Gyin15fractionsover3weeks.Patientsreceivingthe30Gydosereported
moresymptomsat4weeks(nodifferenceat12weeks),withnoevidencefordecreasedrelapserateatmedian
followupof61months(32).Fossaetal.reportedtheirexperiencewith478patientswithstageIdisease
randomlyassignedtoreceiveradiationtoboththeparaaorticandipsilateraliliacfieldsversustheparaaortic
fieldalone.Thosetreatedwithreducedfieldshad3yearsurvivalof99.3%versus100%withtheextended
field.Thisminimallossoftreatmentefficacywasaccompaniedbyareductioninbothgastrointestinalside
effectsandinfertilityrisk.Adeterminationoftheriskofsecondarymalignancieswasnotyetassessable,butit
ispresumedtobereducedinthefaceofthedecreasedsizeofradiationportals(33).
Chemotherapy
Recently,datahavebeenreportedfromarandomizedcomparisonofsingleagentcarboplatindosebasedon
AUC7versusradiotherapyfortheadjuvanttreatmentofclinicalstageIseminoma(34).Medianfollowup
was4years,andtherelapsefreesurvivalwassimilarinbothgroups,96.7%and97.7%,respectively,showing
noninferiorityoftheonecycle,singleagentcarboplatinstrategy.Thistreatmentapproachisavaluableoption
forpatientswhocannottolerateorhavecontraindicationstoradiationtherapy.Therearenodatacurrently
comparingthelongtermsafetyofthisstrategyorsufficientevidencetocommentonanyriskofsecondary
malignancy.Figure363outlinesourapproachtotherapyforstageIseminoma.
Figure363.
9/42
24/4/2016
Managementoftesticularcancer(seminoma).
ManagementofNonbulky,GoodRiskSeminoma(StagesIIA/IIB)
PatientswithstageIIseminomaareoftendividedintononbulkyversusbulkydiseasefortreatmentdiscussion.
Ingeneral,nonbulkydiseaseisdefinedasnodeslessthan5cmintheCTorMRI.Theprimarymodeof
therapyforpatientsinthiscategoryisradiotherapyunlessthepatienthascontraindicationorisunableto
tolerateradiationtreatment.
Radiotherapy
ItisnolongerrecommendedthatstagesIIAandIIBseminomapatientsreceivehighdoseradiation(3035
Gy),mediastinalradiation,orleftsupraclavicularradiation.Thecurrentrecommendationisforradiotherapyto
adoseof20Gytotheparaaorticandipsilateraliliacnodalfieldswitha6Gyboosttotheparaaorticlymph
nodes(35).Occasionally,radiographicevidenceforresidualdiseaseispresentpostradiotherapy,butifthe
abnormalityislessthan3cm,observationisrecommended.
AlternativestoRadiotherapy
Thereisasubsetofpatientswhowillnotbeabletoreceiveradiationtherapyforvariousreasons.These
reasonsmayincludepatientrefusal,inflammatoryboweldisease,horseshoeorpelvickidney,andhistoryof
abdominalsurgery.Inthissetting,systemicchemotherapycouldbeoffered.InaseriespublishedbyXiaoetal.
(36),goodprognosisseminomapatientswereincludedintheanalysisandweretreatedwithfourcyclesof
etoposideandcisplatin(EP).AlthoughthisdoesnotrepresentthestandardofcareforstagesIIAandIIB
seminoma,itisareasonablealternativeforpatientswhoabsolutelycannotreceiveradiationtherapy.
ManagementofAdvanced,GoodRiskSeminoma(StagesIIC/III)
ThistreatmentgroupincludesstageIIpatientswithbulkylymphadenopathy(>5cm)andstageIIIpatients
withgoodriskdisease.Inthisgroupofpatients,theriskofrecurrenceremainshighdespitelocaltherapyand
10/42
24/4/2016
thereforetheprimarytreatmentrecommendationissystemicchemotherapy.Itisalsointhiscategoryof
patientsthattheroleofpositronemissiontomography(PET)scanmaybeintroducedinitslimitedrolefor
GCTs.
Chemotherapy
Therecommendedsystemicchemotherapyregimenforpatientswithgoodriskadvancedseminoma(stages
IICorIIIA)isthreecyclesofbleomycin,etoposide,andcisplatin(BEP).Theevidenceforuseofthreecycles
ofBEPversusfourcycleswaspresentedbydeWitetal.(37,38).Theseinvestigatorsshowedthatthreecycles
ofBEPisequivalenttofourcycles,with2yearprogressionfreesurvival(PFS)of90.4%and89.4%,
respectively(39).Alternatively,patientswhoareunableorrefusetoreceivebleomycinorareolderthan50
yearscanbesuccessfullytreatedwithfourcyclesofEP.
ResidualDiseaseafterChemotherapyandtheRoleofPET
Aftercompletionofchemotherapy,restagingCTscansareperformed.Ifapatientisfoundtohavenoresidual
diseaseorresidualdiseasemeasuringlessthan3cminsizewithnormaltumormarkers,activesurveillance
shouldbepursued.Postchemotherapy,residualdiseasemeasuringgreaterthan3cmcanbefurtherevaluated
byPETimaging.EvidencefortheroleofPETimaginginthesettingofresidualdiseasegreaterthan3cmwas
presentedbyDeSantisetal.(40).Inthisevaluationof33patientswithfollowuptimeof23months,the
positivepredictivevalueofFDGPETwas100%,withaspecificityandsensitivityof100%and89%,
respectively,fortheidentificationofresidualdiseaseinlesionsmorethan3cm.Althoughencouraging,the
roleofPETimaginginthissettingisbeingreexamined,becauseseveralfalsepositivecasesfromour
institutionhavebeenrecentlyidentified.
PETNegativeDiseasePostchemotherapy
IfthereisnoevidenceofaviduptakeonPET,thepatiententerstheactivesurveillancestrategy.Ifthepatientis
unabletohavePETimaging,surgicalbiopsyorconsolidativeradiationtherapycanbeconsideredforthose
patientswithresidualdiseasemeasuringgreaterthan3cm.
PETPositiveDiseasePostchemotherapy
AtMDAnderson,apositivePETscanrequiresaconfirmatorybiopsy.Ifresidualdiseaseisconfirmed,several
optionscanbeconsidered.First,salvageradiationtherapytotheresidualmasscanbeoffered,butthisdoesnot
providelongtermcontrol.Second,thepatientcanbeofferedsalvagechemotherapy.Finally,thepatientmay
undergohighdosechemotherapywithautologousstemcelltransplantation.SeeFigure363forthealgorithm
ofourmanagementstrategy.
ManagementofAdvanced,IntermediateRiskSeminoma
Patientswithadvanced,intermediateriskseminomahavenonpulmonaryvisceralmetastasis.Themost
commonsitesofdiseasearetheliverandbone.Theserarepatientsareofferedsystemicchemotherapyupon
presentation(seeFigure363).ThechemotherapyregimenscommonlyusedarefourcyclesofBEP,four
cyclesofetoposide,ifosfamide,cisplatin(VIP),orfourcyclesofpaclitaxel,ifosfamide,cisplatin(TIP)(41).
SalvageTherapyforRefractory/RecurrentSeminoma
Theprimarytreatmentofrecurrentseminomaissalvagechemotherapy.Forpatientswithlungmetastasis
(goodriskcategory),thestandardofcareisadministrationofeitherthreecyclesofBEPorfourcyclesofEP.
Inpatientswithboneorlivermetastasis(intermediateriskcategory),salvagechemotherapyispursuedwith
11/42
24/4/2016
eitherfourcyclesofBEP,TIP,orVIP.Bleomycinshouldbeavoidedinmenolderthan50years.
Clinicalsignsofrefractorydiseaseshouldbeapproachedwithanaggressivechangeofstrategy,includingthe
optionofhighdosechemotherapyandstemcelltransplantation.UsuallyreservedforBEPfailuresand
recurrentdisease,theroleofstemcelltransplantationinrefractory/recurrentadvancedseminomawas
addressedbyEinhornetal.(42).Nineteenpercentofaseriesof184patientswerepatientswithmetastatic
testicularseminoma.Atamedianfollowupof48months,26of35seminomapatientstreatedwerein
completeremission.Patientsinthiscategoryshouldbeconsideredforreferraltotransplantcentersifpossible.
Case361:SeminomaPresentingwithRenalInsufficiency
A37yearoldmanhadaleftinguinalorchiectomyforclassicseminoma.Laboratorydataatpresentationto
MDACCrevealedserumcreatinineof1.8mg/dL,calcium12.7mg/dL,Hgb10.5g/dL,hCG113mIU/mL,Alk
phos194IU/L,andLDH1773IU/L(ULN618).ACTscanofabdomenandpelvisrevealedalarge
retroperitonealmasswithmarkedlefthydronephrosis(Fig364A).Thepatientreceivedinitiallyonecycleof
cyclophosphamideandcarboplatinum.Repeatlaboratorydatarevealedserumcreatinineof1.1mg/dL,calcium
8.2mg/dL,LDH483IU/L,andundetectablehCG.HesubsequentlyreceivedthreefullcyclesofEPwith
excellentresponse.RepeatimagingshowninFig364Brevealedmarkedimprovementinthesizeofthemass
(from147cm).PostchemotherapyPETimagingshowedtheresidualmasstobemetabolicallyinactive.
Figure364A.
12/42
24/4/2016
Baselineimagingfromcase361showingalargeleftretroperitonealmasswithlefthydronephosis.
Figure364B.
13/42
24/4/2016
14/42
24/4/2016
Repeatimagingfrompatientincase361showingmarkedimprovementinmassafter3cyclesof
chemotherapy.
Comment:Apatientwithadvancedseminomapresentingwithhydronephrosisandrenalinsufficiencymay
receiveinductionchemotherapywithcyclophosphamideandcarboplatinumratherthanplacingnephrostomy
tubestoallowadministrationofBEPorEPinthefirstcycle.Thepatientcansubsequentlyreceivestandard
therapyafternormalizationofrenalfunction.
NonseminomatousGermCellTumors
Histology
EmbryonalCarcinoma
EmbryonalcarcinomaisthesecondmostcommonpurepresentationofGCT.Itisrarelyseenattheextremes
ofage,mostcommonlypresentinginthe20to30yearagegroupandpresentswithmetastasisinonethirdof
cases.Microscopically,embryonalcarcinomacellsarethemostundifferentiatedoftheGCTtypesandare
characterizedbymicroscopicallyvariedcellswithindistinctbordersandscantcytoplasm,givingthe
appearanceofoverlappingnuclei.Tumorcellscanbeseeninsheetsorarrangedaspapillaryortubular
structureswithahighmitoticrate.Thereisapropensityforvascularinvasion.Phenotypiccharacterizationcan
revealpositivityforcytokeratin,CD30,PLAP,AFP,andhCG.ModestelevationsofbothAFPandhCGare
typical,butimportantly,pureembryonalcancerscanbemarkernegativeintheserum.Figure365showsthe
typicalhistologicappearanceofembryonalcarcinoma.
15/42
24/4/2016
Figure365.
Histologicalappearanceofembryonalcarcinoma.
EndodermalSinusTumors(orYolkSacTumors)
PureyolksactumorsareextremelyrareintheadultpatientbutaccountforthemajorityofchildhoodGCTs.In
adults,endodermalsinustumor(EST)oryolksacelementsarecommonlyseenasacomponentofmixed
NSGCTs.Microscopically,ESTcanmanifestasmacrocystic,papillary,solid,oraglandular/alveolarpattern
withperivasculararrangementsofepithelialcellsknownasglomeruloidorSchillerDuvalbodies.HighAFP
levelsgenerallyreflectanESTcomponent,andserumlevelsofAFPareimportantprognosticallyinthe
classificationofgood,intermediate,andpoorriskmetastaticNSGCTs.Figure366showsthetypical
histologicalappearanceofanESTcarcinoma.
Figure366.
16/42
24/4/2016
HistologicalappearanceofESTcarcinoma.
Choriocarcinoma
Alsorareinthepureformintheadultpopulation,choriocarcinomafrequentlypresentsasacomponentof
NSGCTs.Choriocarcinomascomprisebothsyncytiotrophoblastsandcytotrophoblasts,typicallyarrangedin
sheetsornests.ChoriocarcinomasgenerallymakecopiousamountsofhCG,andthelevelofthismarkerisalso
anindicationofprognosisinmetastaticNSGCTs.HalfofchoriocarcinomasarePLAPpositive.
Choriocarcinomaelementstendtodominatetheclinicalcourseandfrequentlymetastasizetothebrain.Figure
367showsthetypicalhistologicalappearanceofchoriocarcinoma.
Figure367.
17/42
24/4/2016
Histologicalappearanceofchoriocarcinoma.
Teratoma
Teratomaspossesssomaticcellsfromatleasttwogermcelllayers(ectoderm,endoderm,andmesoderm).
Variabledegreesofdifferentiationallowforthesubclassificationofmatureandimmatureforms.Mature
teratomaconsistsofterminallydifferentiatedtissuesandcanformcysticstructures.Althoughhistologically
bland,thislowgrademalignancycangrowtoathreateningdimensionandbecomeunresectable.Onlyabout2
to3%ofallGCTsshowmatureteratomaastheonlyhistologiccomponent,butteratomaiscommonlypresent
asanelementofamixedGCT.Immatureteratomaislessdifferentiatedanddisplaysacorrespondinglymore
aggressivebiology.OneoftheunfortunatemanifestationsisthedevelopmentofnonGCTwithintheteratoma.
Knownasteratomawithmalignanttransformation,thisentitytypicallydisplaysthebiologyofwhatever
histologydevelopsandcanrangefromleukemiastosarcomastocarcinomas.Ingeneral,suchatransformation
beliesapoorprognosis(43).Figures368and369representthetypicalhistologicalandgrossappearanceof
teratoma,respectively.
Figure368.
18/42
24/4/2016
Histologicalappearanceofteratoma.
Figure369.
Grossappearanceofteratoma.
ClinicalFeatures
Asdescribedpreviously,approximatelyhalfoftesticularGCTsshowhistologicelementsotherthanseminoma
orproduceserumelevationofAFPindicatingnonseminoma.Thesecancersarecollectivelyknownasmixed
GCTsorNSGCTs,andtheyformagroupofhistologicallyandclinicallydiversecancers(44).NSGCTsare
morelikelytospreadhematogenouslywithincreasedriskofdistantmetastasiswhencomparedtoseminomas.
19/42
24/4/2016
BecauseoftheuniqueandheterogeneousnatureofNSGCTs,thereareseveralclinicalpresentationswhich
warrantfurtherdiscussion,becauseoftheirsignificancetopatientcareandprognosis.
GrowingTeratomaSyndrome
Residualteratomaisalowgrade,slowgrowingmalignancythatcanbefatalbyinexorablegrowth.Thiscan
take10oreven20yearstobecomethreateningandthuscanbemissedwithoutdedicatedlifelongfollowupof
patientswithNSGCTs.Oneofthemostremarkableandclinicallyimportantfeaturesofteratomasisthatthey
areoften"pushing,"andrarelyinvasive.Thusatsurgery,evenverylargemassesaresometimesremovedfar
moreeasilythanwouldbeexpectedonthebasisofthepreoperativeimaging.Itisimportanttoconsultacenter
wheresufficientsurgicalexperienceisavailablebeforeconcludingthataresidualteratomais"unresectable"
(45).
ChoriocarcinomaSyndrome
Asthenameimplies,thisisseeninthesettingofhighvolumeNSGCTthatshowspredominantly
choriocarcinomahistologyandisassociatedwithveryhigh(typicallyabout1,000,000U/L)levelsofhCG.
Thissyndromeischaracterizedbyprominentconstitutionalsymptomsthatrepresenttheeffectsofbothabulky
cancer,andsecondaryhyperthyroidismcausedbycrossreactionofhCGwithTSHreceptors.Typically,
patientsarerapidlylosingweight,tachycardic,anxious,diaphoretic,andhavetender,swollenbreastsfrom
secondaryhyperprolactinemia.Inaddition,mostpatientshavehighvolumelungmetastaseswithimpending
respiratorycompromisefromtheburdenofpulmonarymetastasis.Thisisamedicalemergency,andtreatment
shouldnotbedelayedforhistologicconfirmation,sincethisisapathognomonicconstellationinayoungman.
Metastaticchoriocarcinomahasapropensityforbrainmetastasis,althoughtheyarenotalwaysapparenton
baselineimaging.
Prognosis
Asdescribedabovewithseminoma,theIGCCCGdevelopedaprognosticstagingsystemforNSGCTswith
nonpulmonaryvisceralmetastasisfoundasamajorfactorinprognosis.Unlikeseminoma,prechemotherapy
tumormarkerswereidentifiedassignificantintheprognosisofthesepatients.Theprognosticcategoriesare
outlinedinTable362.Ingeneral,patientswithmediastinalprimary,nonpulmonaryvisceralmetastasisand
"poormarkers"asdefinedinthefigureareconsideredtohavepoorprognosisandhavea5yearOSof48%.
Patientswithtestisorretroperitonealprimary,nononpulmonaryvisceralmetastasisareplacedinthegood
prognosiscategorybasedontumormarkerlevelsasdescribedinthefigure.Goodprognosispatientshavea5
yearOSof92%.Allothersareplacedintheintermediateriskgroupandhavea5yearOSof80%(2).Van
Dijketal.(3)updatedthe5yearOSdataforNSGCTsinapooledmetaanalysis.Theauthorsreported5year
OSof94%forgoodprognosis,83%forintermediateprognosis,and71%forpoorprognosis.Thisillustrates
theimprovingsurvivalratesinthehighriskgroup.
ManagementofClinicalStageINSGCT
Ingeneral,clinicalstageINSGCTincludespatientswithnormalmarkerspostorchiectomyandnoevidenceof
diseaseoutsidetheresectedtestis,epididymis,orcord.Aswithseminoma,radicalinguinalorchiectomyisthe
initialtherapyforearlystageNSGCT.Appropriatesurgerywillcureapproximately70%ofclinicalstageI
patients.Thetwoidentifiedriskfactorsinthesepatientsincludepercentageofembryonalhistologyand
lymphovascularinvasion(LVI),withLVIthemostpredictive(46).Patientsareconsideredlowriskfor
recurrencepostorchiectomy,ifthereislessthan50%embryonalcomponentinthetumorandnoevidenceof
LVI.Theroleofpercentageofembryonalcomponentisdebatable.Infact,Europeanguidelinesutilizeonly
absenceofLVIfordeterminationof"lowrisk"forrecommendationofobservation(47).
Observation
20/42
24/4/2016
Observationisareasonablestrategyforthereliable,lowriskpatient,whichinpracticecanbethosewith
absenceofLVI.TheactivesurveillancescheduleasoutlinedbytheNationalComprehensiveCancerNetwork
(NCCN)ClinicalPracticeGuidelinesinOncologyrecommendsthatpatientsshouldhaveaphysical
examination,chestradiography,andtumormarkermeasurementseverymonthduringthefirstyear,every2
monthsduringthesecondyear,andeverythirdmonthduringthethirdyear.AbdominalandpelvicCTis
recommendedapproximatelyevery3monthsduringthefirstyearandevery4monthsforyears2and3(48).
RetroperitonealLymphNodeDissection
Retroperitoneallymphnodedissection(RPLND)isasurgicalremovalofthe"landingzone"lymphnodes.An
accuratestagingstrategy,itsroleinprimarypreventionofrecurrenceinstageINSGCTpatientsis
controversial.MorbidityofRPLNDincludessympatheticnervedamagethatmayleadtofailureofejaculation
andinfertilityhowever,useofamodifiedsurgicaltemplateisanervesparingapproachthatcanpreservethe
sympatheticnervesandmayfacilitateantegradeejaculationin90%ormorepatients.Stephensonetal.(49)
reportedthatRPLNDinclinicalstageIpatientsyieldeda4yearprogressionfreeprobabilityof96%andisan
optionfortherapyinthispatientpopulation.Higherfailurerateshavebeenreportedforpatientswithhighrisk
clinicalstageINSGCT.PatientswhodonotundergoprophylacticRPLNDmustundergoperiodicCT
scanningoftheabdomentoruleoutgrowingteratomaintheretroperitoneum.
Chemotherapy
Inthepast,adjuvantchemotherapyforstageINSGCTpatientswithhighriskofrecurrenceconsistedoftwo
cyclesofBEP.Recently,tworandomizedtrialsevaluatedtheimpactofonecycleofBEP.Albersetal.(50)
comparedRPLNDtoonecycleofBEPin382patientswithamedianfollowupof4.7years.The2year
recurrencefreesurvivalwas99.46%inthechemotherapygroupand91.87%intheRPLNDgroup,suggesting
anadvantageofonecycleofBEPchemotherapy,althoughthisfindingdidnotreachstatisticalsignificance.
Tandstadetal.(51),intheSWENOTECAstudy,confirmedthesefindingsin745patientswhowere
prospectivelyrandomizedbasedonthepresenceofLVI.TheseinvestigatorsreportedthatonecycleofBEP
reducedtheriskofrecurrenceby90%inpatientswithorwithoutLVI.Ouralgorithmformanagementofnon
seminomatesticularcancerisshowninFigure3610.
Figure3610.
21/42
24/4/2016
Managementoftesticularcancer(nonseminoma).
ManagementofGoodRiskClinicalStagesIIAandIIBNSGCT
Patientswithtumormarkernegative,stagesIIAorIIBNSGCTspresentauniqueclinicalsituation.Atour
institution,thesepatientsaredividedintogroupsbyCTevidenceofdiseasegreaterthanorlessthan3cm.If
patientshavenegativetumormarkerswitharetroperitonealmasslessthan3cmafterorchiectomy,surgical
biopsyispursued.Ifnegative,thenobservationisareasonablealternativeforthereliablepatient.Patientswith
largerthan3cmdisease,positivetumormarkers,orpositivebiopsyaretreatedwithprimarychemotherapy
withBEPforthreecycles.Asdiscussed,severalgroupshavereportedlongtermfollowupdataconfirmingthe
equivalenceofthreecycleswhencomparedtofourcyclesofBEP(37,38).Aspreviouslyrecommended,four
cyclesofEPisalsoareasonablealternativeinpatientswhorefuseorhaveacontraindicationtoreceive
bleomycin(39).Ifresidualtumorisdetectedonfollowupstaging,surgicalresectionisrecommended.
ManagementofGoodRiskStagesIICandIIINSGCT
Patientswithbulkyretroperitonealdiseaseofgreaterthan5cmorpulmonarymetastasis,withrelativelylow
serummarkersconstitutethosewithadvanceddisease,butstillwithfavorableprognosis.Thesepatientsmay
beeitherstageIICorIIIAaccordingtotheAJCCcriteriaandareconsideredtogetherinthisdiscussion.The
primarymodeoftreatmentinthispatientpopulationissystemicchemotherapy.Thismaybeadministered
beforeorafterradicalorchiectomyaslongassurgicalresectionoftheprimaryisperformedaftercompletion
oftherapy.Onceagain,threecyclesofBEPchemotherapyisconsideredstandardofcareandfourcyclesofEP
consideredareasonablealternativeforpatientswithacontraindicationtoreceivebleomycin.Resectionof
residualdiseasepresentonrestagingshouldbeperformed(3739).
Pathologyoftheresectedtumoraftersalvagechemotherapyisdifferentthanafterprimarychemotherapy.
Followingprimarychemotherapy,viableGCT,fibrosis,orteratomaarefoundinapproximately20%,40%,
and40%ofpathologicalspecimens,respectively,comparedto50%,10%,and40%followingsalvage
chemotherapy,respectively.Patientswithgreaterthan10%viableGCTintheresidualpathologyspecimen
afterprimarychemotherapyshouldreceiveadditionaltwocyclesofplatinumbasedchemotherapy(Figure36
10).
22/42
24/4/2016
ManagementofIntermediateandPoorRiskAdvancedStagesIIIBandIIICNSGCT
PatientswithadvancedNSGCTswhopresentwithintermediateorpoorriskfeaturesaremanagedwith
systemicchemotherapyconsistingoffourcyclesofBEP.Thismaybegivenpriortoradicalorchiectomy.For
advanced,intermediateorpoorriskpatientswithacontraindicationtoreceivebleomycin,VIP,orTIPis
recommended(52).Thesepatientsshouldalsobeconsideredforparticipationinclinicaltrials.
ManagementofRecurrentandRefractoryNSGCT
Severalchemotherapyregimenswithclinicalactivityinthesalvagesettinghavebeenreported,andthese
includeVIP,TIP,VeIP(vinblastine,ifosfamide,cisplatin),IPO(irinotecan,paclitaxel,oxaliplatin),or
gemcitabine/oxaliplatin.Ingeneral,manypatientsrespondandsomeareevencuredwithsalvage
chemotherapyandsurgicalconsolidation,especiallythosewithasmallormoderatevolumeofdisease.There
hasbeensomesuggestionthatrotationofchemotherapyregimensmayoffersomebenefit.Wearecurrently
evaluatingourownexperiencewiththistreatmentstrategy.
Thestrategymostsupportedbyrecentdataistheroleofhighdoseinductionchemotherapywithstemcell
transplantation.Einhornetal.(42)retrospectivelyreviewed184patients(149patientswithadvancedNSGCT)
withamedianfollowupof48months.Ninetyofthe149patientswithNSGCTtreatedwithhighdose
chemotherapyandsubsequentautologousstemcelltransplantationwerediseasefreeatfollowup.Theauthors
suggestthatuseofthisaggressivetreatmentassecondlinetherapyisdistinctlyadvantageouswhencompared
topatientswhoreceivethistreatmentinthethirdlinesetting.Basedonthisstudyanddespitetheabsenceofa
randomizedtrial,patientswithrecurrentorrefractoryadvancedstageNSGCTmaybeconsideredforthis
aggressive,yeteffective,treatmentstrategy.
SpecialConsiderations
PitfallsinTumorMarkerElevation
MildelevationofhCG(usually<20)mayoccursecondarytohypogonadismormarijuanause,andtherefore,
shouldnotalwaysbeattributedtoresidualorrecurrenttumor.ModestelevationofAFPmaybepresentwith
residualteratomaandwillnormalizefollowingsurgicalresection,butmayalsobeconstitutionallyelevatedor
indicatepresenceofliverdisease.Additionally,elevatedtumormarkersmayindicateunidentifiedCNSdisease
orresidualprimarytesticulartumor.
RoleofDesperationSurgery
TherearepatientswithNSGCTswhohaverisingtumormarkers,despiteoptimalsystemictherapy.Inthese
instances,surgerytoresectallvisibledisease,atermwecoin"desperationsurgery"couldbeconsidered.Itis
estimatedthatupto20%ofpatientswhofitthesecriteriamaybecuredwithsurgicalresection.Patientswith
isolatedretroperitoneallymphnodedisease,AFPonlyelevation,andwhoundergoacompleteresectionof
residualdiseasehavethemostfavorableoutcome.Referraltoacenterwithhighsurgicalexpertiseinthis
settingisrecommended,aspotentiallylargeenblocresectionsmayberequiredtoachievethedesiredoutcome
ofcompleteresection.
TreatmentofLateRelapse
Laterelapseisdefinedasdiseaserecurrenceafter24monthsfromprimaryBEPchemotherapy.Teratomaand
yolksacarethemostcommonhistologiesinthissetting,withpureteratomaconferringabetterprognosis.
Surgeryisthepreferredinitialtreatmentinthesecases,ifthetumorisfelttobecompletelyresectable.
23/42
24/4/2016
LateComplicationsofTherapy
Althoughrare,therearespecificcomplicationsassociatedwithtreatmentofGCTs,whichareespecially
importantinthispatientpopulation,ascurabilitymayleadtoanormallifeexpectancy.Secondaryleukemias
occurinfewerthan0.5%patientsandareassociatedwithuseofetoposide.Bleomycintoxicitycanappear
earlyandismostassociatedwithdosegreaterthan200IU.Patientsmayalsohaveincreasedriskofvascular
sideeffects,includingRaynaudsyndromeandhypertension.Upto25%ofpatientsmaydevelopthemetabolic
syndrome.Additionalcomplicationsincluderenalinsufficiency,chronicperipheralneuropathy,chronic
electrolyteabnormalities,andneuropsychiatricabnormalities.
Case362:Bep/TipFailure
A24yearoldmanpresentedwithlowerbackpain,anorexia,nightsweats,andweightloss.Imagingstudies
revealedextensiveretroperitoneallymphadenopathy,arighttesticularmass,andbilaterallungnodules.Tumor
markerswerehCG33,261,AFP4.1,andLDH1847.Afineneedleaspirationoftheretroperitonealmass
revealedembryonalcarcinoma.BEPchemotherapywasinitiated.ThekineticsofdeclineofserumhCGlevels
areshownbelowforthefirstthreeoutoffourplannedcycles:
s/pcycle1:1507
s/pcycle2:279
s/pcycle3:323
SalvagechemotherapyiscommencedafterthethirdcycleofBEP.ThepatientreceivedfourcyclesofTIP,
withdecreaseinadenopathyanddeclineofserumhCGtoundetectable.Thepatientwasthenreferredfor
RPLNDandrightradicalorchiectomy.Pathologyrevealednoviabletumor.Twomonthspostoperatively,
serumhCGroseto161.Hereceivedonecycleofirinotecan,paclitaxel,andoxaliplatinwithtumormarker
normalization.Hethenunderwenttandemperipheralbloodstemcelltransplantation(SCT)withhighdose
ICE.Heremainsdiseasefree3.5yearslater.
Comments:ForsymptomaticpatientswithintermediateorpoorriskGCTs,chemotherapycanbeinitiated
beforeorchiectomy.RisingtumormarkersduringBEPchemotherapysignalBEPfailureanddictatechangeof
therapy.ThebestresultsareachievedwithhighdosechemotherapyandSCT.
Case363:TheChallengeofManagingIntercurrentIllness
A35yearoldheavysmokerandmarijuanausermanunderwentaleftorchiectomyfora3.5cmmixed
NSGCTandpresented2monthslatertoMDACCwithleftgroinpainandleftthighnumbness.Tumormarkers
wereAFP6575,hCG1059,andLDH2441.CTscansrevealedbilaterallungnodules,alarge(14.7cm)
retroperitonealmass,lefthydronephrosis,andmultipleotherenlargedabdominalandpelviclymphnodes.
DuringthefirstBEPchemotherapycycle,hesufferedaninferiormyocardialinfarction(MI)secondarytoan
occludingatheroscleroticplaqueintherightcoronaryartery.Aftercoronarystentingandoptimalmedical
therapy,thepatientwasabletocompletefourcyclesofBEPonscheduleandatfulldose,withoutdelayor
significantcomplications,exceptformoderateperipheralneuropathy.Histumormarkersdeclinedasfollows:
FavoriteTable|Print
s/pcycle1 AFP=3853hCG=34.7
s/pcycle2 AFP=542hCG=5.2
s/pcycle3 AFP=88.1hCG=4.6
s/pcycle4 AFP=42hCG=4.7
Thepatientreceivedintramusculartestosteroneinjectionforlowserumtestosteronelevel,and3weekslater
24/42
24/4/2016
serumhCGwas<1.0.SixmonthsafterhisMI,thepatienthadresectionofthelargeleftretroperitonealmass,
theleftkidneyandleftadrenalgland,RPLND,andsegmentalresectionoftheleftpsoasmuscle.Pathologyof
thespecimenrevealed98%necrosisandonlytwomicroscopicfociofresidualviableESTintransitionto
adenocarcinoma.Thepatienthasbeenrecurrencefreefor3years.
Comments:Thiscaseillustratesthreepoints.Thefirstistheimportanceofpursuingchemotherapywhile
managinganintercurrentillness.Thesecondpointistorememberthattherearecausesofelevatedtumor
markersotherthantumor.ThethirdpointisthatwedonottreatfociofMTT.
Case364:DesperationSurgery
A46yearoldmanpresentedwithbackpainandwasfoundtohavean11cmretroperitonealmass,biopsyof
whichrevealedhighgradeGCT(Figure3611A).Heunderwentaleftradicalorchiectomyfora2.8cmmixed
GCT(99%seminoma,1%teratoma).Postoperatively,serumAFPwasgreaterthan10,000.Hereceivedsix
cyclesofEP,followedbyonecycleofVeIPbutneverachievedtumormarkernormalization(Figure3611B).
AtpresentationtoMDACC,hisserumAFPwas604.Thepatientreceivedmultipleadditionalcyclesof
rotatingsalvagechemotherapy,includingactinomycinD,cyclophosphamide,andetoposide(ACE)TIP,
cisplatinum,vincristine,methotrexate,andbleomycin(POMB)doxorubicin,paclitaxel,andgemcitabine
(ATG)andcisplatinum,cyclophosphamide,anddoxorubicin(CisCa)(Figure3611C).Thepatientdeveloped
renalinsufficiency,recalcitrantanemia,andgrade3peripheralneuropathy,andhadtransientnormalizationof
serumtumormarkerswhileawaitingsurgicalresection.Atthetimeofsurgery,serumAFPwas46.9.The
patientunderwentRPLNDwithexcisionofretroperitonealmasses,leftradicalnephrectomy,andexcisionof
retrocrurallymphnodemasses.PathologydemonstratedmetastaticmixedGCT,includingareasofEST,
matureteratoma,andfocalareassuspiciousforembryonalcarcinomaandchoriocarcinoma.Heremains
diseasefreepast5yearsfromthetimeofhissalvagesurgery.
Figure3611A.
25/42
24/4/2016
26/42
24/4/2016
27/42
24/4/2016
Baselineimagingofpatientdescribedincase364withlargeretroperitonealmass.
Figure3611B.
28/42
24/4/2016
29/42
24/4/2016
30/42
24/4/2016
Repeatimagingofpatientincase364aftersixcyclesofEP.
Figure3611C.
31/42
24/4/2016
32/42
24/4/2016
33/42
24/4/2016
Imagingofpatientfromcase364showingresidualdiseasedespitemultiplelinesofsalvagechemotherapy
priortodesperationsurgery.
Comments:FourcyclesofBEPandnotEPisthestandardforpatientswithintermediateandpoorrisk
NSGCT.Inrarecases,wherethetumormarkersdonotnormalize,evenafterexhaustingallchemotherapeutic
options,patientsmaybesalvagedsurgically.PatientswhohaveprimarilyAFPelevationandESTorteratoma
benefitthemostfromsuchanapproach.
Case365:GSTwithOccultPrimary
A29yearoldmanpresentedwithweightlossandleftsupraclavicularlymphadenopathy(seeFigure3612A),
buthadanegativetesticularexaminationandultrasound.Imagingstudiesconfirmeda5cmleft
supraclavicularlymphnodeandshowedasmallleftpleuraleffusion.Abiopsyofthesupraclavicularlymph
nodedemonstratedpoorlydifferentiatedadenocarcinoma.Embryonalcarcinomacouldnotbeexcluded.
ImmunostainsforPLAPandKi1werepositivebutwerenegativeforAFPandinconclusiveforhCG.
Laboratoryevaluationrevealedazoospermiabutnormalserumchemistriesandtumormarkers.Thepatient
wastreatedwiththreecyclesofBEPandachievedacompleteremissionandisnowdiseasefreefor5years
withoutsurgicalconsolidation(Figure3612B).
Figure3612A.
34/42
24/4/2016
35/42
24/4/2016
BaselineimagingofpatientdescribedinCase365showingbulkyleftsupraclavicularadenopathy..
Figure3612B.
36/42
24/4/2016
37/42
24/4/2016
Imagingafterthreecyclesofchemotherapy.
Comments:Thecaseofunknownprimarycarcinomainayoungman,eveniftumormarkersarenegative,
shouldraisethediagnosisofGCTandshouldbetreatedassuch.Surgicalconsolidationisnotalways
necessary,whenaclinicalcompleteresponseisachievedwithchemotherapy.
ExtragonadalGermCellTumors
Patientswithseminomasarisinginthemediastinumhavesimilarprognosistopatientswithtesticular
seminomasandaretreatedwithfourcyclesofEPatourinstitution,iftheydonothavenonpulmonaryvisceral
metastasis.NonseminomatousextragonadalGCTsrepresentadistinctsubsetofGCTsandcarryapoorer
prognosisthanprimarytesticularNSGCTs.Themostcommonoriginisthemediastinum,buttheycanalso
ariseintheretroperitoneumorpinealregion.Rarecasesinvolvethevagina,prostate,liver,andorbit.
MediastinalEGCTsappearaslargeanteriormassesonradiographs.Thissubsetischaracterizedby
prominenceofESTandteratomahistology,comparedtoprimarytesticularGCTs(53).Initialdiagnosismay
beaidedbyelevationsofAFPorhCG.Klinefeltersyndromeisassociatedwithincreasedriskofprimary
nonseminomatousmediastinalGCTs(54).Additionalassociationsincludeacutemegakaryoblasticleukemia,
acutemyeloidleukemia,myelodysplasticsyndrome,andmalignanthistiocytosis.Someofthesecases
representmalignanttransformationofimmatureteratomaelements.
NonseminomatousGCTsareclassifiedashighriskGCTs(2),anddatasuggestthatlongtermsurvivalisas
lowas20%(5557).Theaggressivenatureofthisentityiscoupledbythesurgicaldifficultyofresectionof
residualdiseaseaftertherapy.EarlydiagnosisandaggressiveresectionofmediastinalNSGCTsmayimprove
38/42
24/4/2016
theoutcome.Atourinstitution,thetreatmentstrategyforthisrareentityincludespresurgicalchemotherapyto
optimumresponseandthenconsolidationsurgery.
Conclusion
GCTsrepresenttheparadigmofcurablesolidtumors.Optimalmanagementofthesepatientsrequiresa
multidisciplinaryapproach,integratingchemotherapyandsurgery,toachievethehighestcurerates.Patients
whoposeauniquediagnosticortherapeuticchallengeshouldbeconsideredforearlyreferraltoalargetertiary
carecenter.
References
1.AmericanCancerSociety.CancerFactsandFigures2009.Atlanta:AmericanCancerSociety2009.
2.InternationalGermCellCancerCollaborativeGroup.Internationalgermcellconsensusclassification:A
prognosticfactorbasedstagingsystemformetastaticgermcellcancers.JClinOnc199715:594603.
3.VanDijkMR,SteyerbergEW,HabbemaDF.Survivalofnonseminomatousgermcellcancerpatients
accordingtotheIGCCCGclassification:Anupdatebasedonmetaanalysis.EurJCancer200642:820826.
4.BrayF,FerlayJ,DevesaSS,etal.Interpretingtheinternationaltrendsintesticularseminomaand
nonseminomaincidence.NatClinPractUrol20063:532543.[PubMed:17031378]
5.McGlynnKA,DevesaSS,GraubardBI,etal.Increasingincidenceoftesticulargermcelltumorsamong
blackmenintheUnitedStates.JCO200523:57575761.[PubMed:16110032]
6.McGlynnKA,DevesaSS,SigurdsonAJ,etal.Trendsintheincidenceoftesticulargermcelltumorsinthe
UnitedStates.Cancer200397:6370.[PubMed:12491506]
7.DieckmannKP,PicjlmeierU.Clinicalepidemiologyoftesticulargermcelltumors.WorldJUrol200422:2
14.[PubMed:15034740]
8.HannaN,TimmermanR,FosterR,etal.Testiscancer.In:KufeD,PollockR,WeichselbaumR,etal(eds):
CancerMedicine.Hamilton,Ontario:BCDecker2003:17471768.
9.MollerH,CortesD,EngholmG,etal.Riskoftesticularcancerwithcryptorchidismandwithtesticular
biopsy:Cohortstudy.BrJMed1998317:729730.[PubMed:9732342]
10.GiwercmanA,BrunnE,FrimodtMollerC,etal.Prevalenceofcarcinomainsituandotherhistopathologic
abnormalitiesintestesofmenwithcryptorchidism.JUrol1989142:9981001.[PubMed:2571738]
11.DieckmannKP,PichlmeierU.Theprevalenceoffamilialtesticularcancer:Ananalysisoftwopatient
populationsandareviewoftheliterature.Cancer199780:19541960.[PubMed:9366298]
12.TravisLB,CurtisRE,StormH,etal.Riskofsecondmalignantneoplasmsamonglongtermsurvivorsof
testicularcancer.JNatlCancerInst199789:14291439.[PubMed:9326912]
13.BoslGJ,IlsonDH,RodriguezE,etal.Clinicalrelevanceofthei(12p)markerchromosomeingermcell
tumors.JNatlCancerInst199486:349355.[PubMed:8308927]
14.AtkinNB,BakerMC.Specificchromosomechangei(12p)intesticulartumors.Lancet19822:1349.
[PubMed:6128640]
15.RodriguezE,MatthewS,ReuterV,etal.Cytogeneticanalysisof124prospectivelyascertainedgermcell
tumors.CancerRes199252:22852291.[PubMed:1313741]
16.SumersgillG,GokerH,WeberHallS,etal.Molecularcytogeneticanalysisofadulttesticulargermcell
tumorsandidentificationofregionsofconsensuscopynumberchange.BrJCancer199877:305313.
17.KersemaekersAMF,MayerF,MolierM,etal.Roleofp53andMDM2intreatmentresponseofhuman
germcelltumors.JClinOncol200220:15511561.[PubMed:11896104]
18.KorkolaJE,HouldsworthJ,FeldmanDR,etal.Identificationandvalidationofageneexpressionsignature
thatpredictsoutcomeinadultmenwithgermcelltumors.JClinOncol200927:52405247.[PubMed:
19770384]
19.HorieK,FujitaJ,TakakuraH,etal.Theexpressionofckitproteininhumanadultandfetaltissues.Hum
Reprod19938:19551962.[PubMed:7507133]
20.HoeiHanseniCE,RajpertDeMeytsiE,DaugaardG,etal.Carcinomainsitutestis,theprogenitorof
testiculargermcelltumours:Aclinicalreview.AnnOncol200516:863868.
39/42
24/4/2016
21.BraunsteinGD.Gynecomastia.NEnglJMed2007357:12291237.[PubMed:17881754]
22.WehmannRE,NisulaBC.Metabolicandrenalclearanceratesofpurifiedhumanchorionicgonadotropin.J
ClinInvest198168:184194.[PubMed:7251859]
23.GiraltSA,DexeusF,AmatoR,etal.Hyperthyroidisminmenwithgermcelltumorsandhighlevelsof
betahumanchorionicgonadotropin.Cancer199269:12861290.[PubMed:1371235]
24.LightPA.Tumourmarkersintesticularcancer.JRSocMed198578(Suppl6):1924.
25.YuasaT,YoshikiT,OgawaO,etal.DetectionofalphafetoproteinmRNAinseminoma.JAndrol
199920:336340.[PubMed:10386812]
26.MencelPJ,MotzerRJ,MazumdarM,etal.Advancedseminoma:Treatmentresults,survival,and
prognosticfactorsin142patients.JClinOncol199412:120126.[PubMed:7505805]
27.EdgeSB,ByrdDR,ComptonCC,etal.AJCCCancerStagingManual,6thed.NewYork,Springer,2009.
28.JerussJS,WoodruffTK.Preservationoffertilityinpatientswithcancer.NEnglJMed2009360:902911.
[PubMed:19246362]
29.NazeerT,RoJY,KeeKH,etal.Spermaticcordcontaminationintesticularcancer.ModPathol
19969:762766.[PubMed:8832559]
30.ChungPWM,BayleyAJS,SweetJ,etal.Spermatocyticseminoma:Areview.EurUrol200445:495498.
[PubMed:15041115]
31.WardeP,SpechtL,HorwichA,etal.PrognosticfactorsforrelapseinstageIseminomamanagedby
surveillance:Apooledanalysis.JClinOncol200220:44484452.[PubMed:12431967]
32.JonesWG,FossaSD,MeadGM,etal.Randomizedtrialof30versus20Gyintheadjuvanttreatmentof
stageItesticularseminoma:AreportonMedicalResearchCouncilTrialTE18,EuropeanOrganisationforthe
ResearchandTreatmentofCancerTrial30942.JClinOncol200523:12001208.[PubMed:15718317]
33.FossSD,HorwichA,RussellJM,etal.OptimalplanningtargetvolumeforstageItesticularseminoma:
AMedicalResearchCouncilrandomizedtrial.MedicalResearchCouncilTesticularTumorWorkingGroup.J
ClinOncol199917:1146.[PubMed:21658654]
34.OliverRTD,MasonMD,MeadGM,etal.Radiotherapyversussingledosecarboplatininadjuvant
treatmentofstageIseminoma:Arandomizedtrial.Lancet2005366:293300.[PubMed:16039331]
35.ClassenJ,SchmidbergerH,MeisnerC,etal.RadiotherapyforstagesIIA/Btesticularseminoma:Final
reportofaprospectivemulticenterclinicaltrial.JClinOncol200321:11011106.[PubMed:12637477]
36.XiaoH,MazumdarM,BajorinD,etal.Longtermfollowupofpatientswithgoodriskgermcelltumors
treatedwithetoposideandcisplatin.JClinOncol199715:25532558.[PubMed:9215824]
37.SaxmanSB,FinchD,GoninR,etal.LongtermfollowupofaphaseIIIstudyofthreeversusfourcycles
ofbleomycin,etoposide,andcisplatininfavorableprognosisgermcelltumors:TheIndianaUniversity
Experience.JClinOncol199816:702706.[PubMed:9469360]
38.deWitR,RobertsJT,WilkinsonPM,etal.Equivalenceofthreeorfourcyclesofbleomycin,etoposide,
andcisplatinchemotherapyandofa3or5dayscheduleingoodprognosisgermcellcancer:Arandomized
studyoftheEuropeanOrganizationforResearchandTreatmentofCancerGenitourinaryTractCancer
CooperativeGroupandtheMedicalResearchCouncil.JClinOncol200119:16291640.
39.KondaguntaGV,BacikJ,BajorinD,etal.Etoposideandcisplatinchemotherapyformetastaticgoodrisk
germcelltumors.JClinOncol200523:92909294.[PubMed:16361627]
40.DeSantisM,BokemeyerC,BechererA,etal.PredictiveImpactof218Fluoro2DeoxyDGlucose
positronemissiontomographyforresidualpostchemotherapymassesinpatientswithbulkyseminoma.JClin
Oncol200119:37403744.
41.VukyJ,TickooSK,SheinfeldJ,etal.Salvagechemotherapyforpatientswithadvancedpureseminoma.J
ClinOncol200220:297301.[PubMed:11773182]
42.EinhornLH,WilliamsSD,ChamnessA,etal.Highdosechemotherapyandstemcellrescueformetastatic
germcelltumors.NEnglJMed2007357:340348.[PubMed:17652649]
43.SpiessPE,PistersLL,LiuP,etal.Malignanttransformationoftesticularteratoma:Achemoresistant
phenotype.UrolOncol200826:595599.[PubMed:18367105]
44.BoslGJ,GellerN,CirrincioneC,etal.Interrelationshipsofhistopathologyandotherclinicalvariablesin
patientswithgermcelltumorsofthetestis.Cancer198351:21212125.[PubMed:6188528]
45.LogothetisCJ,SamuelsML,TrindadeA,etal.Thegrowingteratomasyndrome.Cancer198250:1629
1635.[PubMed:6288220]
40/42
24/4/2016
46.AlbersP,SienerR,KlieschS,etal.RiskfactorsforrelapseinclinicalstageInonseminomatoustesticular
germcelltumors:ResultsoftheGermanTesticularCancerStudyGroupTrial.JClinOncol200321:1505
1512.[PubMed:12697874]
47.KregeS,BeyerJ,SouchonR,etal.Europeanconsensusconferenceondiagnosisandtreatmentofgerm
cellcancer:AreportoftheSecondMeetingoftheEuropeanGermCellCancerConsensusgroup(EGCCCG):
Part1.EurUrol200853:478496.[PubMed:18191324]
48.MotzerRJ,BolgerGB,BostonB,etal.Testicularcancer:Clinicalpracticeguidelinesinoncology.JNatl
ComprCancNetw20064:10381058.[PubMed:17112452]
49.StephensonAJ,BoslGJ,MotzerRJ,etal.Retroperitoneallymphnodedissectionfornonseminomatous
germcelltesticularcancer:Impactofpatientselectionfactorsonoutcome.JClinOncol200523:27812788.
[PubMed:15837993]
50.AlbersP,SienerR,KregeS,etal.RandomizedphaseIIItrialcomparingretroperitoneallymphnode
dissectionwithoncecourseofbleomycinandetoposidepluscisplatinchemotherapyintheadjuvanttreatment
ofclinicalstageInonseminomatoustesticulargermcelltumors:AUOTrialAH01/94bytheGerman
TesticularCancerStudyGroup.JClinOncol200826:29662972.[PubMed:18458040]
51.TandstadT,DahlO,CohnCedermarkG,etal.RiskadaptedtreatmentinclinicalstageInonseminomatous
germcelltesticularcancer:TheSWENOTECAManagementProgram.JClinOncol200927:21222128.
[PubMed:19307506]
52.HintonS,CatalanoPJ,EinhornLH,etal.Cisplatin,etoposideandeitherbleomycinorifosfamideinthe
treatmentofdisseminatedgermcelltumors:Finalanalysisofanintergrouptrial.Cancer200397:18691875.
[PubMed:12673712]
53.MoranCA,SusterS.Primarygermcelltumorsofthemediastinum:I.Analysisof322caseswithspecial
emphasisonteratomatouslesionsandaproposalforhistopathologicclassificationandclinicalstaging.Cancer
199780:681690.[PubMed:9264351]
54.NicholsCR,HeeremaNA,PalmerC,etal.Klinefelter'ssyndromeassociatedwithmediastinalgermcell
neoplasms.JClinOncol19875:12901294.[PubMed:3040921]
55.LogothetisCJ,SamuelsML,SeligDE,etal.Chemotherapyofextragonadalgermcelltumors.JClin
Oncol19853:316325.[PubMed:2579212]
56.TonerGC,GellerNL,LinSY,etal.Extragonadalandpoorrisknonseminomatousgermcelltumors.
Survivalandprognosticfeatures.Cancer199167:20492057.[PubMed:1848473]
57.MoranCA,SusterS,KossMN.Primarygermcelltumorsofthemediastinum:III.Yolksactumor,
embryonalcarcinoma,choriocarcinoma,andcombinednonteratomatousgermcelltumorsofthemediastinum
aclinicopathologicandimmunohistochemicalstudyof64cases.Cancer199780:699707.[PubMed:
9264353]
undefined
McGrawHill
CopyrightMcGrawHillGlobalEducationHoldings,LLC.
Allrightsreserved.
YourIPaddressis189.149.255.191
AccessProvidedby:UniversidadAutonomadeYucatan
Silverchair
Histologicalappearanceofclassicseminoma.
Grossappearanceofseminoma.
Managementoftesticularcancer(seminoma).
Baselineimagingfromcase361showingalargeleftretroperitonealmasswithlefthydronephosis.
41/42
24/4/2016
Repeatimagingfrompatientincase361showingmarkedimprovementinmassafter3cyclesof
chemotherapy.
Histologicalappearanceofembryonalcarcinoma.
HistologicalappearanceofESTcarcinoma.
Histologicalappearanceofchoriocarcinoma.
Histologicalappearanceofteratoma.
Grossappearanceofteratoma.
Managementoftesticularcancer(nonseminoma).
Baselineimagingofpatientdescribedincase364withlargeretroperitonealmass.
Repeatimagingofpatientincase364aftersixcyclesofEP.
Imagingofpatientfromcase364showingresidualdiseasedespitemultiplelinesofsalvagechemotherapy
priortodesperationsurgery.
BaselineimagingofpatientdescribedinCase365showingbulkyleftsupraclavicularadenopathy..
Imagingafterthreecyclesofchemotherapy.
42/42
Das könnte Ihnen auch gefallen
- Farmacos Carro RojoDokument34 SeitenFarmacos Carro RojoJacob Diaz100% (1)
- Tumores en El MediastinoDokument28 SeitenTumores en El MediastinoRabi Armando Aranda OntiverosNoch keine Bewertungen
- Urologia TumoresDokument22 SeitenUrologia TumoresRabi Armando Aranda OntiverosNoch keine Bewertungen
- Uso de QuimioterapiaDokument9 SeitenUso de QuimioterapiaRabi Armando Aranda OntiverosNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Safe Handling of CytotoxicsDokument11 SeitenSafe Handling of CytotoxicskaramNoch keine Bewertungen
- About Thyroid Cancer: Overview and TypesDokument12 SeitenAbout Thyroid Cancer: Overview and Typesumaima rizwanNoch keine Bewertungen
- Nursing Management Child With CancerDokument7 SeitenNursing Management Child With CancerlisalovNoch keine Bewertungen
- Full Dataset of Papers FormattedDokument234 SeitenFull Dataset of Papers FormattedoafsNoch keine Bewertungen
- Go Go Go First Vita PlusDokument6 SeitenGo Go Go First Vita PlusArnulfo Yu LanibaNoch keine Bewertungen
- Acute Lymphocytic LeukemiaDokument8 SeitenAcute Lymphocytic LeukemiaWendy EscalanteNoch keine Bewertungen
- US20050014785A1 - Patent ChloroquneDokument16 SeitenUS20050014785A1 - Patent ChloroquneHector CorralesNoch keine Bewertungen
- Nursing Excellence StandardsDokument49 SeitenNursing Excellence StandardsD. GandhirajNoch keine Bewertungen
- Fefg EBM 2017 18 23 MarchDokument26 SeitenFefg EBM 2017 18 23 MarchShivam AgarwalNoch keine Bewertungen
- Brain CancerDokument24 SeitenBrain CancerJohn Lester FernandezNoch keine Bewertungen
- Survival With Cemiplimab in Recurrent Cervical CancerDokument12 SeitenSurvival With Cemiplimab in Recurrent Cervical CancerKassem HijazyNoch keine Bewertungen
- Deeper Trial - Asco 2021Dokument26 SeitenDeeper Trial - Asco 2021Vuong Dinh Thy HaoNoch keine Bewertungen
- The Dry Fasting Miracle From Deprive To T - Luke CoutinhoDokument106 SeitenThe Dry Fasting Miracle From Deprive To T - Luke Coutinhoseerat75% (4)
- Biomedical Waste ManagementDokument31 SeitenBiomedical Waste ManagementSaravanakumar MNoch keine Bewertungen
- Immuno Modulator yDokument377 SeitenImmuno Modulator ysaman7752Noch keine Bewertungen
- DactinomycinDokument1 SeiteDactinomycinIvanne Hisoler0% (2)
- Mucositis GuidlinesDokument13 SeitenMucositis GuidlinesEman MossanNoch keine Bewertungen
- Sfda Approved Drug Mar2021Dokument9 SeitenSfda Approved Drug Mar2021iyad.alsabiNoch keine Bewertungen
- Speaking 35 SamplesDokument35 SeitenSpeaking 35 SamplesJoanmanabat100% (5)
- Compounded Sterile Products Stability Compendium-AntineoplasticsDokument0 SeitenCompounded Sterile Products Stability Compendium-AntineoplasticsRahmalia 'lia Cudby' PrihanantoNoch keine Bewertungen
- Branwyn March 2014Dokument22 SeitenBranwyn March 2014Sneha Rahul ChoudharyNoch keine Bewertungen
- KefirDokument9 SeitenKefirMilliNoch keine Bewertungen
- Wit Medical Terms 3Dokument14 SeitenWit Medical Terms 3directorizlarNoch keine Bewertungen
- 6 Vol. 7 Issue 9 September 2016 IJPSR RE 1915Dokument9 Seiten6 Vol. 7 Issue 9 September 2016 IJPSR RE 1915Nur KhasanahNoch keine Bewertungen
- Testicular CancerDokument21 SeitenTesticular CancerRachel Julianne MoralesNoch keine Bewertungen
- Chapter 07 - Hematologic ProblemsDokument8 SeitenChapter 07 - Hematologic ProblemscariNoch keine Bewertungen
- 216 Finals ReviewerDokument8 Seiten216 Finals Reviewertrlopez4405valNoch keine Bewertungen
- Concept Map LeukemiaDokument7 SeitenConcept Map LeukemiaDiane AbanillaNoch keine Bewertungen
- Time Content A.V. - Aids Evaluation Specific Objectives Teaching of LearningDokument12 SeitenTime Content A.V. - Aids Evaluation Specific Objectives Teaching of LearningYashwanth ReguntaNoch keine Bewertungen
- B Pharm 6 Sem Pharmalite - inDokument18 SeitenB Pharm 6 Sem Pharmalite - insatyaroxx258Noch keine Bewertungen