Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- NantesDiagnosticCriteria For Pudendal NeuralgiaDokument5 SeitenNantesDiagnosticCriteria For Pudendal NeuralgiaTeresa BeckNoch keine Bewertungen
- Moraxella SPP, Sphingomonas SPPDokument31 SeitenMoraxella SPP, Sphingomonas SPPDayledaniel SorvetoNoch keine Bewertungen
- Article - CVD Cardiac Arrest - Bls AclsDokument2 SeitenArticle - CVD Cardiac Arrest - Bls AclsAkhosh SomarajanNoch keine Bewertungen
- Sistem Pelaporan Dan Pembelajaran Keselamatan Pasien RS Arjaty 2022Dokument13 SeitenSistem Pelaporan Dan Pembelajaran Keselamatan Pasien RS Arjaty 2022vera kusunyadewiNoch keine Bewertungen
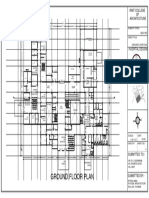
- Ground Floor Plan Sheet 2Dokument1 SeiteGround Floor Plan Sheet 2riteshNoch keine Bewertungen
- Can Oral Sex Cause Throat CancerDokument4 SeitenCan Oral Sex Cause Throat CancerjyuldipNoch keine Bewertungen
- Urinary Tract Infection: DR Badriya Al-Mahrouqi 12/11/2017Dokument51 SeitenUrinary Tract Infection: DR Badriya Al-Mahrouqi 12/11/2017NinaNoch keine Bewertungen
- Disease Deficient Enzyme Cardinal Clinical Features Glycogen Structure Von Gierke'sDokument84 SeitenDisease Deficient Enzyme Cardinal Clinical Features Glycogen Structure Von Gierke'sclubstar100% (4)
- Pediatric Physiology 2007Dokument378 SeitenPediatric Physiology 2007Andres Jeria Diaz100% (1)
- Drug Descrubrimiento de FarmacosDokument302 SeitenDrug Descrubrimiento de FarmacosdavidNoch keine Bewertungen
- Rectal ProlapseDokument9 SeitenRectal ProlapseAnjani Putri RetnaninggalihNoch keine Bewertungen
- Basic Principles of Normal ECG: Prepared By: Ben Ryan Jucay SauceDokument25 SeitenBasic Principles of Normal ECG: Prepared By: Ben Ryan Jucay SauceSoySauceNoch keine Bewertungen
- EDIC Guidelines 2017 PDFDokument22 SeitenEDIC Guidelines 2017 PDFZia ShaikhNoch keine Bewertungen
- Lactated Ringer'sDokument7 SeitenLactated Ringer'sPPLaloNoch keine Bewertungen
- Aseptic MeningitisDokument24 SeitenAseptic Meningitisidno1008100% (1)
- Item Balance Per Unit RPTDokument60 SeitenItem Balance Per Unit RPTYogie 1290Noch keine Bewertungen
- HerbalismDokument18 SeitenHerbalismmieNoch keine Bewertungen
- Mike's Recommended Books For Paramedic StudentsDokument3 SeitenMike's Recommended Books For Paramedic StudentsMichael WilsonNoch keine Bewertungen
- Intramedullary Nailing For Femur Fracture Web Version EnglishDokument6 SeitenIntramedullary Nailing For Femur Fracture Web Version EnglishCarima JatnoNoch keine Bewertungen
- ProspectusDokument156 SeitenProspectusNareshNoch keine Bewertungen
- 17q21.31 Microdeletions FTNWDokument8 Seiten17q21.31 Microdeletions FTNWjohavenbNoch keine Bewertungen
- Khalil High Yeild Step 2 Cs Mnemonic 2nd EdDokument24 SeitenKhalil High Yeild Step 2 Cs Mnemonic 2nd EdCarolina Lopez100% (1)
- Sources of Homeopathic DrugsDokument35 SeitenSources of Homeopathic Drugsnadiida83% (6)
- Resume PortfolioDokument1 SeiteResume Portfolioapi-386291240Noch keine Bewertungen
- 5th Handbook of Transfusion MedicineDokument186 Seiten5th Handbook of Transfusion MedicineDokter Dhea Danni Agisty100% (1)
- Skin Care Plan: Nu Derm Protocol ForDokument7 SeitenSkin Care Plan: Nu Derm Protocol ForsheilaNoch keine Bewertungen
- Oral Alerting ActivitiesDokument3 SeitenOral Alerting ActivitiesAnn VillablancaNoch keine Bewertungen
- Techniques For Parasite Egg Identification in Faecal SamplesDokument9 SeitenTechniques For Parasite Egg Identification in Faecal SamplesDr.Kedar Karki ,M.V.Sc.Preventive Vet.Medicine CLSU Philippines100% (2)
- Biopharmaceutics and Clinical Pharmacokinetics - 20210831 - 212949Dokument22 SeitenBiopharmaceutics and Clinical Pharmacokinetics - 20210831 - 212949Md. Abu Bakar Siddique TayefNoch keine Bewertungen