Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Cardiac Surgery MCQDokument43 SeitenCardiac Surgery MCQprofarmah100% (7)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Fetal Cerebro-Placental Ratio and Adverse Perinatal Outcome: Systematic Review and Meta-Analysis of The Association and Diagnostic PerformanceDokument8 SeitenFetal Cerebro-Placental Ratio and Adverse Perinatal Outcome: Systematic Review and Meta-Analysis of The Association and Diagnostic Performancebidan22Noch keine Bewertungen
- Diagnostics 07 00012Dokument10 SeitenDiagnostics 07 00012bidan22Noch keine Bewertungen
- European Journal of Obstetrics & Gynecology and Reproductive BiologyDokument15 SeitenEuropean Journal of Obstetrics & Gynecology and Reproductive Biologybidan22Noch keine Bewertungen
- Menopause Hormone Replacement TherapyDokument4 SeitenMenopause Hormone Replacement Therapybidan22Noch keine Bewertungen
- AmniotomiDokument8 SeitenAmniotomibidan22Noch keine Bewertungen
- Early Amniotomy After Vaginal Misoprostol For Induction of Labor: A Randomized Clinical TrialDokument5 SeitenEarly Amniotomy After Vaginal Misoprostol For Induction of Labor: A Randomized Clinical Trialbidan22Noch keine Bewertungen
- Abnormal Vaginal Bleeding Policar 051611Dokument69 SeitenAbnormal Vaginal Bleeding Policar 051611bidan22Noch keine Bewertungen
- Antiphospholipid Antibody Syndrome and PregnancyDokument17 SeitenAntiphospholipid Antibody Syndrome and Pregnancybidan22Noch keine Bewertungen
- Chlorpheniramine MaleateDokument3 SeitenChlorpheniramine Maleateapi-3797941100% (1)
- Renal Clearance 2Dokument3 SeitenRenal Clearance 2Ine Marthia DanieNoch keine Bewertungen
- Quiz I Categorical Data AnalysisDokument2 SeitenQuiz I Categorical Data Analysisfatima fatimaNoch keine Bewertungen
- Sensus Harian TGL 05 Maret 2022........Dokument104 SeitenSensus Harian TGL 05 Maret 2022........Ruhut Putra SinuratNoch keine Bewertungen
- Daftar Pasien RSUP H. Adam Malik Medan - Senin, 24 Juli 2023Dokument3 SeitenDaftar Pasien RSUP H. Adam Malik Medan - Senin, 24 Juli 2023Admin neuro-usu.idNoch keine Bewertungen
- Norethisterone JournalDokument29 SeitenNorethisterone JournalAditya Syah PutraNoch keine Bewertungen
- Homeopathic Detox Therapy (HDT) - Interview Ton Jansen - August 2014Dokument21 SeitenHomeopathic Detox Therapy (HDT) - Interview Ton Jansen - August 2014Yuldash100% (2)
- Boyd & Griffin Classification (1949)Dokument14 SeitenBoyd & Griffin Classification (1949)João Pedro ZenattoNoch keine Bewertungen
- 3.4-Behar Anorexia y MadurezDokument10 Seiten3.4-Behar Anorexia y MadurezAlejandra CarmonaNoch keine Bewertungen
- Resveratrol and Its Effects On Human Health and LongevityDokument367 SeitenResveratrol and Its Effects On Human Health and LongevityArnulfo Yu LanibaNoch keine Bewertungen
- Manual of Obstetrics, 8e (Jun 25, 2014) - (1451186770) - (LWW) PDFDokument766 SeitenManual of Obstetrics, 8e (Jun 25, 2014) - (1451186770) - (LWW) PDFPrem100% (9)
- Pharmacoeconomics - : Lebanese International University School of Pharmacy Fall 2021-2022Dokument18 SeitenPharmacoeconomics - : Lebanese International University School of Pharmacy Fall 2021-2022undeadrebornNoch keine Bewertungen
- Mother To Child Transmition of HIVDokument23 SeitenMother To Child Transmition of HIVGenoveva Maditias Dwi PertiwiNoch keine Bewertungen
- Drug StudyDokument7 SeitenDrug Studyanne009Noch keine Bewertungen
- CV For FellowshipDokument3 SeitenCV For Fellowshipapi-568710214Noch keine Bewertungen
- Virtual Notebook 1.1.3 Part 2 - Notebook - Day 2Dokument6 SeitenVirtual Notebook 1.1.3 Part 2 - Notebook - Day 2Justice JensenNoch keine Bewertungen
- B. Mahmoud - Salmonella - A Dangerous Foodborne Pathogen-Intech (2011)Dokument450 SeitenB. Mahmoud - Salmonella - A Dangerous Foodborne Pathogen-Intech (2011)kiệt lêNoch keine Bewertungen
- Anti Tuberculosis AgentsDokument15 SeitenAnti Tuberculosis Agentsejg26100% (1)
- Form 86 2022 Health Examination RecordDokument1 SeiteForm 86 2022 Health Examination RecordMA. GLIZA TANNoch keine Bewertungen
- Occlusal Dysesthesia or Phantom BiteDokument14 SeitenOcclusal Dysesthesia or Phantom BitebryanabauerNoch keine Bewertungen
- Drug Study-Ceftriaxone ClindamycinDokument2 SeitenDrug Study-Ceftriaxone ClindamycinDavid VillanuevaNoch keine Bewertungen
- Type 2 Diabetes MellitusDokument4 SeitenType 2 Diabetes MellitusMazhar WarisNoch keine Bewertungen
- Planning: NCP #1 Chronic Pain Related To Compression of Spinal Nerves As Evidenced byDokument10 SeitenPlanning: NCP #1 Chronic Pain Related To Compression of Spinal Nerves As Evidenced byNicole Anne TungolNoch keine Bewertungen
- Case No 37Dokument5 SeitenCase No 37Aila GoliasNoch keine Bewertungen
- Lesson 3 - Internet Addiction: Activity 1 - Pre-Learn VocabularyDokument8 SeitenLesson 3 - Internet Addiction: Activity 1 - Pre-Learn VocabularyLyon WooNoch keine Bewertungen
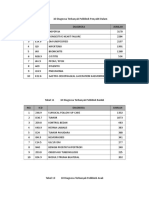
- 10 Diagnosa PenyakitDokument3 Seiten10 Diagnosa PenyakitDiny Rachma Putri HNoch keine Bewertungen
- Silabus Rmo 2021Dokument13 SeitenSilabus Rmo 2021Nuzlan NuariNoch keine Bewertungen
- Drugs For Diabetes MellitusDokument3 SeitenDrugs For Diabetes MellitusGerardLum100% (1)
- Encopresis in Children An Overview of Recent FindiDokument5 SeitenEncopresis in Children An Overview of Recent FindiMaulana MalikNoch keine Bewertungen