Das könnte Ihnen auch gefallen
- Stress Urinary Incontinence in Relation To Pelvic Floor Muscle StrengthDokument10 SeitenStress Urinary Incontinence in Relation To Pelvic Floor Muscle StrengthNoraNoch keine Bewertungen
- Antenatal Care and Its Effect On Risk of PihDokument11 SeitenAntenatal Care and Its Effect On Risk of PihNoraNoch keine Bewertungen
- Thyroid Hormonal Changes Among Women With Polycystic Ovarian SyndromeDokument14 SeitenThyroid Hormonal Changes Among Women With Polycystic Ovarian SyndromeNoraNoch keine Bewertungen
- Female Circumcision: Limiting The Harm (Version 2 Peer Review: 2 Approved, 1 Approved With Reservations)Dokument8 SeitenFemale Circumcision: Limiting The Harm (Version 2 Peer Review: 2 Approved, 1 Approved With Reservations)NoraNoch keine Bewertungen
- Pregnancy in A Patient With Recurrent GlioblastomaDokument6 SeitenPregnancy in A Patient With Recurrent GlioblastomaNoraNoch keine Bewertungen
- Abdul Halim, Abu Sayeed Md. Abdullah, Fazlur Rahman, Animesh BiswasDokument11 SeitenAbdul Halim, Abu Sayeed Md. Abdullah, Fazlur Rahman, Animesh BiswasNoraNoch keine Bewertungen
- Anaemia On First Trimester PregnancyDokument11 SeitenAnaemia On First Trimester PregnancyNoraNoch keine Bewertungen
- Bakri Balloon PDFDokument5 SeitenBakri Balloon PDFNoraNoch keine Bewertungen
- Injections SiteDokument10 SeitenInjections SiteNora100% (2)
- Preterm DeliveryDokument12 SeitenPreterm DeliveryNoraNoch keine Bewertungen
- Active Management of Pregnant Cancer PatientDokument9 SeitenActive Management of Pregnant Cancer PatientNoraNoch keine Bewertungen
- Menu Makanan Untuk Pesakit Hospital: IsninDokument2 SeitenMenu Makanan Untuk Pesakit Hospital: IsninNoraNoch keine Bewertungen
- A Randomized Trial of Coached Versus Uncoached Maternal Pushing During The Second Stage of Labor 2006 American Journal of Obstetrics and GynecologyDokument4 SeitenA Randomized Trial of Coached Versus Uncoached Maternal Pushing During The Second Stage of Labor 2006 American Journal of Obstetrics and GynecologyNoraNoch keine Bewertungen
- Pressure Points - Postnatal Care Planning PDFDokument15 SeitenPressure Points - Postnatal Care Planning PDFNoraNoch keine Bewertungen
- Nursing ManagerDokument30 SeitenNursing ManagerNoraNoch keine Bewertungen
- Orientation ListDokument1 SeiteOrientation ListNoraNoch keine Bewertungen
- End of Life Care BrochureDokument2 SeitenEnd of Life Care BrochureNoraNoch keine Bewertungen
- BSSDokument4 SeitenBSSNoraNoch keine Bewertungen
- Kwawu Foster Kwesi - Breast Cancer, Knowledge, Attitudes and Perception Amongs Female Soldiers of The Ghana Armed Forces in The Greater Accra Region - 2009 PDFDokument93 SeitenKwawu Foster Kwesi - Breast Cancer, Knowledge, Attitudes and Perception Amongs Female Soldiers of The Ghana Armed Forces in The Greater Accra Region - 2009 PDFNoraNoch keine Bewertungen
- Didik UPSR 2017 TARIKH 9.1.2017 - 1079367617 PDFDokument15 SeitenDidik UPSR 2017 TARIKH 9.1.2017 - 1079367617 PDFPencil Box100% (2)
- Vaccination in Pregnancy PDFDokument7 SeitenVaccination in Pregnancy PDFNoraNoch keine Bewertungen
- Active Labor Duration and Dilation Rates Among Low Risk Nulliparous Women With Spontaneous Labor Onset A Systematic Review 2010 Journal of MidwiferyDokument11 SeitenActive Labor Duration and Dilation Rates Among Low Risk Nulliparous Women With Spontaneous Labor Onset A Systematic Review 2010 Journal of MidwiferyNoraNoch keine Bewertungen
- Prenatal Care by Connie Sussan AustenDokument31 SeitenPrenatal Care by Connie Sussan AustenNoraNoch keine Bewertungen
- The Effect of A Training Program During Pregnancy On The Attitude and Intention of NulliparousDokument8 SeitenThe Effect of A Training Program During Pregnancy On The Attitude and Intention of NulliparousNoraNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- CHBP Progress NoteDokument1 SeiteCHBP Progress NoteNelson R. PouNoch keine Bewertungen
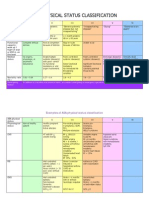
- ASADokument3 SeitenASAMelisa Malik50% (2)
- AntepartalDokument27 SeitenAntepartalaliehso100% (1)
- Pre EclampsiaDokument2 SeitenPre EclampsiaDIVINA VINCEE PRESTONoch keine Bewertungen
- Effect of Kenikir (Cosmos Caudatus) On Malondialdehyde (MDA) and Blood Pressure When Hypertension in Pregnancy A Systematic ReviewDokument14 SeitenEffect of Kenikir (Cosmos Caudatus) On Malondialdehyde (MDA) and Blood Pressure When Hypertension in Pregnancy A Systematic ReviewInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- OB OSCE ReviewerDokument5 SeitenOB OSCE ReviewerPao Ali100% (1)
- Obstetrics and GynecologyDokument4 SeitenObstetrics and Gynecologychuppepay100% (3)
- No. 33. Diagnosis and Management of Preeclampsia and EclampsiaDokument9 SeitenNo. 33. Diagnosis and Management of Preeclampsia and EclampsiaRomi RanutaNoch keine Bewertungen
- 2010 Updated Management Protocol in Selected Obstetric Topics MOH, EthiopiaDokument228 Seiten2010 Updated Management Protocol in Selected Obstetric Topics MOH, EthiopiaAhmedNoch keine Bewertungen
- NP 12345 EyyyyDokument133 SeitenNP 12345 EyyyySjerwin Anthony Gianan100% (2)
- HELLP Syndrome and Preeclampsia in Patient With Neurofibromatosis Type 1 - Case ReportDokument5 SeitenHELLP Syndrome and Preeclampsia in Patient With Neurofibromatosis Type 1 - Case ReportSabrina JonesNoch keine Bewertungen
- Drugs Used in The Management of Pre-EclampsiaDokument11 SeitenDrugs Used in The Management of Pre-EclampsiaVenance NtengoNoch keine Bewertungen
- Machine Learning Approach For Pre-Eclampsia Risk Factors AssociationDokument6 SeitenMachine Learning Approach For Pre-Eclampsia Risk Factors AssociationBiBiana PinToNoch keine Bewertungen
- LESSON PLAN On Preeclampsia BGCCDokument11 SeitenLESSON PLAN On Preeclampsia BGCCjrkedridgemwanakalandoNoch keine Bewertungen
- Preeclampsia:: What You Need To KnowDokument2 SeitenPreeclampsia:: What You Need To KnowRhod Vincent Jamolod TayongNoch keine Bewertungen
- Journal 1Dokument4 SeitenJournal 1Kristoff CamposNoch keine Bewertungen
- SOMANZ - Hypertension Pregnancy Guideeline April 2014Dokument51 SeitenSOMANZ - Hypertension Pregnancy Guideeline April 2014Amanda Mustika AdiNoch keine Bewertungen
- ACOG SMFM Joint Practice Bulletin Multiple Gestation 2004Dokument15 SeitenACOG SMFM Joint Practice Bulletin Multiple Gestation 2004Reza ZulkarnainNoch keine Bewertungen
- Effect of Magnesium Sulfate On Oxytocin-Induced Contractility inDokument10 SeitenEffect of Magnesium Sulfate On Oxytocin-Induced Contractility injoelruizmaNoch keine Bewertungen
- Nuhra Region7 AgendaDokument59 SeitenNuhra Region7 AgendaEuna Patricia AguilarNoch keine Bewertungen
- Case Report Hellp SyndromeDokument21 SeitenCase Report Hellp Syndromearebe29Noch keine Bewertungen
- DR Khaled Final Exam MCQ 2012 - 2013Dokument89 SeitenDR Khaled Final Exam MCQ 2012 - 2013ﻣﻠﻚ عيسى100% (2)
- High Risk Pregnancy Review QuestionsDokument59 SeitenHigh Risk Pregnancy Review Questionsmitted100% (1)
- Multichoice MidwiferyDokument8 SeitenMultichoice MidwiferyEvanNoch keine Bewertungen
- Acog Practice Bulletin Summary: Gestational Hypertension and PreeclampsiaDokument4 SeitenAcog Practice Bulletin Summary: Gestational Hypertension and PreeclampsiaAji PatriajatiNoch keine Bewertungen
- Immunological Tolerance, Pregnancy, and Preeclampsia: The Roles of Semen Microbes and The FatherDokument39 SeitenImmunological Tolerance, Pregnancy, and Preeclampsia: The Roles of Semen Microbes and The FatherAnanda Yuliastri DewiNoch keine Bewertungen
- H. Hypertensive Disorders in PregnancyDokument50 SeitenH. Hypertensive Disorders in PregnancyRadha ChiombonNoch keine Bewertungen
- Douglas A. Woelkers, MD Associate Professor of Reproductive Medicine University of California, San DiegoDokument36 SeitenDouglas A. Woelkers, MD Associate Professor of Reproductive Medicine University of California, San DiegoongkisawooNoch keine Bewertungen
- Exercise in PregnancyDokument7 SeitenExercise in PregnancynirchennNoch keine Bewertungen
- Nursing Role and Nursing Care During Pregnancy ComplicationsDokument21 SeitenNursing Role and Nursing Care During Pregnancy Complicationsvienny kayeNoch keine Bewertungen