Das könnte Ihnen auch gefallen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Minute Math 2Dokument112 SeitenMinute Math 2Lidia Dicu100% (3)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Diagnosing Borderline Personality DisorderDokument12 SeitenDiagnosing Borderline Personality DisorderAnonymous 0uCHZz72vwNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Power BI For Data ModellingDokument25 SeitenPower BI For Data ModellingJunior Leite100% (1)
- Marana Karaka SthanaDokument20 SeitenMarana Karaka SthanaKamal RanathungaNoch keine Bewertungen
- Model Curriculum Vitae and Resume For Law Student GraduatesDokument2 SeitenModel Curriculum Vitae and Resume For Law Student GraduatesSnehal SinghNoch keine Bewertungen
- Testing MechanicalDokument42 SeitenTesting MechanicalSadique ChakoleNoch keine Bewertungen
- University of The CordillerasDokument2 SeitenUniversity of The Cordillerasmj Canilang100% (1)
- ISO 30401 MandateDokument4 SeitenISO 30401 MandateTheerapan CNoch keine Bewertungen
- Frequencies: StatisticsDokument5 SeitenFrequencies: StatisticsEzza RiezaNoch keine Bewertungen
- Perbandingan Mutu Dan Harga Tablet Amoksisilin 500 MG Generik Dengan Non Generik Yang Beredar Di PasaranDokument16 SeitenPerbandingan Mutu Dan Harga Tablet Amoksisilin 500 MG Generik Dengan Non Generik Yang Beredar Di Pasarantzennopharma7828Noch keine Bewertungen
- Australian Dental Journal: The Contemporary Management of Third MolarsDokument8 SeitenAustralian Dental Journal: The Contemporary Management of Third MolarsEzza RiezaNoch keine Bewertungen
- The Effect of Various Classes of Malocclusions On The Maxillary Arch Forms and Dimensions in Jordanian PopulationDokument7 SeitenThe Effect of Various Classes of Malocclusions On The Maxillary Arch Forms and Dimensions in Jordanian PopulationEzza RiezaNoch keine Bewertungen
- Daftar PustakaDokument2 SeitenDaftar PustakaEzza RiezaNoch keine Bewertungen
- Nasakah PublikasiDokument11 SeitenNasakah PublikasiEzza RiezaNoch keine Bewertungen
- Dog Training Book Rex in The CityDokument56 SeitenDog Training Book Rex in The CitybebekbuluhNoch keine Bewertungen
- InTech-Diagnostic Imaging in Oral and Maxillofacial PathologyDokument25 SeitenInTech-Diagnostic Imaging in Oral and Maxillofacial PathologyDian Primadia PutriNoch keine Bewertungen
- Test KtiDokument1 SeiteTest KtiEzza RiezaNoch keine Bewertungen
- Lembaran Rekap PedodonsiaDokument1 SeiteLembaran Rekap PedodonsiaEzza RiezaNoch keine Bewertungen
- 167Dokument9 Seiten167real_septiady_madrid3532Noch keine Bewertungen
- Maybelline Co - IdDokument2 SeitenMaybelline Co - IdEzza RiezaNoch keine Bewertungen
- Pyogenic Granuloma of Gingiva: A MisnomerDokument4 SeitenPyogenic Granuloma of Gingiva: A MisnomerInternational Organization of Scientific Research (IOSR)Noch keine Bewertungen
- KUISIONERDokument9 SeitenKUISIONERRini Ajah RNoch keine Bewertungen
- Oral and Maxillofacial Surgery and Procedures 003Dokument4 SeitenOral and Maxillofacial Surgery and Procedures 003Ezza RiezaNoch keine Bewertungen
- Oral and Maxillofacial Surgery and Procedures 003Dokument4 SeitenOral and Maxillofacial Surgery and Procedures 003Ezza RiezaNoch keine Bewertungen
- 07 PDFDokument7 Seiten07 PDFEzza RiezaNoch keine Bewertungen
- 7 130p D PDFDokument108 Seiten7 130p D PDFEzza RiezaNoch keine Bewertungen
- Gingival Epulis CaseDokument5 SeitenGingival Epulis Casejinny1_0Noch keine Bewertungen
- Oral and Maxillofacial Surgery Syllabus 01.PDF 30538196Dokument117 SeitenOral and Maxillofacial Surgery Syllabus 01.PDF 30538196Ezza RiezaNoch keine Bewertungen
- Gingival Epulis CaseDokument5 SeitenGingival Epulis Casejinny1_0Noch keine Bewertungen
- 2212 4403Dokument18 Seiten2212 4403Ezza RiezaNoch keine Bewertungen
- 1-The Etiology of Orthodontic ProblemsDokument47 Seiten1-The Etiology of Orthodontic ProblemsEzza RiezaNoch keine Bewertungen
- Gingival Epulis CaseDokument5 SeitenGingival Epulis Casejinny1_0Noch keine Bewertungen
- Research Article: Effectiveness of Mouth Washes On Streptococci in Plaque Around Orthodontic AppliancesDokument5 SeitenResearch Article: Effectiveness of Mouth Washes On Streptococci in Plaque Around Orthodontic AppliancesEzza RiezaNoch keine Bewertungen
- Ameloblastoma: A Clinical Review and Trends in ManagementDokument13 SeitenAmeloblastoma: A Clinical Review and Trends in ManagementEzza RiezaNoch keine Bewertungen
- Gingival Epulis CaseDokument5 SeitenGingival Epulis Casejinny1_0Noch keine Bewertungen
- Kista Odontogenik Di Rumah Sakit Dr. Wahidin Sudirohusodo MakassarDokument8 SeitenKista Odontogenik Di Rumah Sakit Dr. Wahidin Sudirohusodo MakassarEzza RiezaNoch keine Bewertungen
- 15 Angle ClassificationDokument33 Seiten15 Angle ClassificationEzza RiezaNoch keine Bewertungen
- Ich GuidelinesDokument5 SeitenIch GuidelinesdrdeeptisharmaNoch keine Bewertungen
- ExampleApp Functional SpecificationDokument119 SeitenExampleApp Functional SpecificationmilosvarakNoch keine Bewertungen
- Final SPKDokument9 SeitenFinal SPKAinul qalbiNoch keine Bewertungen
- Knowledge Intensive Business Services (KIBS) : Don Scott-Kemmis July 2006Dokument8 SeitenKnowledge Intensive Business Services (KIBS) : Don Scott-Kemmis July 2006KALAWANoch keine Bewertungen
- An Introduction To Genre Theory: January 1997Dokument16 SeitenAn Introduction To Genre Theory: January 1997pratolectusNoch keine Bewertungen
- IT MANAGER Job Description - Minconsult SDN BHDDokument4 SeitenIT MANAGER Job Description - Minconsult SDN BHDSivasakti MarimuthuNoch keine Bewertungen
- Basic ConceptsDokument96 SeitenBasic ConceptsMuthu KumarNoch keine Bewertungen
- Liverpool University Campus MapDokument2 SeitenLiverpool University Campus MapJohn LukNoch keine Bewertungen
- HIRARC - Yawar Hassan KhanDokument11 SeitenHIRARC - Yawar Hassan KhanCyberMissio StudiosNoch keine Bewertungen
- Recovering The Essence in Language - EssayDokument3 SeitenRecovering The Essence in Language - EssayOnel1Noch keine Bewertungen
- Castellated Beam: Cell Form: Ds 0.25 DsDokument2 SeitenCastellated Beam: Cell Form: Ds 0.25 DsعلياسماعيلNoch keine Bewertungen
- Studio D A1 WorkbookDokument4 SeitenStudio D A1 WorkbookZubyr Bhatty0% (1)
- 9990 Y18-20 Sy PDFDokument40 Seiten9990 Y18-20 Sy PDFmashalNoch keine Bewertungen
- Science Documentary 2016: The Math Mystery Mathematics in Nature and Universe. (A Reaction Paper)Dokument3 SeitenScience Documentary 2016: The Math Mystery Mathematics in Nature and Universe. (A Reaction Paper)Ms Tuesday WattpadNoch keine Bewertungen
- Art Intg Proj CL 6-10Dokument5 SeitenArt Intg Proj CL 6-10Sarthak JoshiNoch keine Bewertungen
- Empirical and Tchebysheff's TheoremDokument7 SeitenEmpirical and Tchebysheff's TheoremLee Yee RunNoch keine Bewertungen
- Many Worlds InterpretationDokument26 SeitenMany Worlds InterpretationahsbonNoch keine Bewertungen
- Oracle Linux 7 Update 5-E93593Dokument68 SeitenOracle Linux 7 Update 5-E93593Saad Ullah KhanNoch keine Bewertungen
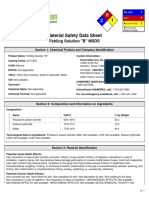
- Fehling Solution "B" MSDS: Section 1: Chemical Product and Company IdentificationDokument6 SeitenFehling Solution "B" MSDS: Section 1: Chemical Product and Company IdentificationAnnisaNoch keine Bewertungen
- 2023 Occ 1ST ExamDokument3 Seiten2023 Occ 1ST ExamSamantha LaboNoch keine Bewertungen
- Beyond GrammarDokument184 SeitenBeyond Grammaryazadn100% (2)
- The Historical & Evolutionary Theory of The Origin of StateDokument5 SeitenThe Historical & Evolutionary Theory of The Origin of StateMateen Ali100% (1)