Das könnte Ihnen auch gefallen
- Barral InstituteDokument32 SeitenBarral InstituteIoan-ovidiu Cordis100% (3)
- Pain Essay - What Are The Pathways Involved in The Sensation of Pain and How Can We Manipulate Them For Our BenefitDokument5 SeitenPain Essay - What Are The Pathways Involved in The Sensation of Pain and How Can We Manipulate Them For Our BenefitscholifyNoch keine Bewertungen
- Soil Seed FungiDokument506 SeitenSoil Seed FungiJanel Lucena86% (7)
- 4 Physiology Supplement Handout Based On Ganong For TOPNOTCH 21 by Jaffar PinedaDokument46 Seiten4 Physiology Supplement Handout Based On Ganong For TOPNOTCH 21 by Jaffar PinedaAthena Borja100% (3)
- Spinal Mechanisms of Pain and Analgesia: ReviewarticleDokument17 SeitenSpinal Mechanisms of Pain and Analgesia: ReviewarticleAblfazl KianiNoch keine Bewertungen
- Safety and Efficacy of Intrathecal Ziconotide in The Management of Severe Chronic PainDokument14 SeitenSafety and Efficacy of Intrathecal Ziconotide in The Management of Severe Chronic PainRodolfoMadNoch keine Bewertungen
- Claudia Stiles Library ProjectDokument3 SeitenClaudia Stiles Library ProjectClaudia StilesNoch keine Bewertungen
- Pain Molecular MechanismsDokument10 SeitenPain Molecular MechanismsEsteban OcampoNoch keine Bewertungen
- Pathophysiology of Pain: Neural Processing and ModulationDokument12 SeitenPathophysiology of Pain: Neural Processing and ModulationFirah Triple'sNoch keine Bewertungen
- Neuropathic PainDokument9 SeitenNeuropathic PainOki HarisandiNoch keine Bewertungen
- Essay 1 PainDokument3 SeitenEssay 1 PainDaniela PaceNoch keine Bewertungen
- Alpha-2 Adrenergic Receptor Agonists: A Review of Current Clinical ApplicationsDokument8 SeitenAlpha-2 Adrenergic Receptor Agonists: A Review of Current Clinical ApplicationsabdulNoch keine Bewertungen
- The Role of Adrenergic Receptors and Pain: The Good, The Bad, and The UnknownDokument5 SeitenThe Role of Adrenergic Receptors and Pain: The Good, The Bad, and The Unknowndrjully29Noch keine Bewertungen
- Pharmacology of The Equine Foot Medical Pain Management For Laminitis 2021Dokument13 SeitenPharmacology of The Equine Foot Medical Pain Management For Laminitis 2021guadialvarezNoch keine Bewertungen
- EFIC2015 Poster AbstractsDokument1.066 SeitenEFIC2015 Poster AbstractsszscribdNoch keine Bewertungen
- Drugs Acting On Nervous SystemDokument17 SeitenDrugs Acting On Nervous SystemAmina mNoch keine Bewertungen
- Molecular Approaches For Neuropathic Pain TreatmentDokument6 SeitenMolecular Approaches For Neuropathic Pain Treatmentmatheus derocoNoch keine Bewertungen
- A Central Mechanism of Analgesia in Mice and Humans Lacking The Sodium Channel Na 1.7: An AnalysisDokument30 SeitenA Central Mechanism of Analgesia in Mice and Humans Lacking The Sodium Channel Na 1.7: An AnalysissargamcNoch keine Bewertungen
- Central Neuronal Mechanisms in Cancer-Induced Bone Pain: Richard M. Gordon-Williams and Anthony H. DickensonDokument5 SeitenCentral Neuronal Mechanisms in Cancer-Induced Bone Pain: Richard M. Gordon-Williams and Anthony H. DickensonPham Thanh MinhNoch keine Bewertungen
- Alternatives To Opioid Analgesia in Small Animal Anesthesia, Alpha-2 Agonist 2019Dokument15 SeitenAlternatives To Opioid Analgesia in Small Animal Anesthesia, Alpha-2 Agonist 2019Carolina Duque RodriguezNoch keine Bewertungen
- Pain MechanismsDokument6 SeitenPain Mechanismsrr48843Noch keine Bewertungen
- PHARM Yoshimura LocalAnesthetics PDFDokument32 SeitenPHARM Yoshimura LocalAnesthetics PDFDhaif dhaifNoch keine Bewertungen
- Fisiopatología Del DolorDokument29 SeitenFisiopatología Del DolorHÉCTOR MIGUEL ESTRADA BOLAÑOSNoch keine Bewertungen
- Chemotherapy Induced Peripheral Neuropathy Risk ... 2010Dokument9 SeitenChemotherapy Induced Peripheral Neuropathy Risk ... 2010gemita aldeaNoch keine Bewertungen
- An Introduction To The Endocannabinoid SystemDokument5 SeitenAn Introduction To The Endocannabinoid Systemjoseba_pavia6405Noch keine Bewertungen
- Ef®cacy of Intravenous Magnesium in Neuropathic Pain: S. Brill, P. M. Sedgwick, W. Hamann and P. P. Di VadiDokument4 SeitenEf®cacy of Intravenous Magnesium in Neuropathic Pain: S. Brill, P. M. Sedgwick, W. Hamann and P. P. Di VadiVandhy P. Andi LoloNoch keine Bewertungen
- Basicanatomyand Physiologyofpain Pathways: Sarah Bourne,, Andre G. Machado,, Sean J. NagelDokument10 SeitenBasicanatomyand Physiologyofpain Pathways: Sarah Bourne,, Andre G. Machado,, Sean J. NagelarlinieNoch keine Bewertungen
- Sci-Hub - Anatomía Básica y Fisiología de Las Vías Del Dolor - 10.1016:j.nec.2014.06Dokument10 SeitenSci-Hub - Anatomía Básica y Fisiología de Las Vías Del Dolor - 10.1016:j.nec.2014.06Lucero DiazNoch keine Bewertungen
- Introduction To CNS PharmacologyDokument49 SeitenIntroduction To CNS Pharmacologymatchees-gone rogueNoch keine Bewertungen
- Descending Facilitation From The Brainstem Determines Behavioural and Neuronal Hypersensitivity Following Nerve Injury and e Cacy of PregabalinDokument15 SeitenDescending Facilitation From The Brainstem Determines Behavioural and Neuronal Hypersensitivity Following Nerve Injury and e Cacy of PregabalinmagreaNoch keine Bewertungen
- Essay 2 PainDokument2 SeitenEssay 2 PainDaniela PaceNoch keine Bewertungen
- Ion Channel NociceptorDokument13 SeitenIon Channel NociceptorarmeiliaNoch keine Bewertungen
- Pain Research: Product Guide - Edition 1Dokument36 SeitenPain Research: Product Guide - Edition 1D. GiffordNoch keine Bewertungen
- Peripheral Mechanisms of Opioid Analgesia: Christoph Stein and Leonie Julia LangDokument6 SeitenPeripheral Mechanisms of Opioid Analgesia: Christoph Stein and Leonie Julia LangLidiaNoch keine Bewertungen
- 14Dokument10 Seiten14Juliana ObandoNoch keine Bewertungen
- Molecular Mechanisms of Action of Systemic Lidocaine in Acute and Chronic PainDokument15 SeitenMolecular Mechanisms of Action of Systemic Lidocaine in Acute and Chronic PainAlfredo HuamaniNoch keine Bewertungen
- Mechanisms of Mechanical Allodynia ExplainedDokument13 SeitenMechanisms of Mechanical Allodynia Explainedaskar drNoch keine Bewertungen
- Adrenergic Agonists and ReceptorsDokument90 SeitenAdrenergic Agonists and ReceptorsOMAR NASSERNoch keine Bewertungen
- Vagus Nerve Stimulation Effects on Amygdala-Induced Epilepsy in RatsDokument11 SeitenVagus Nerve Stimulation Effects on Amygdala-Induced Epilepsy in RatsCecilia HarrisonNoch keine Bewertungen
- 415 2017 Article 8641Dokument8 Seiten415 2017 Article 8641Karel GuevaraNoch keine Bewertungen
- SC 2015225Dokument11 SeitenSC 2015225elbueno21Noch keine Bewertungen
- LO 18 Pain Pathways and Pharma MGT OADokument4 SeitenLO 18 Pain Pathways and Pharma MGT OAhbgossNoch keine Bewertungen
- Easy ANSDokument23 SeitenEasy ANSAmirAmeer AliNoch keine Bewertungen
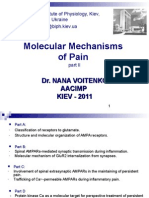
- Molecular Mechanisms of Pain: Dr. Nana Voitenko Aacimp KIEV - 2011Dokument39 SeitenMolecular Mechanisms of Pain: Dr. Nana Voitenko Aacimp KIEV - 2011Gilad NoyNoch keine Bewertungen
- Vardeh Pain - Medicine 2017Dokument3 SeitenVardeh Pain - Medicine 2017malakNoch keine Bewertungen
- Gate Control TheoryDokument33 SeitenGate Control TheorySarath KumarNoch keine Bewertungen
- Local Anesthetics SabinDokument69 SeitenLocal Anesthetics Sabinsabin7000Noch keine Bewertungen
- 2014 Calcium Channel Proteins Mediate Trigeminal Neuropathic Pain States Associated With Aberrant Excitatory SynaptogenesisDokument13 Seiten2014 Calcium Channel Proteins Mediate Trigeminal Neuropathic Pain States Associated With Aberrant Excitatory SynaptogenesisCristian OyarzoNoch keine Bewertungen
- UntitledDokument19 SeitenUntitledSarbjeet SinghNoch keine Bewertungen
- Chapter-2-pharmacologyDokument18 SeitenChapter-2-pharmacologynikhilkhatker2020Noch keine Bewertungen
- Cases For Review For CH 567-SignedDokument2 SeitenCases For Review For CH 567-SignedGhieGhie TPNoch keine Bewertungen
- Mechanical Allodynia: Invited ReviewDokument7 SeitenMechanical Allodynia: Invited ReviewFabiano VargasNoch keine Bewertungen
- Principios_de_la_EconomiaDokument39 SeitenPrincipios_de_la_EconomiajavierandreamoNoch keine Bewertungen
- Br. J. Anaesth.-2001-Kidd-3-11Dokument9 SeitenBr. J. Anaesth.-2001-Kidd-3-11Kevin MulyaNoch keine Bewertungen
- YlikontiolaDokument7 SeitenYlikontiolaodontologia uvNoch keine Bewertungen
- For Nasari 2012Dokument8 SeitenFor Nasari 2012basma adianaNoch keine Bewertungen
- Pain Revised-Book-2014Dokument167 SeitenPain Revised-Book-2014Maria AngelescuNoch keine Bewertungen
- Muscle Relaxants Anesthesia QuizDokument2 SeitenMuscle Relaxants Anesthesia QuizFabian LitetaNoch keine Bewertungen
- Reduction of Sporadic and Neurofibromatosis Type 2-Associated Vestibular Schwannoma Growth in Vitro and in Vivo After Treatment With The C-Jun N-Terminal Kinase Inhibitor AS602801Dokument10 SeitenReduction of Sporadic and Neurofibromatosis Type 2-Associated Vestibular Schwannoma Growth in Vitro and in Vivo After Treatment With The C-Jun N-Terminal Kinase Inhibitor AS602801NG keyNoch keine Bewertungen
- Attenuation of Early Phase Inflammation by Cannabidiol Prevents Pain and Nerve Damage in Rat Osteoarthritis. Philpott Et Al., 2017Dokument10 SeitenAttenuation of Early Phase Inflammation by Cannabidiol Prevents Pain and Nerve Damage in Rat Osteoarthritis. Philpott Et Al., 2017betoNoch keine Bewertungen
- Neuromuscular Blocking Agents GuideDokument1 SeiteNeuromuscular Blocking Agents GuideIbraheem SairiNoch keine Bewertungen
- CNS Regeneration: Basic Science and Clinical AdvancesVon EverandCNS Regeneration: Basic Science and Clinical AdvancesJeffrey KordowerNoch keine Bewertungen
- Central Actions of Angiotensin and Related HormonesVon EverandCentral Actions of Angiotensin and Related HormonesJoseph P. BuckleyNoch keine Bewertungen
- Strategies For Achieving High-Level Expression of Genes in Escherichia ColiDokument27 SeitenStrategies For Achieving High-Level Expression of Genes in Escherichia ColiRhinNoch keine Bewertungen
- Bio4eu StudyDokument149 SeitenBio4eu StudyRodolfoMadNoch keine Bewertungen
- Common Poisonous Plants and Mushrooms of North AmericaDokument326 SeitenCommon Poisonous Plants and Mushrooms of North AmericaRodolfoMadNoch keine Bewertungen
- HormonasDokument1 SeiteHormonasRodolfoMadNoch keine Bewertungen
- Guide For AuthorsDokument2 SeitenGuide For AuthorsRodolfoMadNoch keine Bewertungen
- Geral PDFDokument11 SeitenGeral PDFRodolfoMadNoch keine Bewertungen
- Geral PDFDokument11 SeitenGeral PDFRodolfoMadNoch keine Bewertungen
- Antip em Alga MarronDokument10 SeitenAntip em Alga MarronRodolfoMadNoch keine Bewertungen
- Geral 3Dokument9 SeitenGeral 3RodolfoMadNoch keine Bewertungen
- Plasticidade Das Celulas EstaminaisDokument3 SeitenPlasticidade Das Celulas EstaminaisRodolfoMadNoch keine Bewertungen
- Ral 2 PDFDokument18 SeitenRal 2 PDFRodolfoMadNoch keine Bewertungen
- Libro de Anatomia de Las Tortugas en InglesDokument180 SeitenLibro de Anatomia de Las Tortugas en InglesPaula PeñaNoch keine Bewertungen
- Artigo BioinformaticaDokument8 SeitenArtigo BioinformaticaRodolfoMadNoch keine Bewertungen
- Artigo BioinformaticaDokument8 SeitenArtigo BioinformaticaRodolfoMadNoch keine Bewertungen
- Diablo III Startup LogDokument32 SeitenDiablo III Startup LogRodolfoMadNoch keine Bewertungen
- Plasticidade Das Celulas EstaminaisDokument3 SeitenPlasticidade Das Celulas EstaminaisRodolfoMadNoch keine Bewertungen
- D3 DebugDokument52 SeitenD3 DebugRodolfoMadNoch keine Bewertungen
- D3 PrefsDokument1 SeiteD3 PrefsfreebookmanNoch keine Bewertungen
- Anti Bacterian ADokument6 SeitenAnti Bacterian ARodolfoMadNoch keine Bewertungen
- Células EstaminaisDokument8 SeitenCélulas EstaminaisRodolfoMadNoch keine Bewertungen
- Trilho Caminho Dos MortosDokument2 SeitenTrilho Caminho Dos MortosRodolfoMadNoch keine Bewertungen
- CulturaDokument7 SeitenCulturaRodolfoMadNoch keine Bewertungen
- Pattern and Sources of Naturally Produced OrganohalogensDokument12 SeitenPattern and Sources of Naturally Produced OrganohalogensRodolfoMadNoch keine Bewertungen
- 3.2. Biochemical Biomarkers in Algae and Marine PollutionDokument15 Seiten3.2. Biochemical Biomarkers in Algae and Marine Pollutionteddy_constantinNoch keine Bewertungen
- Do Vesicle Cells of The Red Alga Asparagopsis (Falkenbergia Stage) Play A Role in Bromocarbon ProductionDokument5 SeitenDo Vesicle Cells of The Red Alga Asparagopsis (Falkenbergia Stage) Play A Role in Bromocarbon ProductionRodolfoMadNoch keine Bewertungen
- Halogenated Metabolites With Antibacterial Activity From The Okinawan Laurencia SpeciesDokument7 SeitenHalogenated Metabolites With Antibacterial Activity From The Okinawan Laurencia SpeciesRodolfoMadNoch keine Bewertungen
- Machine Learning Module-3Dokument23 SeitenMachine Learning Module-3Samba Shiva Reddy.g ShivaNoch keine Bewertungen
- Fpga Implementation of Neural Networks: Main ContentsDokument21 SeitenFpga Implementation of Neural Networks: Main Contentsatef BenhaouesNoch keine Bewertungen
- Markscheme: May 2017 Biology Higher Level Paper 3Dokument22 SeitenMarkscheme: May 2017 Biology Higher Level Paper 3Xiang SizheNoch keine Bewertungen
- 1Dokument6 Seiten1Jude Matthew Diokno BernalNoch keine Bewertungen
- Reflective Essay On DeathDokument8 SeitenReflective Essay On Deathafibzfwdkaesyf100% (2)
- Myers AP 3e - Unit 3 - WatermarkDokument78 SeitenMyers AP 3e - Unit 3 - WatermarkRahaf AftanNoch keine Bewertungen
- Artificial Intelligence Chapter 20.5: Neural NetworksDokument84 SeitenArtificial Intelligence Chapter 20.5: Neural NetworksshardapatelNoch keine Bewertungen
- Paper PDFDokument376 SeitenPaper PDFIvan KraljevićNoch keine Bewertungen
- A Good Start in Life - Understanding Your Child's Brain and BehaviorDokument300 SeitenA Good Start in Life - Understanding Your Child's Brain and BehaviorSarah Emmanuel HaryonoNoch keine Bewertungen
- PerdevLesson10 BIOPSYCHOLOGYDokument27 SeitenPerdevLesson10 BIOPSYCHOLOGYDale DuclosNoch keine Bewertungen
- Pain Physiology Chapter Explains Nociception and HyperalgesiaDokument20 SeitenPain Physiology Chapter Explains Nociception and HyperalgesiaDiana TiganucNoch keine Bewertungen
- Neurons, Synapses, and Signaling: Lecture Presentations by Nicole Tunbridge and Kathleen FitzpatrickDokument102 SeitenNeurons, Synapses, and Signaling: Lecture Presentations by Nicole Tunbridge and Kathleen FitzpatrickSallyNoch keine Bewertungen
- General Education Post-TestDokument10 SeitenGeneral Education Post-TestNailah Andalinog100% (1)
- Biology Class X: Assignment No.4 Chapter 12: Coordination and ControlDokument2 SeitenBiology Class X: Assignment No.4 Chapter 12: Coordination and ControlAbdullah ButtNoch keine Bewertungen
- Neural Network Module 1Dokument76 SeitenNeural Network Module 14JK18CS031 Lavanya PushpakarNoch keine Bewertungen
- NEUROBIOLOGY OF LEARNING IN ADULTS AND DEVELOPMENTDokument20 SeitenNEUROBIOLOGY OF LEARNING IN ADULTS AND DEVELOPMENTbotoks uwuNoch keine Bewertungen
- Unit 7 Quizlet Test QuestionsDokument6 SeitenUnit 7 Quizlet Test QuestionsChristian CortnerNoch keine Bewertungen
- Nervous System WorksheetDokument8 SeitenNervous System WorksheetBeneNoch keine Bewertungen
- Neurocardiology: Anatomical and Functional PrinciplesDokument21 SeitenNeurocardiology: Anatomical and Functional PrinciplesLuis A Gil PantojaNoch keine Bewertungen
- Regeneracion Neuronal PDFDokument12 SeitenRegeneracion Neuronal PDFcumbredinNoch keine Bewertungen
- Muscle Physiology and NeurophysiologyDokument68 SeitenMuscle Physiology and NeurophysiologyAlan MagpantayNoch keine Bewertungen
- Chapter 9-Nervous SystemDokument2 SeitenChapter 9-Nervous SystemLynNoch keine Bewertungen
- 2 The BrainDokument21 Seiten2 The BrainLok YiuNoch keine Bewertungen
- Biopsychology: Ninth EditionDokument24 SeitenBiopsychology: Ninth EditionJasleen Kaur100% (1)
- PROJECT On Stress Management by Karan Pathak FinalDokument85 SeitenPROJECT On Stress Management by Karan Pathak FinalKaran pathakNoch keine Bewertungen
- Neural Signaling Med 1Dokument42 SeitenNeural Signaling Med 1sally.kh.mhNoch keine Bewertungen
- Nervous System Structure and FunctionDokument4 SeitenNervous System Structure and FunctionrohitNoch keine Bewertungen
- CH 10 Lecture PresentationDokument159 SeitenCH 10 Lecture PresentationBrian Mathieu Jr.Noch keine Bewertungen