Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Cardio WorkbookDokument5 SeitenCardio WorkbookZhy Caluza100% (1)
- CID-Treatment of Acinetobacter InfectionsDokument6 SeitenCID-Treatment of Acinetobacter InfectionsRizal PharmNoch keine Bewertungen
- CID-Treatment of Acinetobacter InfectionsDokument6 SeitenCID-Treatment of Acinetobacter InfectionsRizal PharmNoch keine Bewertungen
- Introduction To BiostatisticsDokument49 SeitenIntroduction To BiostatisticsRizal PharmNoch keine Bewertungen
- Introduction To BiostatisticsDokument49 SeitenIntroduction To BiostatisticsRizal PharmNoch keine Bewertungen
- Asthma Action Plan EnglishDokument7 SeitenAsthma Action Plan EnglishRizal PharmNoch keine Bewertungen
- B.SC Nursing - 2019 - 2 - Aug Sept - Pharmacology Pathology andDokument1 SeiteB.SC Nursing - 2019 - 2 - Aug Sept - Pharmacology Pathology andshubham vermaNoch keine Bewertungen
- THYROIDINIUMDokument13 SeitenTHYROIDINIUMUnnathi TNoch keine Bewertungen
- Pathological Tooth ResorptionDokument143 SeitenPathological Tooth ResorptionAnas KallayilNoch keine Bewertungen
- 1 Procedure Neurological Assessment (Cranial Nerves)Dokument7 Seiten1 Procedure Neurological Assessment (Cranial Nerves)Jonh Vincent DedoroNoch keine Bewertungen
- Chapter 4 - Water PollutionDokument44 SeitenChapter 4 - Water PollutionLuqman NHNoch keine Bewertungen
- The Language of AnatomyDokument7 SeitenThe Language of AnatomyLinziJaeOnelNoch keine Bewertungen
- Best Practice Guidelines - Wound Management Diabetic Foot UlcersDokument27 SeitenBest Practice Guidelines - Wound Management Diabetic Foot UlcersAndrada Catrinoiu100% (1)
- Learners With Chronic IllnessDokument22 SeitenLearners With Chronic IllnessERICAMILES BARRIENTOS0% (1)
- Trends in Intellectual Property RightsDokument22 SeitenTrends in Intellectual Property RightsHana HallajNoch keine Bewertungen
- Wa0002.Dokument7 SeitenWa0002.mustaphasuleiman124Noch keine Bewertungen
- Induction and Augmentation of LaborDokument20 SeitenInduction and Augmentation of Laborjssamc prasootitantraNoch keine Bewertungen
- Chapter 13 - Diseases of White Blood Cells, Lymph Nodes, Spleen, and ThymusDokument10 SeitenChapter 13 - Diseases of White Blood Cells, Lymph Nodes, Spleen, and ThymusAgnieszka WisniewskaNoch keine Bewertungen
- Digestive Symptoms in COVID-19 Patients With Mild Disease SeverityDokument13 SeitenDigestive Symptoms in COVID-19 Patients With Mild Disease SeveritytyariNoch keine Bewertungen
- Hip Exam - OSCE Stations PDFDokument2 SeitenHip Exam - OSCE Stations PDFEmiel AwadNoch keine Bewertungen
- Uddeholms Ab Safety Data Sheet: UDDEHOLM (BRUSH WELLMAN) Alloys: Moldmax®HH/LH and Weldpak®Dokument8 SeitenUddeholms Ab Safety Data Sheet: UDDEHOLM (BRUSH WELLMAN) Alloys: Moldmax®HH/LH and Weldpak®awesome_600Noch keine Bewertungen
- Hellp 2Dokument57 SeitenHellp 2Angela CaguitlaNoch keine Bewertungen
- Systemic Disease and Their Oral ManifestationsDokument80 SeitenSystemic Disease and Their Oral ManifestationsRakshya ShresthaNoch keine Bewertungen
- ANSDokument42 SeitenANSRakshan T100% (1)
- Managing Infectious Health Hazards and Diseases in The Construction Industry - SlidesDokument126 SeitenManaging Infectious Health Hazards and Diseases in The Construction Industry - SlidesHuzaifa SafdarNoch keine Bewertungen
- HODGES-Autism Spectrum Disorder Definition, Epidemiology, Causes, and Clinical EvaluationDokument11 SeitenHODGES-Autism Spectrum Disorder Definition, Epidemiology, Causes, and Clinical EvaluationwNoch keine Bewertungen
- Antibiotic Resistance and Evolution Case Study GR 11Dokument7 SeitenAntibiotic Resistance and Evolution Case Study GR 11Petro BricalliNoch keine Bewertungen
- Table of Benefits QLMDokument8 SeitenTable of Benefits QLMJuliyanto WibowoNoch keine Bewertungen
- Pro Animal Testing On Animals: Opening StatementsDokument3 SeitenPro Animal Testing On Animals: Opening StatementsShiela RengelNoch keine Bewertungen
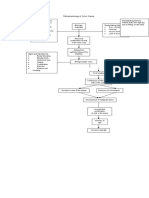
- Pathophysiology of Colon Cancer Predisposing Factors: Etiology: Precipitating Factors: Precipitating FactorsDokument1 SeitePathophysiology of Colon Cancer Predisposing Factors: Etiology: Precipitating Factors: Precipitating FactorstatiNoch keine Bewertungen
- Various CT Scan Score in Pneumonia and CovidDokument8 SeitenVarious CT Scan Score in Pneumonia and CovidrishaNoch keine Bewertungen
- Soal Ujian SekolahDokument47 SeitenSoal Ujian SekolahClemens JasonNoch keine Bewertungen
- ST English 8 No. 1Dokument4 SeitenST English 8 No. 1Roylyn Joy CarlosNoch keine Bewertungen
- (PHARMA A) 3.3 - Antibiotics I - Dr. Cruz (2024)Dokument15 Seiten(PHARMA A) 3.3 - Antibiotics I - Dr. Cruz (2024)Miguel Luis NavarreteNoch keine Bewertungen
- Angina Pectoris Pharmacological and Acupuncture TherapyDokument5 SeitenAngina Pectoris Pharmacological and Acupuncture TherapyEditor IJTSRDNoch keine Bewertungen