Das könnte Ihnen auch gefallen
- Pregnancy in A Didelphic Uterus - A Case ReportDokument7 SeitenPregnancy in A Didelphic Uterus - A Case ReportAmin BashyrNoch keine Bewertungen
- Case Conference NICHOLASDokument9 SeitenCase Conference NICHOLASagathapradanaNoch keine Bewertungen
- Bicornuate Uterus With Associated Bilateral Tubal Blockage and Fibroid TumorsDokument3 SeitenBicornuate Uterus With Associated Bilateral Tubal Blockage and Fibroid TumorsPutu AndreNoch keine Bewertungen
- Herlyn Werner WunderlichDokument3 SeitenHerlyn Werner WunderlichAgung SentosaNoch keine Bewertungen
- Successful Pregnancy Outcome in A Case of Bi-Cornuate Uterus With Boh With Secondary Infertility and GDM - A Very Rare Case Report - Medisun AcademyDokument4 SeitenSuccessful Pregnancy Outcome in A Case of Bi-Cornuate Uterus With Boh With Secondary Infertility and GDM - A Very Rare Case Report - Medisun AcademyGautom Kumar PaulNoch keine Bewertungen
- Minakshi S. Neglected Puerperal Inversion of The Uterus Ignorance Makes Acute A Chronic FormDokument4 SeitenMinakshi S. Neglected Puerperal Inversion of The Uterus Ignorance Makes Acute A Chronic FormJulius Albert SNoch keine Bewertungen
- Herlyn Werner Wundrlich Syndrome PDFDokument7 SeitenHerlyn Werner Wundrlich Syndrome PDFfitriamarizkaNoch keine Bewertungen
- Rupture Uterus in Pregnancy With Didelphys Uterus: A Rare Case ReportDokument3 SeitenRupture Uterus in Pregnancy With Didelphys Uterus: A Rare Case Reportanon_804324181Noch keine Bewertungen
- Hematometra in Uterus Didelphys With Right Hemivagina and Right Renal AgenesisDokument3 SeitenHematometra in Uterus Didelphys With Right Hemivagina and Right Renal AgenesisDexter BluesNoch keine Bewertungen
- Ectopic Pregnancy: Clinical PracticeDokument9 SeitenEctopic Pregnancy: Clinical PracticeNurul WulandariNoch keine Bewertungen
- General Gynaecology:, Leo Francis AquilizanDokument15 SeitenGeneral Gynaecology:, Leo Francis AquilizanesjayemNoch keine Bewertungen
- Van Wyk Grumbach Syndrome The Importance of Thyroi 2024 International JournDokument5 SeitenVan Wyk Grumbach Syndrome The Importance of Thyroi 2024 International JournRonald QuezadaNoch keine Bewertungen
- Ovarian Ectopic Pregnancy: A Rare Case: Iran J Reprod Med Vol. 12. No. 4. PP: 281-284, April 2014Dokument4 SeitenOvarian Ectopic Pregnancy: A Rare Case: Iran J Reprod Med Vol. 12. No. 4. PP: 281-284, April 2014alif bagusNoch keine Bewertungen
- AMasculine PresentingFemaleAdolescentaRareCaseofPoorly DifferentiatedSertoli LeydigCellTumorDokument15 SeitenAMasculine PresentingFemaleAdolescentaRareCaseofPoorly DifferentiatedSertoli LeydigCellTumorDaniella Ashley BaltesNoch keine Bewertungen
- A Rare Case of Ovarian Dysgerminoma in A 6Dokument5 SeitenA Rare Case of Ovarian Dysgerminoma in A 6sarinovitapratiwiNoch keine Bewertungen
- Chronic Ovarian Ectopic Pregnancy - An Unusual Occurrence: A Case ReportDokument5 SeitenChronic Ovarian Ectopic Pregnancy - An Unusual Occurrence: A Case Reportindex PubNoch keine Bewertungen
- Medicine: Intrauterine Device Found in An Ovarian TumorDokument5 SeitenMedicine: Intrauterine Device Found in An Ovarian TumorRezky amalia basirNoch keine Bewertungen
- Ovarian CystDokument4 SeitenOvarian CystGenio RachmadanaNoch keine Bewertungen
- Scar Ectopic Case ReportDokument6 SeitenScar Ectopic Case ReportMominah MayamNoch keine Bewertungen
- Laparoscopic Management of Rudimentary Uterine Horn Pregnancy: Case Report and Literature ReviewDokument4 SeitenLaparoscopic Management of Rudimentary Uterine Horn Pregnancy: Case Report and Literature ReviewCamacho OmarNoch keine Bewertungen
- Jurnal KEDokument16 SeitenJurnal KEMuhammad Harris ZainalNoch keine Bewertungen
- Rare Case of Partial Mole With Live Fetus Progression To Invasive Mole With Lung Metastasis Following Spontaneous ConceptionDokument3 SeitenRare Case of Partial Mole With Live Fetus Progression To Invasive Mole With Lung Metastasis Following Spontaneous ConceptionIJAR JOURNALNoch keine Bewertungen
- P15:Secondandthirdtrimestersi: S. Latella, V. Fenu, P. Ceccarelli, F. Baldinotti, L. Iughetti, A. Volpe, V. MazzaDokument2 SeitenP15:Secondandthirdtrimestersi: S. Latella, V. Fenu, P. Ceccarelli, F. Baldinotti, L. Iughetti, A. Volpe, V. MazzaXlr8zzNoch keine Bewertungen
- UC Irvine: Clinical Practice and Cases in Emergency MedicineDokument6 SeitenUC Irvine: Clinical Practice and Cases in Emergency MedicinePatrick NunsioNoch keine Bewertungen
- Endometrial Carcinoma in A 24-Year-Old: A Case Report and Systematic ReviewDokument5 SeitenEndometrial Carcinoma in A 24-Year-Old: A Case Report and Systematic ReviewIJAR JOURNALNoch keine Bewertungen
- Case Report: Postpartum Uterine Wound Dehiscence Leading To Secondary PPH: Unusual SequelaeDokument4 SeitenCase Report: Postpartum Uterine Wound Dehiscence Leading To Secondary PPH: Unusual SequelaemelisaberlianNoch keine Bewertungen
- Rare Case of Bicornuate Uterus With Fetal Death in A Multipara WomanDokument2 SeitenRare Case of Bicornuate Uterus With Fetal Death in A Multipara WomanInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- TOG Endometrial HyperplasiaDokument6 SeitenTOG Endometrial HyperplasiaNalin AbeysingheNoch keine Bewertungen
- Managment of Scar PregnancyDokument43 SeitenManagment of Scar Pregnancyvacha sardarNoch keine Bewertungen
- Uterine Rupture in Healthy Uterus Complication of Misoprostol (About Two Cases and Review of The Literature)Dokument3 SeitenUterine Rupture in Healthy Uterus Complication of Misoprostol (About Two Cases and Review of The Literature)International Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- Obstetrics and Gynecology ClinicsDokument247 SeitenObstetrics and Gynecology ClinicsAlexandr TrotskyNoch keine Bewertungen
- Ectopic Pregnancy: A ReviewDokument13 SeitenEctopic Pregnancy: A ReviewDinorah MarcelaNoch keine Bewertungen
- The Conservative Management of Early PreDokument11 SeitenThe Conservative Management of Early PreAnna JuniedNoch keine Bewertungen
- Uterine Rupture in Nulliparous Woman Without Risk Factors: A Case Report and Literature ReviewDokument6 SeitenUterine Rupture in Nulliparous Woman Without Risk Factors: A Case Report and Literature ReviewBOHR International Journal on GynaecologyNoch keine Bewertungen
- Uterine Leiomyoma in An Adolescent Female: Case ReportDokument3 SeitenUterine Leiomyoma in An Adolescent Female: Case Reportdr.putra888Noch keine Bewertungen
- Endometrial Adenocarcinoma and Polycystic Ovary Syndrome: Risk Factors, Management, and PrognosisDokument4 SeitenEndometrial Adenocarcinoma and Polycystic Ovary Syndrome: Risk Factors, Management, and PrognosisDikie MustofadijayaNoch keine Bewertungen
- Mucinous Adenocarcinoma FinalDokument16 SeitenMucinous Adenocarcinoma Finalritzy0997Noch keine Bewertungen
- Post Partum Maternal Morbidities and TheDokument102 SeitenPost Partum Maternal Morbidities and TheBagusHibridaNoch keine Bewertungen
- Cervical Dysgenesis With Transverse Vaginal Septum With Imperforate Hymen in An 11 Year Old Girl Presenting With Acute AbdomenDokument4 SeitenCervical Dysgenesis With Transverse Vaginal Septum With Imperforate Hymen in An 11 Year Old Girl Presenting With Acute Abdomenshe-docNoch keine Bewertungen
- Malignancies in Pregnancy Multiple 2016 Best Practice Research ClinicalDokument8 SeitenMalignancies in Pregnancy Multiple 2016 Best Practice Research ClinicalorriNoch keine Bewertungen
- Didelphys Uterus With Cervical Cancer What About Herlyn-Werner-Wunderlich Syndrome A Case Report and Review of Literature!Dokument3 SeitenDidelphys Uterus With Cervical Cancer What About Herlyn-Werner-Wunderlich Syndrome A Case Report and Review of Literature!International Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- Adnexal Mass in Pregnancy - UpToDateDokument22 SeitenAdnexal Mass in Pregnancy - UpToDateBhargav YagnikNoch keine Bewertungen
- Vesicular Mole: Dr. Mohammed Abdalla Egypt, Domiat G. HospitalDokument32 SeitenVesicular Mole: Dr. Mohammed Abdalla Egypt, Domiat G. Hospitalmadmax500Noch keine Bewertungen
- International Journal of Pharmaceutical Science Invention (IJPSI)Dokument3 SeitenInternational Journal of Pharmaceutical Science Invention (IJPSI)inventionjournalsNoch keine Bewertungen
- Abnormal Uterine BleedingDokument22 SeitenAbnormal Uterine BleedingAde JuandaNoch keine Bewertungen
- Twin Pregnancy With Complete Hydatidiform Mole andDokument3 SeitenTwin Pregnancy With Complete Hydatidiform Mole andGEAMH OBGYNNoch keine Bewertungen
- Ultrasound Scanning of Fetal AnomalyDokument19 SeitenUltrasound Scanning of Fetal AnomalyFA Khan0% (1)
- Total and Acute Uterine Inversion After Delivery A Case Report PDFDokument4 SeitenTotal and Acute Uterine Inversion After Delivery A Case Report PDFatika sgrtNoch keine Bewertungen
- 10.1515 - Med 2019 0098Dokument4 Seiten10.1515 - Med 2019 0098fansofiuNoch keine Bewertungen
- English Task Gynecology System: Case ReportDokument4 SeitenEnglish Task Gynecology System: Case ReportCecepNoch keine Bewertungen
- Review Adnexal Masses Pregnancy Rcog PDFDokument6 SeitenReview Adnexal Masses Pregnancy Rcog PDFRosália Coutada100% (1)
- Tinjauan Pustaka Agenesis UteriDokument2 SeitenTinjauan Pustaka Agenesis UteriMaulana DimasNoch keine Bewertungen
- Case Report Ghazanfar Page 130-132Dokument3 SeitenCase Report Ghazanfar Page 130-132sohailurologistNoch keine Bewertungen
- C-Obs 42 Management of Monochorionic Twins New Mar 11Dokument4 SeitenC-Obs 42 Management of Monochorionic Twins New Mar 11indra_strongNoch keine Bewertungen
- Anesthetic Management of An Undiagnosed Advanced Extrauterine Pregnancy Under Combined Spinal-Epidural AnesthesiaDokument4 SeitenAnesthetic Management of An Undiagnosed Advanced Extrauterine Pregnancy Under Combined Spinal-Epidural AnesthesiaHanayuki VizureiNoch keine Bewertungen
- Scar PregnancyDokument11 SeitenScar Pregnancyasshagab04Noch keine Bewertungen
- Uterine Inversion: A Life-Threatening Obstetric Emergency: Dawn R. Hostetler, MD, and Michael Bosworth, DODokument4 SeitenUterine Inversion: A Life-Threatening Obstetric Emergency: Dawn R. Hostetler, MD, and Michael Bosworth, DOAndi Farras WatyNoch keine Bewertungen
- EndometrisisDokument10 SeitenEndometrisisAmmarNoch keine Bewertungen
- Nejmoa1514762 PDFDokument12 SeitenNejmoa1514762 PDFDexter BluesNoch keine Bewertungen
- Ulkus Kornea Eng VerDokument15 SeitenUlkus Kornea Eng VerDexter BluesNoch keine Bewertungen
- Activation of mTOR: A Culprit of Alzheimer's Disease?: Neuropsychiatric Disease and Treatment DoveDokument16 SeitenActivation of mTOR: A Culprit of Alzheimer's Disease?: Neuropsychiatric Disease and Treatment Dovemr dexterNoch keine Bewertungen
- Benefits and Risks of Antiretroviral TherapyDokument12 SeitenBenefits and Risks of Antiretroviral TherapyAtgy Dhita AnggraeniNoch keine Bewertungen
- Pamj 24 182 PDFDokument5 SeitenPamj 24 182 PDFDexter BluesNoch keine Bewertungen
- PRM2016 1658172 PDFDokument7 SeitenPRM2016 1658172 PDFDexter BluesNoch keine Bewertungen
- SDJ 2016 09 01 PDFDokument7 SeitenSDJ 2016 09 01 PDFDexter BluesNoch keine Bewertungen
- Referat Obgyn FixDokument29 SeitenReferat Obgyn FixDexter BluesNoch keine Bewertungen
- Mood Dynamics in Bipolar Disorder: Research Open AccessDokument9 SeitenMood Dynamics in Bipolar Disorder: Research Open AccesswulanfarichahNoch keine Bewertungen
- Jurnal Anak RirinDokument10 SeitenJurnal Anak RirinDexter BluesNoch keine Bewertungen
- Jurnal Anak Ririn PDFDokument10 SeitenJurnal Anak Ririn PDFDexter BluesNoch keine Bewertungen
- Medi 96 E5795 PDFDokument5 SeitenMedi 96 E5795 PDFDexter BluesNoch keine Bewertungen
- Nejmoa1606356 PDFDokument10 SeitenNejmoa1606356 PDFDexter BluesNoch keine Bewertungen
- Childhood IQ and Bipolar Link PDFDokument9 SeitenChildhood IQ and Bipolar Link PDFDexter BluesNoch keine Bewertungen
- The Seven Cardinal MovementsDokument4 SeitenThe Seven Cardinal MovementsDexter BluesNoch keine Bewertungen
- QuestionsDokument1 SeiteQuestionsDexter BluesNoch keine Bewertungen
- The Seven Cardinal MovementsDokument4 SeitenThe Seven Cardinal MovementsDexter BluesNoch keine Bewertungen
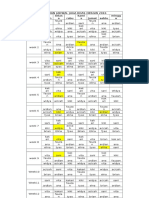
- Rincian Jadwal Jaga Koas Obsgin 2016 Senin Selas A Rabu Kami S Jumat Sabtu Mingg UDokument1 SeiteRincian Jadwal Jaga Koas Obsgin 2016 Senin Selas A Rabu Kami S Jumat Sabtu Mingg UDexter BluesNoch keine Bewertungen
- Fix ObgynDokument17 SeitenFix ObgynDexter BluesNoch keine Bewertungen
- The Seven Cardinal MovementsDokument3 SeitenThe Seven Cardinal MovementsMaria Mandid0% (1)
- 1830 PDF PDFDokument5 Seiten1830 PDF PDFDexter BluesNoch keine Bewertungen
- Referat Obgyn FixDokument29 SeitenReferat Obgyn FixDexter BluesNoch keine Bewertungen
- Childhood IQ and Bipolar Link PDFDokument9 SeitenChildhood IQ and Bipolar Link PDFDexter BluesNoch keine Bewertungen
- Jurnal Elderly 2 PDFDokument3 SeitenJurnal Elderly 2 PDFDexter BluesNoch keine Bewertungen
- Geriatric Itch PDFDokument16 SeitenGeriatric Itch PDFDexter BluesNoch keine Bewertungen
- Unchallengeable Miracles of QuranDokument430 SeitenUnchallengeable Miracles of QuranyoursincerefriendNoch keine Bewertungen
- Pruritus: An Updated Look at An Old ProblemDokument7 SeitenPruritus: An Updated Look at An Old ProblemThariq Mubaraq DrcNoch keine Bewertungen
- 10 4103@0378-6323 116725 PDFDokument14 Seiten10 4103@0378-6323 116725 PDFDexter BluesNoch keine Bewertungen
- Clinical Guidelines Acute Rehab Management 2010 InteractiveDokument172 SeitenClinical Guidelines Acute Rehab Management 2010 InteractivenathanaelandryNoch keine Bewertungen
- TSWJ2015 803752 PDFDokument8 SeitenTSWJ2015 803752 PDFDexter BluesNoch keine Bewertungen
- HR Policy ManualDokument34 SeitenHR Policy Manualshamna AbdullaNoch keine Bewertungen
- 10 Jurnal Tentang Judul Penerapan Nafas Dalam Post Op Apendisitis Sulhan Wira DutaDokument98 Seiten10 Jurnal Tentang Judul Penerapan Nafas Dalam Post Op Apendisitis Sulhan Wira DutaSultan Wira DutaNoch keine Bewertungen
- Jurnal 4Dokument5 SeitenJurnal 4Nindita RahmaNoch keine Bewertungen
- DC Kit2 ObadiaDokument2 SeitenDC Kit2 ObadiaErnesto KangNoch keine Bewertungen
- Spinal InjuryDokument24 SeitenSpinal InjuryFuad Ahmad ArdiansyahNoch keine Bewertungen
- Chapter 43 - Thrombocytopenia and ThrombocytosisDokument6 SeitenChapter 43 - Thrombocytopenia and ThrombocytosisNathaniel SimNoch keine Bewertungen
- Nuclear Imaging: Nama: Novita Rifanti Sustianingrum Nama Legiun: RadiologyDokument4 SeitenNuclear Imaging: Nama: Novita Rifanti Sustianingrum Nama Legiun: RadiologyAz Az AzNoch keine Bewertungen
- Cerebral Palsy Brain Paralysis: Complications of Neurodevelopmental DisordersDokument11 SeitenCerebral Palsy Brain Paralysis: Complications of Neurodevelopmental DisordersmikayNoch keine Bewertungen
- Extrapyramidal System DisordersDokument41 SeitenExtrapyramidal System DisordersAyshe SlocumNoch keine Bewertungen
- The Clinical Significance of The Retromolar Canal and Foramen in DentistryDokument24 SeitenThe Clinical Significance of The Retromolar Canal and Foramen in Dentistryمحمد عبدالرحمنNoch keine Bewertungen
- Learning Logs 2Dokument9 SeitenLearning Logs 2api-240988800Noch keine Bewertungen
- Short Increment Sensitivity Index Test (SISI)Dokument2 SeitenShort Increment Sensitivity Index Test (SISI)Anish RajNoch keine Bewertungen
- Cyclamen: Chilly PulsatillaDokument10 SeitenCyclamen: Chilly Pulsatillaअनुरूपम स्वामीNoch keine Bewertungen
- M1 All ProgramsDokument26 SeitenM1 All ProgramsDaisy Joy MBardz100% (1)
- Management of Traumatic Liver Injuries: DR Junaid Ahmad SofiDokument80 SeitenManagement of Traumatic Liver Injuries: DR Junaid Ahmad SofiNatalindah Jokiem Woecandra T. D.Noch keine Bewertungen
- Helicobacter PyloriDokument251 SeitenHelicobacter PyloriLuminita HutanuNoch keine Bewertungen
- Topic 9.2 Graded QuizDokument8 SeitenTopic 9.2 Graded QuizTran WinnerNoch keine Bewertungen
- 2023 Projects Microbiology-Hons-BookletDokument56 Seiten2023 Projects Microbiology-Hons-Bookletchand198Noch keine Bewertungen
- Ma. Lammatao: Trion AKG Marble LLCDokument11 SeitenMa. Lammatao: Trion AKG Marble LLCNasir AhmedNoch keine Bewertungen
- DrowningDokument22 SeitenDrowningNovie GarillosNoch keine Bewertungen
- Sc-Cal Plus Msds 3.0Dokument8 SeitenSc-Cal Plus Msds 3.0dbNoch keine Bewertungen
- Hypertrophic ScarsDokument13 SeitenHypertrophic ScarsNovita NingtyasNoch keine Bewertungen
- Fauci Dossier Valentine S Day Document 2022 (1) SummaryDokument5 SeitenFauci Dossier Valentine S Day Document 2022 (1) SummarySherri StreightNoch keine Bewertungen
- Immobilization and Death of Bacteria by Flora Seal Microbial SealantDokument6 SeitenImmobilization and Death of Bacteria by Flora Seal Microbial SealantinventionjournalsNoch keine Bewertungen
- DC2020-0067 ICD-10 Code For COVID-19 (Previously Known As 2019-nCoV) (02-12-20)Dokument1 SeiteDC2020-0067 ICD-10 Code For COVID-19 (Previously Known As 2019-nCoV) (02-12-20)Leah Rose Figueroa ParasNoch keine Bewertungen
- CKD Pocket GuideDokument2 SeitenCKD Pocket GuideLutfi MalefoNoch keine Bewertungen
- Sex Education Prevents Teen PregnancyDokument2 SeitenSex Education Prevents Teen PregnancyLeila Margrethe TrivilegioNoch keine Bewertungen
- Cataract Case PresentationDokument7 SeitenCataract Case PresentationShahbaz AAnsariNoch keine Bewertungen
- Obstetrics by Ten Teachers, 20th Edition 2017Dokument33 SeitenObstetrics by Ten Teachers, 20th Edition 2017salah subbah100% (1)
- Five"EFFICACY OF GANDHARVAHASTADI KASHAYAM IN THE MANAGEMENT OF ESSENTIAL HYPERTENSION (UCCHA - RAKTHACHAAPA)Dokument12 SeitenFive"EFFICACY OF GANDHARVAHASTADI KASHAYAM IN THE MANAGEMENT OF ESSENTIAL HYPERTENSION (UCCHA - RAKTHACHAAPA)Pradeep SambandamNoch keine Bewertungen