Das könnte Ihnen auch gefallen
- Determonacion Del Segmento Anterio Por OctDokument10 SeitenDetermonacion Del Segmento Anterio Por OctFelipe AlarcónNoch keine Bewertungen
- Olsen 2012Dokument7 SeitenOlsen 2012Camila GuerraNoch keine Bewertungen
- 1112CRSTEuro Cs VinciguerraDokument3 Seiten1112CRSTEuro Cs VinciguerraR Andres Plaza ZNoch keine Bewertungen
- Anterior Chamber Angle Assessment Techniques: Claudio Campa, Luisa Pierro, Paolo Bettin and Francesco BandelloDokument21 SeitenAnterior Chamber Angle Assessment Techniques: Claudio Campa, Luisa Pierro, Paolo Bettin and Francesco BandelloJovan Z. PopovićNoch keine Bewertungen
- Anterior Chamber Angle Imaging With Optical Coherence TomographyDokument7 SeitenAnterior Chamber Angle Imaging With Optical Coherence TomographySouvik BanerjeeNoch keine Bewertungen
- Sirius ZHeidariMMohammadpourDokument82 SeitenSirius ZHeidariMMohammadpourSyamerra YapNoch keine Bewertungen
- Comparison Between Femtosecond Laser Mushroom Con Figuration and Manual Trephine Straight-Edge Con Figuration Deep Anterior Lamellar KeratoplastyDokument6 SeitenComparison Between Femtosecond Laser Mushroom Con Figuration and Manual Trephine Straight-Edge Con Figuration Deep Anterior Lamellar KeratoplastyindahdeshakaNoch keine Bewertungen
- AncdDokument7 SeitenAncdNurulia RizkiNoch keine Bewertungen
- Increased Iris Thickness and Association With Primary Angle Closure GlaucomaDokument6 SeitenIncreased Iris Thickness and Association With Primary Angle Closure GlaucomaNinda AstariNoch keine Bewertungen
- Anterior Segment OctDokument53 SeitenAnterior Segment OctA.c. RaghuNoch keine Bewertungen
- Intraindividual Comparison of Aspherical and Spherical Intraocular Lenses of Same Material and PlatformDokument6 SeitenIntraindividual Comparison of Aspherical and Spherical Intraocular Lenses of Same Material and PlatformAkhilesh KumarNoch keine Bewertungen
- Wa0000Dokument7 SeitenWa0000Ocha24 TupamahuNoch keine Bewertungen
- Comparative Axial Length Measurements Using Optical and Acoustic Biometry in Normal Persons and in Patients With Retinal LesionsDokument5 SeitenComparative Axial Length Measurements Using Optical and Acoustic Biometry in Normal Persons and in Patients With Retinal LesionsAyu Wedhani SpcNoch keine Bewertungen
- Fundamentals of Oral and Maxillofacial RadiologyVon EverandFundamentals of Oral and Maxillofacial RadiologyBewertung: 4 von 5 Sternen4/5 (1)
- Journal of Vocational Health (: 02 (2019) : 134-139 Was Obtained 11 Aprill 2020Dokument2 SeitenJournal of Vocational Health (: 02 (2019) : 134-139 Was Obtained 11 Aprill 2020Ananta IpoNoch keine Bewertungen
- Macular Hole Size As A Prognostic Factor in Macular Hole SurgeryDokument5 SeitenMacular Hole Size As A Prognostic Factor in Macular Hole SurgeryArni ZulsitaNoch keine Bewertungen
- Comparison Between Digital and Manual Marking For Toric Intraocular LensesDokument4 SeitenComparison Between Digital and Manual Marking For Toric Intraocular LensesRaúl Plasencia SaliniNoch keine Bewertungen
- Anterior Chamber Angle Assessment Technique - CH 17Dokument20 SeitenAnterior Chamber Angle Assessment Technique - CH 17riveliNoch keine Bewertungen
- The Ocular Biometric and Corneal Topographic Characteristics of High-Anisometropic Adults in TaiwanDokument6 SeitenThe Ocular Biometric and Corneal Topographic Characteristics of High-Anisometropic Adults in TaiwanNurul Falah KalokoNoch keine Bewertungen
- Comparison of Corneal Biomechanical Properties Among AxialDokument8 SeitenComparison of Corneal Biomechanical Properties Among AxialPutri kartiniNoch keine Bewertungen
- Catarct SinilisDokument5 SeitenCatarct SinilisAsri Mukti NantaNoch keine Bewertungen
- Coscarelli, 2012Dokument8 SeitenCoscarelli, 2012vitor auzierNoch keine Bewertungen
- Ecop 09 00286Dokument11 SeitenEcop 09 00286GabrielNoch keine Bewertungen
- 1233 2373 1 SMDokument6 Seiten1233 2373 1 SMellaNoch keine Bewertungen
- Clinical Study: Comparison of The Optical Quality Between Small Incision Lenticule Extraction and Femtosecond Laser LASIKDokument10 SeitenClinical Study: Comparison of The Optical Quality Between Small Incision Lenticule Extraction and Femtosecond Laser LASIKnicoNoch keine Bewertungen
- Salmon 2003Dokument9 SeitenSalmon 2003Andrea GilNoch keine Bewertungen
- HHS Public AccessDokument12 SeitenHHS Public Accessnisa_kartikaNoch keine Bewertungen
- BiometryDokument7 SeitenBiometrysandip shelakeNoch keine Bewertungen
- Effect of Corneal Asphericity and Spherical Aberration On Intraocular Lens Power CalculationsDokument2 SeitenEffect of Corneal Asphericity and Spherical Aberration On Intraocular Lens Power Calculationsr2201cNoch keine Bewertungen
- Opd - Scan Ii PDFDokument6 SeitenOpd - Scan Ii PDFDfhos Oftalmo ServiceNoch keine Bewertungen
- Focal Structure-Function Relationships in Primary Open-Angle Glaucoma Using OCT and OCT-A MeasurementsDokument10 SeitenFocal Structure-Function Relationships in Primary Open-Angle Glaucoma Using OCT and OCT-A MeasurementsAlejandro LondoñoNoch keine Bewertungen
- Jur 1Dokument11 SeitenJur 1Dewi Puspita SariNoch keine Bewertungen
- Accuracy of Two Devices and Three Different Calculation Methods For Predicting Residual Astigmatism After Intraocular Lens ImplantationDokument5 SeitenAccuracy of Two Devices and Three Different Calculation Methods For Predicting Residual Astigmatism After Intraocular Lens Implantationjorefe12Noch keine Bewertungen
- Thesis Topics in Ophthalmology in AiimsDokument5 SeitenThesis Topics in Ophthalmology in AiimsBuyCollegePaperOnlineUK100% (1)
- A Review On Different Glaucoma Detection PDFDokument6 SeitenA Review On Different Glaucoma Detection PDFgiribabukandeNoch keine Bewertungen
- Feng Et Al 2023 Epithelial Thickness Mapping in Keratoconic Corneas Repeatability and Agreement Between Cso Ms 39Dokument14 SeitenFeng Et Al 2023 Epithelial Thickness Mapping in Keratoconic Corneas Repeatability and Agreement Between Cso Ms 39vahidsmpNoch keine Bewertungen
- A Deep Learning System For Automatic Assessment of Anterior Chamber Angle in Ultrasound Biomicroscopy ImagesDokument11 SeitenA Deep Learning System For Automatic Assessment of Anterior Chamber Angle in Ultrasound Biomicroscopy Imageszj xiaoNoch keine Bewertungen
- Femto Vs Phaco 2Dokument6 SeitenFemto Vs Phaco 2Bonita AsyigahNoch keine Bewertungen
- Kjo 32 172Dokument10 SeitenKjo 32 172Nurul Dwi LestariNoch keine Bewertungen
- Corneal Parameters Measurement in Healthy Subjects Using Scheimpflug and Anterior Segment Optical Coherence TomographyDokument6 SeitenCorneal Parameters Measurement in Healthy Subjects Using Scheimpflug and Anterior Segment Optical Coherence TomographyvahidsmpNoch keine Bewertungen
- Ijaret: ©iaemeDokument6 SeitenIjaret: ©iaemeIAEME PublicationNoch keine Bewertungen
- Scleral Thickness Manuscript CT-JC-review SKG 31102022Dokument25 SeitenScleral Thickness Manuscript CT-JC-review SKG 31102022Divya DarshiniNoch keine Bewertungen
- Lenstar IOLmasterDokument6 SeitenLenstar IOLmasterWillRoseroNoch keine Bewertungen
- Oftalmologi 2Dokument3 SeitenOftalmologi 2Jericho JeruzalemNoch keine Bewertungen
- Protocol ACDDokument8 SeitenProtocol ACDmariamzlaptopNoch keine Bewertungen
- IolDokument7 SeitenIolAnonymous h0DxuJTNoch keine Bewertungen
- Rajiv Gandhi University of Health Sciences, Karnataka, BangaloreDokument9 SeitenRajiv Gandhi University of Health Sciences, Karnataka, BangaloreAhmed Febri Hertama 'Sinosuke'Noch keine Bewertungen
- 1 s2.0 S0002939421006279 MainDokument7 Seiten1 s2.0 S0002939421006279 MainskocabzzNoch keine Bewertungen
- PterygiumDokument6 SeitenPterygiumDewiakyuNoch keine Bewertungen
- Assesment of Entrance Skin Doses For Patients - Abdullah Medical CityDokument4 SeitenAssesment of Entrance Skin Doses For Patients - Abdullah Medical CityGeorgiana KokonaNoch keine Bewertungen
- The Precision of The Panoramic Mandibular Index: ResearchDokument5 SeitenThe Precision of The Panoramic Mandibular Index: Research13eeeNoch keine Bewertungen
- 2016 Article 229Dokument7 Seiten2016 Article 229nisa_kartikaNoch keine Bewertungen
- A Cross-Sectional Study of Artifacts in Cone Beam Computed Tomography Images of Patients in A HospitalDokument4 SeitenA Cross-Sectional Study of Artifacts in Cone Beam Computed Tomography Images of Patients in A HospitalIJAR JOURNALNoch keine Bewertungen
- In-Plane Ultrasonic Needle Tracking Using A Fiber-Optic HydrophoneDokument9 SeitenIn-Plane Ultrasonic Needle Tracking Using A Fiber-Optic Hydrophonetaehyun KimNoch keine Bewertungen
- Accuracy of Working Length Measurement Electronic Apex Locator Versus Cone-Beam Computed TomographyDokument11 SeitenAccuracy of Working Length Measurement Electronic Apex Locator Versus Cone-Beam Computed Tomographygabrielatorres12Noch keine Bewertungen
- 2 EAL CompDokument6 Seiten2 EAL CompSoumya AbrahamNoch keine Bewertungen
- Long Term Follow-Up Safety and E Myopia Refractive Surgery: Ffectiveness ofDokument9 SeitenLong Term Follow-Up Safety and E Myopia Refractive Surgery: Ffectiveness ofayurNoch keine Bewertungen
- Anterior Chamber Depth Measurement in Pseudophakic Eyes A Comparison of Pentacam and UltrasoundDokument8 SeitenAnterior Chamber Depth Measurement in Pseudophakic Eyes A Comparison of Pentacam and UltrasoundWillRoseroNoch keine Bewertungen
- Body Mass Index and Interocular Asymmetry of Retinal and Choroidal Thickness in Emmetropic and Ametropic SubjectsDokument13 SeitenBody Mass Index and Interocular Asymmetry of Retinal and Choroidal Thickness in Emmetropic and Ametropic SubjectsAthenaeum Scientific PublishersNoch keine Bewertungen
- Diagnostic Ability of Retinal Ganglion Cell Complex, RetinalDokument7 SeitenDiagnostic Ability of Retinal Ganglion Cell Complex, RetinalYoselin Herrera GuzmánNoch keine Bewertungen
- Bowling FM CombinedDokument10 SeitenBowling FM CombinedRika FitriaNoch keine Bewertungen
- Publication PDFDokument44 SeitenPublication PDFRika FitriaNoch keine Bewertungen
- MRI Diffusion-Weighted Imaging in Intracranial Hemorrhage (ICH)Dokument10 SeitenMRI Diffusion-Weighted Imaging in Intracranial Hemorrhage (ICH)Rika FitriaNoch keine Bewertungen
- CER32 SleepApnea FinalReview 201108Dokument494 SeitenCER32 SleepApnea FinalReview 201108Rika FitriaNoch keine Bewertungen
- 459 FullDokument7 Seiten459 FullRika FitriaNoch keine Bewertungen
- jgrd50150 PDF Jsessionid f01t02Dokument21 Seitenjgrd50150 PDF Jsessionid f01t02suraj.atmos458Noch keine Bewertungen
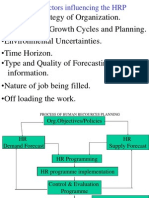
- HRPDokument35 SeitenHRPShree ....Noch keine Bewertungen
- Soil 5 15 2019 PDFDokument18 SeitenSoil 5 15 2019 PDFAnimisetti narayanaNoch keine Bewertungen
- Research Paper On Human Capital DevelopmentDokument6 SeitenResearch Paper On Human Capital Developmentvagipelez1z2100% (1)
- ch10 Acceptance Sampling PDFDokument29 Seitench10 Acceptance Sampling PDFgtmani123Noch keine Bewertungen
- EseuDokument13 SeitenEseuMadalinaNoch keine Bewertungen
- Identifying The Inquiry and Stating The ProblemDokument36 SeitenIdentifying The Inquiry and Stating The ProblemKenneth L. MaqueNoch keine Bewertungen
- Chapter 1-3Dokument15 SeitenChapter 1-3Ryan Balacanao BautistaNoch keine Bewertungen
- Report On RMG Industry Bangladesh - Economic PerspectiveDokument87 SeitenReport On RMG Industry Bangladesh - Economic PerspectiveRuhin Afrin Joyee100% (1)
- Mba Thesis DownloadDokument7 SeitenMba Thesis Downloadjuliegonzalezpaterson100% (1)
- What Is The Sign Test?: Step 1Dokument10 SeitenWhat Is The Sign Test?: Step 1Erica Andrea CacaoNoch keine Bewertungen
- Ashton Brennecke CV 2019Dokument3 SeitenAshton Brennecke CV 2019api-456822679Noch keine Bewertungen
- Mathematics Analysis and Approaches (HL) Extended Essay: TOPIC:-ProbabilityDokument55 SeitenMathematics Analysis and Approaches (HL) Extended Essay: TOPIC:-ProbabilityAnupransh SharmaNoch keine Bewertungen
- Career ManagementDokument23 SeitenCareer ManagementKritika SinghNoch keine Bewertungen
- Recruitment & Selection Process in Textile Sector With Reference To Coimbatore DistrictDokument5 SeitenRecruitment & Selection Process in Textile Sector With Reference To Coimbatore DistrictMaryamNoch keine Bewertungen
- Strategic ManagementDokument103 SeitenStrategic ManagementMayur KrishnaNoch keine Bewertungen
- 197detection and Quantification of Disease in Cabbage Using Clustering and RGB Colour Features PDFDokument7 Seiten197detection and Quantification of Disease in Cabbage Using Clustering and RGB Colour Features PDFGovindNoch keine Bewertungen
- TilesDokument58 SeitenTilesRicky KhannaNoch keine Bewertungen
- FDA Guidance StandardDokument40 SeitenFDA Guidance Standardajitbasrur445Noch keine Bewertungen
- 4 SOP GTE Profile (Package S) - Title & Name (2022)Dokument8 Seiten4 SOP GTE Profile (Package S) - Title & Name (2022)Anupriya RoyNoch keine Bewertungen
- BUS 511-Midterm-Test - 1-SampleQuestionsDokument3 SeitenBUS 511-Midterm-Test - 1-SampleQuestionshod.mechengineerNoch keine Bewertungen
- Null and Alternative Hypothesis Null Hypothesis DefinitionDokument34 SeitenNull and Alternative Hypothesis Null Hypothesis Definition04 Shaina SachdevaNoch keine Bewertungen
- Saccos and Youth DevelopmentDokument29 SeitenSaccos and Youth DevelopmentGgayi Joseph0% (1)
- Chapter 4Dokument12 SeitenChapter 4AYNETU TEREFENoch keine Bewertungen
- Dr. K. ReddyDokument14 SeitenDr. K. ReddyUpendra SinghNoch keine Bewertungen
- Guide To NIRDokument24 SeitenGuide To NIRtvijayak4150% (2)
- Efektivitas Strategi Komunikasi Pemasaran Sosial Kampanye Sustainable Seafood, Wwf-IndonesiaDokument10 SeitenEfektivitas Strategi Komunikasi Pemasaran Sosial Kampanye Sustainable Seafood, Wwf-IndonesiaEva LianNoch keine Bewertungen
- Writing A Recommendation in A Research Paper ExampleDokument8 SeitenWriting A Recommendation in A Research Paper Examplenydohavihup2Noch keine Bewertungen
- Tuv Sud Lifts and EscalatorsDokument2 SeitenTuv Sud Lifts and EscalatorsJazonNoch keine Bewertungen
- Sociology 16th Edition Macionis Solutions Manual 1Dokument15 SeitenSociology 16th Edition Macionis Solutions Manual 1ricky100% (58)