Das könnte Ihnen auch gefallen
- 4 - ClinicalDokument11 Seiten4 - Clinicalapi-464332286100% (1)
- Functional Limitations Checklist PDFDokument53 SeitenFunctional Limitations Checklist PDFBarney Livingstone50% (2)
- Apothecary, Household and Metric Systems of MeasurementDokument4 SeitenApothecary, Household and Metric Systems of MeasurementMANLANGIT, Bianca Trish A.100% (1)
- The Heart Manual: Post Myocardial Infarction (Post MI) EditionDokument18 SeitenThe Heart Manual: Post Myocardial Infarction (Post MI) EditionPablo L RodriguezNoch keine Bewertungen
- 6 Minute Walk Test InstructionsDokument6 Seiten6 Minute Walk Test InstructionscpradheepNoch keine Bewertungen
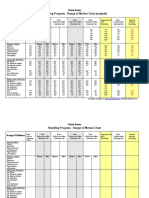
- Standing Program - Range of Motion Chart (Sample) : Client NameDokument2 SeitenStanding Program - Range of Motion Chart (Sample) : Client NameNorMan Albaytar PerezNoch keine Bewertungen
- Physical Therapy DocumentationDokument5 SeitenPhysical Therapy DocumentationdjdkNoch keine Bewertungen
- Urinalysis Result Form Combur 10Dokument2 SeitenUrinalysis Result Form Combur 10Hyde Lee Bin HaoNoch keine Bewertungen
- Physical Assessment Write-UpDokument10 SeitenPhysical Assessment Write-UpkathypinzonNoch keine Bewertungen
- Exercise to Prevent and Manage Chronic Disease Across the LifespanVon EverandExercise to Prevent and Manage Chronic Disease Across the LifespanNoch keine Bewertungen
- Cinahl Rotator Cuff InjuriesDokument11 SeitenCinahl Rotator Cuff InjurieslizardbeeNoch keine Bewertungen
- Home Exercise ProgramDokument6 SeitenHome Exercise ProgramRavin NarwalNoch keine Bewertungen
- نسخة Lecture - PAIN Assessment & ManagementDokument52 Seitenنسخة Lecture - PAIN Assessment & Managementjsoal100% (1)
- Rehabilitation of Patients After StrokeDokument47 SeitenRehabilitation of Patients After StrokeRogerNoch keine Bewertungen
- Myocardial Infarction (MI)Dokument29 SeitenMyocardial Infarction (MI)ناصر دويكاتNoch keine Bewertungen
- Sci RehabDokument45 SeitenSci RehabkaushikawebNoch keine Bewertungen
- Physical Agents: Therapeutic ModalitiesDokument31 SeitenPhysical Agents: Therapeutic Modalitiessinanhadeed100% (1)
- Occupational Therapy Now Volume 14.5Dokument32 SeitenOccupational Therapy Now Volume 14.5Sara Gomes CastroNoch keine Bewertungen
- DM PhysioDokument24 SeitenDM Physiodwi astutiNoch keine Bewertungen
- SLR Ventilator Weaning Education PresentationDokument48 SeitenSLR Ventilator Weaning Education Presentationfallenczar100% (1)
- Lung Transplant PathwayDokument39 SeitenLung Transplant PathwayMohana Preethi MNoch keine Bewertungen
- Lec 3 Definition of PhysioDokument18 SeitenLec 3 Definition of PhysioBhargav100% (1)
- Psoriatic ArthritisDokument12 SeitenPsoriatic ArthritisSelvia RosadiNoch keine Bewertungen
- Medication Administration TimesDokument3 SeitenMedication Administration TimesBenjel AndayaNoch keine Bewertungen
- Medical Emergencies in Rehabilitation MedicineDokument24 SeitenMedical Emergencies in Rehabilitation MedicineAzza El Awar100% (1)
- Geriatric RehabilitationDokument10 SeitenGeriatric RehabilitationJuanitoCabatañaLimIIINoch keine Bewertungen
- Respiratory Rate and Breathing Pattern: Clinical ReviewDokument3 SeitenRespiratory Rate and Breathing Pattern: Clinical ReviewMochamad BilalNoch keine Bewertungen
- Geriatrics Sir ZahidDokument575 SeitenGeriatrics Sir ZahidSheeraz ShahzadNoch keine Bewertungen
- Pain Management in The Elderly Population 2010 PDFDokument9 SeitenPain Management in The Elderly Population 2010 PDFDara Agusti MaulidyaNoch keine Bewertungen
- Traumatic Brain Injury (Tbi)Dokument11 SeitenTraumatic Brain Injury (Tbi)api-267971269Noch keine Bewertungen
- B. Occupational Therapy (Hons.) : Faculty of Health Sciences Universiti Teknologi MaraDokument3 SeitenB. Occupational Therapy (Hons.) : Faculty of Health Sciences Universiti Teknologi MaraSiti Nur Hafidzoh OmarNoch keine Bewertungen
- A Guide For People With C1-C3 Spinal Cord InjuryDokument23 SeitenA Guide For People With C1-C3 Spinal Cord InjuryivanchanNoch keine Bewertungen
- OT8 - Thumb Immobilization SplintDokument4 SeitenOT8 - Thumb Immobilization SplintAnnbe Barte100% (1)
- Splinting InstructionsDokument19 SeitenSplinting Instructionsiris_madrigal100% (1)
- Development Chart For BookletDokument13 SeitenDevelopment Chart For BookletzapelNoch keine Bewertungen
- Role of OT in End of Life CareDokument13 SeitenRole of OT in End of Life Carekori holubNoch keine Bewertungen
- Muscular System DisordersDokument36 SeitenMuscular System DisordersShawn Henry CepedaNoch keine Bewertungen
- 5 6323480972671058006Dokument195 Seiten5 6323480972671058006Anonymous QOCn5dNoch keine Bewertungen
- Glassgow Coma Scale and Rancho Los AmigosDokument17 SeitenGlassgow Coma Scale and Rancho Los AmigosHEMA CHANDRANNoch keine Bewertungen
- Lumbar Laminectomy Diskectomy Fusion PDFDokument3 SeitenLumbar Laminectomy Diskectomy Fusion PDFRully SyahrizalNoch keine Bewertungen
- Safe Patient Handling - Sitting Up and TransferringDokument12 SeitenSafe Patient Handling - Sitting Up and TransferringgrazeyjvNoch keine Bewertungen
- Pulmonary Rehabilitation ExercisesDokument28 SeitenPulmonary Rehabilitation ExercisesAdrian AlzNoch keine Bewertungen
- Whiplash Injury Recovery Booklet - 2nd Edition PDFDokument21 SeitenWhiplash Injury Recovery Booklet - 2nd Edition PDFshivani04Noch keine Bewertungen
- Front Matter - 2020 - Guccione S Geriatric Physical Therapy PDFDokument1 SeiteFront Matter - 2020 - Guccione S Geriatric Physical Therapy PDFGamalia MartaNoch keine Bewertungen
- Depression in Older AdultsDokument22 SeitenDepression in Older AdultsDr. Shanojan Thiyagalingam, FRCPC FACPNoch keine Bewertungen
- Part 2: Social Skills Training: RatingDokument3 SeitenPart 2: Social Skills Training: RatingGina GucioNoch keine Bewertungen
- Therapeutic Modalities: Chapter 6 or 7Dokument32 SeitenTherapeutic Modalities: Chapter 6 or 7Ajay Pal NattNoch keine Bewertungen
- Oedojo Soedirham) : Department of Health Promotion and Behavioral SciencesDokument59 SeitenOedojo Soedirham) : Department of Health Promotion and Behavioral SciencesAshri Nur IstiqomahNoch keine Bewertungen
- GCS Assessment - Information SheetDokument4 SeitenGCS Assessment - Information SheetVeronica TanuwijayaNoch keine Bewertungen
- ApproachDokument37 SeitenApproachAshu AshNoch keine Bewertungen
- Pedia1 NewbornDokument300 SeitenPedia1 NewbornNacel CelesteNoch keine Bewertungen
- Orthopedic Manual Therapy Chadcook3rdPTMASUDDokument30 SeitenOrthopedic Manual Therapy Chadcook3rdPTMASUDHisham Al ShamiNoch keine Bewertungen
- Occupational Therapy Activities For AdultsDokument3 SeitenOccupational Therapy Activities For AdultsEllee HadesNoch keine Bewertungen
- Physical Agent ModalitiesDokument13 SeitenPhysical Agent ModalitiesLeonardo MustopoNoch keine Bewertungen
- An 8 Week Scapular Stabilization Exercise Program in An Elite Archer With Scapular Dyskinesis Presenting Joint Noise A Case Report With One YearDokument8 SeitenAn 8 Week Scapular Stabilization Exercise Program in An Elite Archer With Scapular Dyskinesis Presenting Joint Noise A Case Report With One YearAmbrogio Orsini100% (1)
- Strategies Used by Occupational Therapy To Maximize ADL IndependenceDokument53 SeitenStrategies Used by Occupational Therapy To Maximize ADL IndependenceNizam lotfiNoch keine Bewertungen
- SCI Acute Care and Rehabilitation PT 2009Dokument265 SeitenSCI Acute Care and Rehabilitation PT 2009api-3822828Noch keine Bewertungen
- Traumatic Brain InjuryDokument50 SeitenTraumatic Brain InjurySiesta CatsNoch keine Bewertungen
- Immobilization Protocol For Extensor Tendon RepairDokument2 SeitenImmobilization Protocol For Extensor Tendon RepairFatin NawarahNoch keine Bewertungen
- Autogenic DrainageDokument6 SeitenAutogenic DrainagePhooi Yee LauNoch keine Bewertungen
- Rehabilitation of Lower Limb AmputeeDokument53 SeitenRehabilitation of Lower Limb AmputeeMohamoud Mohamed100% (2)
- Who Wants To Be A Millionaire? MaterialsDokument61 SeitenWho Wants To Be A Millionaire? MaterialsShivaniNoch keine Bewertungen
- Refelctivejournalpart1Dokument3 SeitenRefelctivejournalpart1ShivaniNoch keine Bewertungen
- Cognitive Teaching ModelsDokument26 SeitenCognitive Teaching ModelsShivaniNoch keine Bewertungen
- Assessment of Breathlessness Clinical Pathway Assessment HandoutDokument8 SeitenAssessment of Breathlessness Clinical Pathway Assessment HandoutShivaniNoch keine Bewertungen
- Disaster ManagmentDokument75 SeitenDisaster ManagmentShivani100% (2)
- A Detailed Lesson Plan in Living ThingsDokument23 SeitenA Detailed Lesson Plan in Living ThingsclarisseNoch keine Bewertungen
- Effect On Oral NAC in COPDDokument5 SeitenEffect On Oral NAC in COPDMeiyanti MeiyantiNoch keine Bewertungen
- Pneumothorax (Collapsed Lung) : What Is A Pneumothorax?Dokument17 SeitenPneumothorax (Collapsed Lung) : What Is A Pneumothorax?Hazel EstayanNoch keine Bewertungen
- Clinical CoachDokument374 SeitenClinical CoachGensai KawakamiNoch keine Bewertungen
- Practice Exam in Nursing Set ADokument38 SeitenPractice Exam in Nursing Set AGo IdeasNoch keine Bewertungen
- Pulmonary EmbolismDokument4 SeitenPulmonary Embolismemmag1221100% (1)
- Acefyl SPP - 03 Dec 2010Dokument54 SeitenAcefyl SPP - 03 Dec 2010maliakbar111Noch keine Bewertungen
- Medical Surgical Nursing QuestionsDokument7 SeitenMedical Surgical Nursing Questionseloisa mae gementizaNoch keine Bewertungen
- 5 Patient Assessment Skills To Crush The TMC-RRT ExamDokument4 Seiten5 Patient Assessment Skills To Crush The TMC-RRT ExamNaser Abdulfatah Al Hazmi100% (1)
- Oxygen Therapy: From Wikipedia, The Free EncyclopediaDokument11 SeitenOxygen Therapy: From Wikipedia, The Free EncyclopediaDadi ArdiansyahNoch keine Bewertungen
- Nurs FPX 4050 Assessment 1 Preliminary Care Coordination PlanDokument4 SeitenNurs FPX 4050 Assessment 1 Preliminary Care Coordination PlanEmma Watson100% (1)
- NSTP ReviewerDokument13 SeitenNSTP ReviewerPamela Isabelle April EncenzoNoch keine Bewertungen
- WellBeing 169 - 2017 AU PDFDokument156 SeitenWellBeing 169 - 2017 AU PDFchiguazoNoch keine Bewertungen
- Thoracic SurgeryDokument33 SeitenThoracic SurgeryTed Cipriano VistaNoch keine Bewertungen
- Signs and Symptoms of Respiratory DiseasesDokument42 SeitenSigns and Symptoms of Respiratory DiseasesjabeedNoch keine Bewertungen
- 380 Case Study CDokument11 Seiten380 Case Study Capi-639359658Noch keine Bewertungen
- Monoclonal Cocktail-The Game Changer: DR - Kannan Nair Consultant-Er Sreechand Hospital, KannurDokument18 SeitenMonoclonal Cocktail-The Game Changer: DR - Kannan Nair Consultant-Er Sreechand Hospital, KannurKannan NairNoch keine Bewertungen
- A. Any ST-segment Elevation Greater Than or Equal To 1 MMDokument35 SeitenA. Any ST-segment Elevation Greater Than or Equal To 1 MMmashe1Noch keine Bewertungen
- Reaction Paper ChemDokument2 SeitenReaction Paper ChemAlexis Dela Cruz RoguelNoch keine Bewertungen
- Pico JurnalDokument3 SeitenPico JurnalMarinaNoch keine Bewertungen
- Respiratory ExaminationDokument59 SeitenRespiratory ExaminationNur Hamizah Md FuziNoch keine Bewertungen
- Respiratory Passmedicine 2020Dokument555 SeitenRespiratory Passmedicine 2020Vikrant100% (2)
- Oxygenation NCM 103Dokument10 SeitenOxygenation NCM 103Marti GregorioNoch keine Bewertungen
- Teaching Slide Set 2020: Global Initiative For Chronic Obstructive Lung Disease (Gold)Dokument53 SeitenTeaching Slide Set 2020: Global Initiative For Chronic Obstructive Lung Disease (Gold)MirsalinaNoch keine Bewertungen
- LECTURE RadPatho Complete 1Dokument69 SeitenLECTURE RadPatho Complete 1Soleil SierraNoch keine Bewertungen
- Lecture 4, 5 - Drugs Used in Bronchial Asthma & COPDDokument57 SeitenLecture 4, 5 - Drugs Used in Bronchial Asthma & COPDBalakrishnan Thangaraj100% (1)
- Wbi15 01 Que 20230117Dokument36 SeitenWbi15 01 Que 20230117grengtaNoch keine Bewertungen
- Emphysema NCPDokument5 SeitenEmphysema NCPAbegail Bautista DoriaNoch keine Bewertungen