Das könnte Ihnen auch gefallen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Sample of Psychological ReportDokument4 SeitenSample of Psychological ReportRochelle Joyce Olmilla Bersamin67% (3)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Sex ManualDokument14 SeitenSex ManualCally LiueNoch keine Bewertungen
- Scalar Wave Morphogenetic Field Mechanic PDFDokument135 SeitenScalar Wave Morphogenetic Field Mechanic PDFMokhtar Mohd100% (7)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Physical Assessment SampleDokument6 SeitenPhysical Assessment Samplecarlylove33% (3)
- Contact DermatitisDokument70 SeitenContact DermatitisThariq Mubaraq DrcNoch keine Bewertungen
- MycetomaDokument26 SeitenMycetomaTummalapalli Venkateswara RaoNoch keine Bewertungen
- Brain DeathDokument24 SeitenBrain DeathKawaljit KaurNoch keine Bewertungen
- Douleur Neuropathique 4 Questions (Dn4) Neuropathic Pain Diagnostic QuestionnaireDokument1 SeiteDouleur Neuropathique 4 Questions (Dn4) Neuropathic Pain Diagnostic QuestionnaireKrisnawati Intan SuwignyoNoch keine Bewertungen
- Douleur Neuropathique 4 Questions (Dn4) Neuropathic Pain Diagnostic QuestionnaireDokument1 SeiteDouleur Neuropathique 4 Questions (Dn4) Neuropathic Pain Diagnostic QuestionnaireKrisnawati Intan SuwignyoNoch keine Bewertungen
- Douleur Neuropathique 4 Questions (Dn4) Neuropathic Pain Diagnostic QuestionnaireDokument1 SeiteDouleur Neuropathique 4 Questions (Dn4) Neuropathic Pain Diagnostic QuestionnaireKrisnawati Intan SuwignyoNoch keine Bewertungen
- Douleur Neuropathique 4 Questions (Dn4) Neuropathic Pain Diagnostic QuestionnaireDokument1 SeiteDouleur Neuropathique 4 Questions (Dn4) Neuropathic Pain Diagnostic QuestionnaireKrisnawati Intan SuwignyoNoch keine Bewertungen
- Douleur Neuropathique 4 Questions (Dn4) Neuropathic Pain Diagnostic QuestionnaireDokument1 SeiteDouleur Neuropathique 4 Questions (Dn4) Neuropathic Pain Diagnostic QuestionnaireKrisnawati Intan SuwignyoNoch keine Bewertungen
- Sieff D.F. 2017 Trauma Worlds and The Wisdom of Marion Woodman AuthorsDokument18 SeitenSieff D.F. 2017 Trauma Worlds and The Wisdom of Marion Woodman AuthorsMelissa Viana100% (1)
- Precautionary and Sanitary Practices in Handling FoodDokument31 SeitenPrecautionary and Sanitary Practices in Handling FoodBrenNan ChannelNoch keine Bewertungen
- Coliform Analysis in Wastewater 2012Dokument24 SeitenColiform Analysis in Wastewater 2012engrbvgNoch keine Bewertungen
- Menstrual DisordersDokument45 SeitenMenstrual DisordersMegat Mohd Azman Adzmi100% (1)
- BLS CPRDokument42 SeitenBLS CPRKhairunisa SiregarNoch keine Bewertungen
- Mapping Obgyn 26feb 2017Dokument10 SeitenMapping Obgyn 26feb 2017Thariq Mubaraq DrcNoch keine Bewertungen
- Abses Serebri2 PDFDokument22 SeitenAbses Serebri2 PDFRagillia Irena FebriNoch keine Bewertungen
- Drco 2ndDokument371 SeitenDrco 2ndThariq Mubaraq DrcNoch keine Bewertungen
- 00 Diabetic Retinopathy Medical StudentsDokument7 Seiten00 Diabetic Retinopathy Medical StudentsBrigita De VegaNoch keine Bewertungen
- 00 Diabetic Retinopathy Medical StudentsDokument7 Seiten00 Diabetic Retinopathy Medical StudentsBrigita De VegaNoch keine Bewertungen
- 00 Diabetic Retinopathy Medical StudentsDokument7 Seiten00 Diabetic Retinopathy Medical StudentsBrigita De VegaNoch keine Bewertungen
- Drco 2ndDokument371 SeitenDrco 2ndThariq Mubaraq DrcNoch keine Bewertungen
- Koning SanderDokument111 SeitenKoning SanderThariq Mubaraq DrcNoch keine Bewertungen
- Khan 2009Dokument5 SeitenKhan 2009Thariq Mubaraq DrcNoch keine Bewertungen
- Wjo 5 65Dokument7 SeitenWjo 5 65Thariq Mubaraq DrcNoch keine Bewertungen
- TNM Staging For H&NDokument30 SeitenTNM Staging For H&NkiwiamoghNoch keine Bewertungen
- ABO Group For NPC 1Dokument5 SeitenABO Group For NPC 1Thariq Mubaraq DrcNoch keine Bewertungen
- Brach y TherapyDokument6 SeitenBrach y TherapyThariq Mubaraq DrcNoch keine Bewertungen
- Indonesian WhoqolDokument5 SeitenIndonesian WhoqolSri Nindita RuslanNoch keine Bewertungen
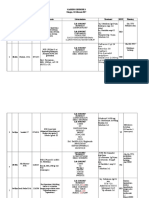
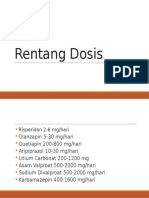
- Rentang Dosis New-Dr. Syahrial, SP - KJDokument2 SeitenRentang Dosis New-Dr. Syahrial, SP - KJThariq Mubaraq DrcNoch keine Bewertungen
- MEP - Kuliah FKDokument65 SeitenMEP - Kuliah FKThariq Mubaraq DrcNoch keine Bewertungen
- Cancers 04 00307Dokument16 SeitenCancers 04 00307Thariq Mubaraq DrcNoch keine Bewertungen
- Genograms: Practical Tools PhysiciansDokument6 SeitenGenograms: Practical Tools PhysiciansThariq Mubaraq DrcNoch keine Bewertungen
- Chronic Cor-Pulmonale in Adults: An Experience From A Tertiary Teaching Hospital in DharwadDokument4 SeitenChronic Cor-Pulmonale in Adults: An Experience From A Tertiary Teaching Hospital in DharwadThariq Mubaraq DrcNoch keine Bewertungen
- JuDokument8 SeitenJuThariq Mubaraq DrcNoch keine Bewertungen
- OccupationalDokument7 SeitenOccupationalVirza Chairunnisa LatuconsinaNoch keine Bewertungen
- Immunopathology of Allergic Contact Dermatitis: Imunopatologia Da Dermatite de Contato AlérgicaDokument15 SeitenImmunopathology of Allergic Contact Dermatitis: Imunopatologia Da Dermatite de Contato AlérgicaThariq Mubaraq DrcNoch keine Bewertungen
- Exercises For Task 4Dokument5 SeitenExercises For Task 4Henrry SenaNoch keine Bewertungen
- Perbedaan Kadar Hbsag Sampel Serum Dan Plasma Metode Clia Pada PendonorDokument7 SeitenPerbedaan Kadar Hbsag Sampel Serum Dan Plasma Metode Clia Pada PendonorAAK DHGRiski MaulanaNoch keine Bewertungen
- Mendiguchia 2012 Rectus Femoris Muscle Injuries in Football-A Clinically Relevant Review of Mechanisms of Injury, Risk Factors and Preventive Strategies PDFDokument11 SeitenMendiguchia 2012 Rectus Femoris Muscle Injuries in Football-A Clinically Relevant Review of Mechanisms of Injury, Risk Factors and Preventive Strategies PDFJuan PalomoNoch keine Bewertungen
- Medic A MentosDokument1 SeiteMedic A MentosVictor Manuel Palha SemedoNoch keine Bewertungen
- Patient Medical Records: Discharge and Home-Care InstructionsDokument27 SeitenPatient Medical Records: Discharge and Home-Care InstructionsAnamaria ManceraNoch keine Bewertungen
- FD PDFDokument580 SeitenFD PDFAinul LuthfiNoch keine Bewertungen
- 1 Anti Emetics II BDS 3 June 2020 AdobeDokument28 Seiten1 Anti Emetics II BDS 3 June 2020 AdobeBishal ChauhanNoch keine Bewertungen
- (Final Proposal) 20181220 Beauttah Migiro Akuma - Research Proposal - Right To Health - Version 1.0Dokument14 Seiten(Final Proposal) 20181220 Beauttah Migiro Akuma - Research Proposal - Right To Health - Version 1.0Brian BeauttahNoch keine Bewertungen
- Liver Complications - SLEDokument5 SeitenLiver Complications - SLEFanny PritaningrumNoch keine Bewertungen
- CDK Edisi CME-2 TH 2020 5 SKP PDFDokument24 SeitenCDK Edisi CME-2 TH 2020 5 SKP PDFnarinaaviNoch keine Bewertungen
- DSWD Guidelines For Residential FacilitiesDokument12 SeitenDSWD Guidelines For Residential FacilitiesCharlene Ordoñez Dela CruzNoch keine Bewertungen
- Tangina Mo BizarDokument1 SeiteTangina Mo BizarJhon eric EscultorNoch keine Bewertungen
- Amy WebDokument62 SeitenAmy WebAnotherAnonymomNoch keine Bewertungen
- Resume-Perry Duane GriceDokument4 SeitenResume-Perry Duane Griceapi-297972018Noch keine Bewertungen
- Greater Political ParticipationDokument12 SeitenGreater Political ParticipationBe-COOL State Of MindNoch keine Bewertungen
- Computer Addiction Power Point PresentationDokument24 SeitenComputer Addiction Power Point PresentationGee A50% (4)
- York County Court Schedule For Aug. 20Dokument15 SeitenYork County Court Schedule For Aug. 20York Daily Record/Sunday NewsNoch keine Bewertungen
- Nilai Lab NormalDokument3 SeitenNilai Lab Normalraa_zhraNoch keine Bewertungen
- DiphtheriaDokument11 SeitenDiphtheriabrigde_xNoch keine Bewertungen
- Biocare GuidelinesDokument3 SeitenBiocare GuidelinesnsjunnarkarNoch keine Bewertungen