Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Oral and Esophageal DisordersDokument33 SeitenOral and Esophageal DisordersSandeepNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- ATI Community Health Proctored Exam 2020Dokument7 SeitenATI Community Health Proctored Exam 20204 u0% (1)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- PQCNC clOUDi Kickoff Main 2021Dokument27 SeitenPQCNC clOUDi Kickoff Main 2021kcochranNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- Abnormal Psychology SyllabusDokument17 SeitenAbnormal Psychology SyllabusAkhu C CeyrranneNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Prepared By: Manisha Thapa Leeza ShresthaDokument12 SeitenPrepared By: Manisha Thapa Leeza ShresthaManjesh Mishra XettriNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- IFU Wondfo SARS CoV 2 Antibody Test (Lateral Flow Method) PDFDokument2 SeitenIFU Wondfo SARS CoV 2 Antibody Test (Lateral Flow Method) PDFEndrio R HartonoNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Medik FamiliDokument10 SeitenMedik FamiliBig DaddyCoolNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Speedo Snail: Quick Review: Drugs: Mode/Mechanism of ActionDokument15 SeitenSpeedo Snail: Quick Review: Drugs: Mode/Mechanism of ActionGustavo A OrtegonNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Coronary Artery Disease & Hypertension Practice Quiz (50 Questions)Dokument18 SeitenCoronary Artery Disease & Hypertension Practice Quiz (50 Questions)Erica Veluz LuyunNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
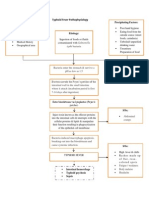
- Typhoid Fever PathophysiologyDokument1 SeiteTyphoid Fever Pathophysiologynesjyn75% (4)
- Study Literature Review: The Effect of Lockdown On The Covid19 Pandemic Period On Air QualityDokument10 SeitenStudy Literature Review: The Effect of Lockdown On The Covid19 Pandemic Period On Air QualityCeclia SousaNoch keine Bewertungen
- Differntial Diagnosis Between Diseases: Dr. Mohi IsmailDokument71 SeitenDifferntial Diagnosis Between Diseases: Dr. Mohi Ismailamamùra maamarNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Pembacaan Jurnal NEURODokument22 SeitenPembacaan Jurnal NEUROTeisha JVNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Hematologic Diagnostic Tests ExplainedDokument15 SeitenHematologic Diagnostic Tests ExplainedMichael Baylon DueñasNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- MetabolismDokument16 SeitenMetabolismAdiShineNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- PracticalDokument89 SeitenPracticalAthEer AhmadNoch keine Bewertungen
- Sujok TreatmentDokument34 SeitenSujok Treatmentflopalan100% (10)
- COVID-19 and Autoimmune DiseasesDokument8 SeitenCOVID-19 and Autoimmune DiseasesMan'SzAr'diAnSyAhNoch keine Bewertungen
- DR Ken LiegnerDokument43 SeitenDR Ken LiegnertonerangerNoch keine Bewertungen
- DAFPUS Psikosomatis NewDokument5 SeitenDAFPUS Psikosomatis NewEvy LiesniawatiNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Potential Nursing Diagnosis: Risk for InfectionDokument2 SeitenPotential Nursing Diagnosis: Risk for InfectionKarl KiwisNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- MAPEH 8 1st Quarter Exam for Cabugao Integrated SchoolDokument3 SeitenMAPEH 8 1st Quarter Exam for Cabugao Integrated SchoolMa. Reina Gail T. LizasoNoch keine Bewertungen
- Disorders of The Adrenal GlandsDokument9 SeitenDisorders of The Adrenal Glandsmoon businessNoch keine Bewertungen
- Lecture 5.3 Metabolic Errors of Carbohydrates PART 3Dokument8 SeitenLecture 5.3 Metabolic Errors of Carbohydrates PART 3Huzaifa MehmoodNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Ulcerative ColitisDokument18 SeitenUlcerative ColitisKasuganti koteshwar raoNoch keine Bewertungen
- Abnormal Psychology Plus NEW MyPsychLab 15th Edition Butcher Test Bank 1Dokument36 SeitenAbnormal Psychology Plus NEW MyPsychLab 15th Edition Butcher Test Bank 1herbertjacksonjioyzepmaf100% (22)
- CPH PrefinalDokument22 SeitenCPH PrefinalZharmaine ChavezNoch keine Bewertungen
- Horner's Syndrome As A Complication of Thyroidectomy: Report of A CaseDokument3 SeitenHorner's Syndrome As A Complication of Thyroidectomy: Report of A CaseDanielle SangalangNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- HPV (Human Papilloma Virus)Dokument20 SeitenHPV (Human Papilloma Virus)DeneseJocsonNoch keine Bewertungen
- National TB Control ManualDokument223 SeitenNational TB Control ManualTrishenth FonsekaNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)