Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- All Shifting Final Exam Questions Complete First Shift: M Ultiple C HoiceDokument11 SeitenAll Shifting Final Exam Questions Complete First Shift: M Ultiple C HoicejuliusNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Written Revalida - 2012Dokument21 SeitenWritten Revalida - 2012juliusNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- BurnsDokument4 SeitenBurnsjuliusNoch keine Bewertungen
- Case 11 Lower Genital UTIDokument2 SeitenCase 11 Lower Genital UTIjuliusNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Female Infertility: An OverviewDokument12 SeitenFemale Infertility: An OverviewSuhar TomiNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Male Hypogonadism - Basic, Clinical, and Therapeutic Principles PDFDokument407 SeitenMale Hypogonadism - Basic, Clinical, and Therapeutic Principles PDFMansoor Abbas100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- L5 The Menstrual CycleDokument12 SeitenL5 The Menstrual CycleKatrina Salas MiclatNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Biology 12 - The Reproductive System!: Name: Block: DateDokument4 SeitenBiology 12 - The Reproductive System!: Name: Block: DateLerr Real Relle100% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Amenorrhea - Algorithm & DifferentialsDokument9 SeitenAmenorrhea - Algorithm & DifferentialsItharshan IndreswaranNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Infertility: Presented ByDokument47 SeitenInfertility: Presented ByNilakshi Barik MandalNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- CTS-3 STARS Academy Multan Campus-Secure PDFDokument14 SeitenCTS-3 STARS Academy Multan Campus-Secure PDFHanzala ShahidNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- AmenorrheaDokument41 SeitenAmenorrheadoraNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Reproductive and Endocrine System: Role of Hormones in The Male and Female Reproductive SystemDokument47 SeitenReproductive and Endocrine System: Role of Hormones in The Male and Female Reproductive Systempj100% (2)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- HY EndocrineDokument22 SeitenHY EndocrineoopsseNoch keine Bewertungen
- Exercise and The Menstrual CycleDokument14 SeitenExercise and The Menstrual CycleAndrew HaslettNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Animal Biotechnology For Livestock Production 3 Springer, 2023Dokument334 SeitenAnimal Biotechnology For Livestock Production 3 Springer, 2023Gilbert MethewNoch keine Bewertungen
- 2nd Year Mcqs - Mcqs Physiology MedicalDokument4 Seiten2nd Year Mcqs - Mcqs Physiology MedicalKhadijaSarwarNoch keine Bewertungen
- Growing Pains: Problems With Puberty Suppression in Treating Gender DysphoriaDokument34 SeitenGrowing Pains: Problems With Puberty Suppression in Treating Gender DysphoriaColin Wright100% (2)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Ob Maternity NotesDokument46 SeitenOb Maternity Notesr79cb5480100% (4)
- The Breasts Do Become Sensitive and Some Women DoDokument14 SeitenThe Breasts Do Become Sensitive and Some Women DoJaymih Santos AbasoloNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Embryo TransferDokument21 SeitenEmbryo TransferMARCO ANTONIO CABRERA PASCACIONoch keine Bewertungen
- D0679sci Part2 QR 2020 FinalDokument21 SeitenD0679sci Part2 QR 2020 FinalEND GAMINGNoch keine Bewertungen
- Birth Control Pill & Lupron Sample IVF CalendarDokument2 SeitenBirth Control Pill & Lupron Sample IVF Calendarandi hamatajNoch keine Bewertungen
- Anatomy and Physiology-Endocrine SystemDokument5 SeitenAnatomy and Physiology-Endocrine SystemEixid Enna YeLikNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Bio ProjectDokument17 SeitenBio Projectsaifnkhannrahman100% (5)
- DPC-3 Word - 1Dokument42 SeitenDPC-3 Word - 1charlienitin1325Noch keine Bewertungen
- Postmenopausal Syndrome: Pronob K. Dalal, Manu AgarwalDokument11 SeitenPostmenopausal Syndrome: Pronob K. Dalal, Manu Agarwalwidya astutyloloNoch keine Bewertungen
- Reproduction in Humans: Test Yourself 18.1 (Page 335)Dokument4 SeitenReproduction in Humans: Test Yourself 18.1 (Page 335)leeNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Adolescence by John Santrock - 15e, TEST BANK 0078035481Dokument38 SeitenAdolescence by John Santrock - 15e, TEST BANK 0078035481jksnmmmNoch keine Bewertungen
- Open Breast Disorders (Benign and Malignant) DoneDokument117 SeitenOpen Breast Disorders (Benign and Malignant) Donereema.saleh123Noch keine Bewertungen
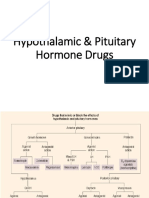
- Hypothalamic & Pituitary Hormone DrugsDokument29 SeitenHypothalamic & Pituitary Hormone DrugsDylan MansillaNoch keine Bewertungen
- Body Condition and Suckling As Factor Influencing The Duration of Postpartum Anestrum in Cattle.Dokument26 SeitenBody Condition and Suckling As Factor Influencing The Duration of Postpartum Anestrum in Cattle.Raul KimNoch keine Bewertungen
- Up-To-Date Review About Minipuberty and Overview On Hypothalamic-Pituitary-Gonadal Axis Activation in Fetal and Neonatal LifeDokument9 SeitenUp-To-Date Review About Minipuberty and Overview On Hypothalamic-Pituitary-Gonadal Axis Activation in Fetal and Neonatal LifeBerry BancinNoch keine Bewertungen
- PNLE II For Maternal and Child HealthDokument13 SeitenPNLE II For Maternal and Child HealthASDF ASDF100% (1)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)