Das könnte Ihnen auch gefallen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- All Shifting Final Exam Questions Complete First Shift: M Ultiple C HoiceDokument11 SeitenAll Shifting Final Exam Questions Complete First Shift: M Ultiple C HoicejuliusNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Written Revalida - 2012Dokument21 SeitenWritten Revalida - 2012juliusNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- BurnsDokument4 SeitenBurnsjuliusNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Case 11 Lower Genital UTIDokument2 SeitenCase 11 Lower Genital UTIjuliusNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Lecture - 4 - 28june2023Dokument18 SeitenLecture - 4 - 28june2023vanshikaNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- General Mathematics - Module #3Dokument7 SeitenGeneral Mathematics - Module #3Archie Artemis NoblezaNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- RBG - CRM BRD - Marketing - v4.1Dokument68 SeitenRBG - CRM BRD - Marketing - v4.1Manvi Pareek100% (2)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- الاستراتيجية الامنية الأمريكيةDokument141 Seitenالاستراتيجية الامنية الأمريكيةAhmedZEMMITNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Section D Textual QuestionsDokument52 SeitenSection D Textual Questionsxander ganderNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Isc Class 11 Maths Sample Paper Model 1Dokument2 SeitenIsc Class 11 Maths Sample Paper Model 1Gaurav ShuklaNoch keine Bewertungen
- Thompson VarelaDokument18 SeitenThompson VarelaGiannis NinosNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- 2007 - Q1 NewsletterDokument20 Seiten2007 - Q1 NewsletterKisara YatiyawelaNoch keine Bewertungen
- Emotional Intelligence - WikipediaDokument10 SeitenEmotional Intelligence - WikipediaJellie MendozaNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Class Program 2019 2020Dokument2 SeitenClass Program 2019 2020Cristy Gongon100% (5)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- 10 Applications in Engineering Mechanics PDFDokument10 Seiten10 Applications in Engineering Mechanics PDFWolf Lord100% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Kalki ProjectDokument3 SeitenKalki ProjectMandar SohoniNoch keine Bewertungen
- CO - Config Sap Top JobsDokument81 SeitenCO - Config Sap Top JobsAditya PakalaNoch keine Bewertungen
- TARA FrameworkDokument2 SeitenTARA Frameworkdominic100% (1)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- SF3300Dokument2 SeitenSF3300benoitNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- DocumentDokument4 SeitenDocumentJuliana ZamorasNoch keine Bewertungen
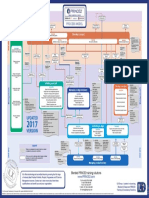
- p2 Process Model 2017Dokument1 Seitep2 Process Model 2017Miguel Fernandes0% (1)
- Time UntimeDokument10 SeitenTime UntimeMacmillan Publishers11% (27)
- TENSES ExerciseDokument28 SeitenTENSES ExerciseKhanh PhamNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Slides - Simple Linear RegressionDokument35 SeitenSlides - Simple Linear RegressionJarir AhmedNoch keine Bewertungen
- DataSheet CertificationPaths InsuranceSuite AnalystsDokument7 SeitenDataSheet CertificationPaths InsuranceSuite Analystsshanmuga89Noch keine Bewertungen
- People vs. Orbecido Iii Case DigestDokument2 SeitenPeople vs. Orbecido Iii Case DigestCristine LabutinNoch keine Bewertungen
- Project RealDokument4 SeitenProject RealKenneth Jay BagandoNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Monkey Shine - ScriptDokument4 SeitenMonkey Shine - Scriptapi-583045984Noch keine Bewertungen
- Chapter 1Dokument13 SeitenChapter 1Jerard AnciroNoch keine Bewertungen
- Adeyinka Wulemat Olarinmoye - The Images of Women in Yoruban Folktales PDFDokument12 SeitenAdeyinka Wulemat Olarinmoye - The Images of Women in Yoruban Folktales PDFAngel SánchezNoch keine Bewertungen
- Medication Instructions Prior To SurgeryDokument11 SeitenMedication Instructions Prior To Surgeryhohj100% (1)
- Background Essay LSA Skills (Speaking)Dokument12 SeitenBackground Essay LSA Skills (Speaking)Zeynep BeydeşNoch keine Bewertungen
- Creativity and AestheticDokument17 SeitenCreativity and AestheticSyahirah Erahzs100% (1)
- Creative LeadershipDokument6 SeitenCreative LeadershipRaffy Lacsina BerinaNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)