Das könnte Ihnen auch gefallen
- A Study of Menstrual Distress Questionnaire in First Year Medical StudentsDokument4 SeitenA Study of Menstrual Distress Questionnaire in First Year Medical StudentswidyaersafitriNoch keine Bewertungen
- Eating Attitude Test 26Dokument4 SeitenEating Attitude Test 26Dedeh SuherniNoch keine Bewertungen
- Root Canal Irrigation Solutions and Shaping ProceduresDokument9 SeitenRoot Canal Irrigation Solutions and Shaping ProceduresTara Lingating0% (1)
- Major Histocompatibility ComplexDokument15 SeitenMajor Histocompatibility ComplexsanasharNoch keine Bewertungen
- Human Leukocyte Antigens: Dr. B.Vijayasree 1 Year Post-Graduate Department of MicrobiologyDokument30 SeitenHuman Leukocyte Antigens: Dr. B.Vijayasree 1 Year Post-Graduate Department of Microbiologyvijayasree bavireddyNoch keine Bewertungen
- LS3310 Clin Imm WK 1 HLA 2010-2011Dokument36 SeitenLS3310 Clin Imm WK 1 HLA 2010-2011Colbert NcubeNoch keine Bewertungen
- Lecture 8 MHCDokument4 SeitenLecture 8 MHCJake MillerNoch keine Bewertungen
- Seatwork On HLA and Polyagglutination by Bryan LeeDokument3 SeitenSeatwork On HLA and Polyagglutination by Bryan LeeIsabella CeaNoch keine Bewertungen
- Major Histocompatibility Complex: Role in Immune Response and Disease SusceptibilityDokument16 SeitenMajor Histocompatibility Complex: Role in Immune Response and Disease Susceptibilityمروه عماد عيسىNoch keine Bewertungen
- MHC MoleculeDokument45 SeitenMHC MoleculeShah NAWAZNoch keine Bewertungen
- Infectious Diseases and Immunity: Special Reference To Major Histocompatibility ComplexDokument9 SeitenInfectious Diseases and Immunity: Special Reference To Major Histocompatibility ComplexEndashew AlemuNoch keine Bewertungen
- MHC and Disease Susceptibility (Type 1 Diabetes As Example)Dokument8 SeitenMHC and Disease Susceptibility (Type 1 Diabetes As Example)FATbovenNoch keine Bewertungen
- RespirationDokument20 SeitenRespirationdr_swaralipiNoch keine Bewertungen
- HLA Typing: Understanding the Critical Genetic Test for Transplant MatchingDokument14 SeitenHLA Typing: Understanding the Critical Genetic Test for Transplant MatchingSCREEN SENSE ENTERTAINMENTNoch keine Bewertungen
- Immunology MHCDokument7 SeitenImmunology MHCAbdullah EssaNoch keine Bewertungen
- Major Histocompatibility Complex (MHC) and TCRDokument59 SeitenMajor Histocompatibility Complex (MHC) and TCRPuyi Puyenk100% (1)
- Clinical Role of Human Leukocyte Antigen in Health and DiseaseDokument24 SeitenClinical Role of Human Leukocyte Antigen in Health and Diseasejeremy romero ramirezNoch keine Bewertungen
- Sequence Variability Analysis of Human Class I and Class II MHC MoleculesDokument19 SeitenSequence Variability Analysis of Human Class I and Class II MHC MoleculesFernando Fernández GarcíaNoch keine Bewertungen
- Hla Typing and Transplant Immunology: Moderator: DR Biman SaikiaDokument70 SeitenHla Typing and Transplant Immunology: Moderator: DR Biman SaikialbNoch keine Bewertungen
- Immune Regulation: Antibodies and T-Cell Receptors (TCRS)Dokument43 SeitenImmune Regulation: Antibodies and T-Cell Receptors (TCRS)fakhirNoch keine Bewertungen
- 7.MHC and TransplantationDokument34 Seiten7.MHC and Transplantationعوض الكريمNoch keine Bewertungen
- Lectura Seminario 6Dokument19 SeitenLectura Seminario 6salma pejerreyNoch keine Bewertungen
- HLA system-HLA Typing and Its Role in Tissue TransplantationDokument48 SeitenHLA system-HLA Typing and Its Role in Tissue TransplantationAshikNoch keine Bewertungen
- MHC (Major Histocompatibility Complex) : StructureDokument5 SeitenMHC (Major Histocompatibility Complex) : StructureAhmad Farid OthmanNoch keine Bewertungen
- Antigen Processing and Presentation PDFDokument36 SeitenAntigen Processing and Presentation PDFMarinero CzarNoch keine Bewertungen
- Human Leukocyte Antigen (HLA) System: Alkitab University College of Technology Medical Department of Medical AnalysisDokument4 SeitenHuman Leukocyte Antigen (HLA) System: Alkitab University College of Technology Medical Department of Medical AnalysisMohammed R.HusseinNoch keine Bewertungen
- download (1)Dokument9 Seitendownload (1)kahkashanahmed065Noch keine Bewertungen
- Major Histocompatibilty Complex(Mhc)Dokument13 SeitenMajor Histocompatibilty Complex(Mhc)boscomooliNoch keine Bewertungen
- Human Leukocyte Antigens (HLA) - A Roadmap - UpToDateDokument19 SeitenHuman Leukocyte Antigens (HLA) - A Roadmap - UpToDateVivek GoswamiNoch keine Bewertungen
- Antigen Processing and PresentationDokument2 SeitenAntigen Processing and PresentationEllya Latifah IlyasNoch keine Bewertungen
- 9.MHC in Immune Response-2Dokument16 Seiten9.MHC in Immune Response-2alhyarylyn3Noch keine Bewertungen
- His to Comp at AbilityDokument24 SeitenHis to Comp at AbilitycyskinkropsNoch keine Bewertungen
- 02immunodermatology-120316150656-phpapp01Dokument29 Seiten02immunodermatology-120316150656-phpapp01kahkashanahmed065Noch keine Bewertungen
- LECTURE 17 Major Histocompatibility MoleculesDokument7 SeitenLECTURE 17 Major Histocompatibility MoleculesDomenica Mishel Sandoval SegoviaNoch keine Bewertungen
- Sam CD Rom - ImmunologyDokument111 SeitenSam CD Rom - ImmunologyDr. Muha. Hasan Mahbub-Ur-RahmanNoch keine Bewertungen
- Major Histocompatibility Complex: More Than One Class of MHCDokument3 SeitenMajor Histocompatibility Complex: More Than One Class of MHCTONY GO AWAYNoch keine Bewertungen
- Genetics of Autoimmune DiseasesDokument7 SeitenGenetics of Autoimmune Diseasesolympiakos7Noch keine Bewertungen
- AutoimmunityDokument8 SeitenAutoimmunityRachit NarangNoch keine Bewertungen
- Bulek 2012Dokument8 SeitenBulek 2012Marco Antonio PrettiNoch keine Bewertungen
- Lecture MHCDokument33 SeitenLecture MHCrockyrawat01012003Noch keine Bewertungen
- What are the HLA genes? (38 charactersDokument2 SeitenWhat are the HLA genes? (38 characterspoojaNoch keine Bewertungen
- Molecular Basis For HLA-DQ Associations With IDDM: Perspectives in DiabetesDokument8 SeitenMolecular Basis For HLA-DQ Associations With IDDM: Perspectives in DiabetesLigia AbdalaNoch keine Bewertungen
- Immune SystemDokument32 SeitenImmune Systemanupama menonNoch keine Bewertungen
- Hla ManualDokument12 SeitenHla Manualhashimelhaj100% (1)
- Pathology Review of Immune System Diseases and Hypersensitivity ReactionsDokument270 SeitenPathology Review of Immune System Diseases and Hypersensitivity ReactionsDianaNitaNoch keine Bewertungen
- Class 8 MHC - LSDokument32 SeitenClass 8 MHC - LSDarwin QuinterosNoch keine Bewertungen
- Deficiencias en MHC I Y IIDokument7 SeitenDeficiencias en MHC I Y IIJuan David CortesNoch keine Bewertungen
- Antigen Processing and PresentationDokument23 SeitenAntigen Processing and PresentationMin KyuNoch keine Bewertungen
- HBB 2306 Notes IIDokument14 SeitenHBB 2306 Notes IIfelixNoch keine Bewertungen
- Slide MHC HlaDokument47 SeitenSlide MHC HlaSandi AuliaNoch keine Bewertungen
- Major Histocompatibility Complex-HypersensitivityDokument10 SeitenMajor Histocompatibility Complex-HypersensitivityJesuhovie Solomon OkpobrisiNoch keine Bewertungen
- Function and structure of Antibodies and MHC Class I and II antigensDokument60 SeitenFunction and structure of Antibodies and MHC Class I and II antigensZubair YousafNoch keine Bewertungen
- Major Histocompatibility Complex and Hematopoietic Stem Cell Transplantation: Beyond The Classical HLA PolymorphismDokument14 SeitenMajor Histocompatibility Complex and Hematopoietic Stem Cell Transplantation: Beyond The Classical HLA PolymorphismSara María Vargas CastilloNoch keine Bewertungen
- Self Peptidome Variation Shapes Individual ImmuneDokument7 SeitenSelf Peptidome Variation Shapes Individual ImmuneannavictoriaaltierivanniNoch keine Bewertungen
- Mechanisms of Immunologic Tolerance and AutoimmunityDokument65 SeitenMechanisms of Immunologic Tolerance and AutoimmunityPrincewill Seiyefa100% (1)
- Genetic Susceptibility To Autoimmune Diseases & MechanismsDokument3 SeitenGenetic Susceptibility To Autoimmune Diseases & MechanismsZara MohammedNoch keine Bewertungen
- MHCDokument25 SeitenMHCSAMUELNoch keine Bewertungen
- HLA Sensitisation - Can It Be PreventedDokument11 SeitenHLA Sensitisation - Can It Be PreventedPatriciaNoch keine Bewertungen
- Immunology of Transplant Rejection: More..Dokument7 SeitenImmunology of Transplant Rejection: More..kusumrajaiNoch keine Bewertungen
- He Dual Role of HLA-C in Tolerance and Immunity at The Maternal-Fetal InterfaceDokument14 SeitenHe Dual Role of HLA-C in Tolerance and Immunity at The Maternal-Fetal Interface石一Noch keine Bewertungen
- Roit ChapaDokument10 SeitenRoit ChapaValentin UngureanuNoch keine Bewertungen
- Cellular and Molecular Mechanisms of Inflammation: Receptors of Inflammatory Cells: Structure—Function RelationshipsVon EverandCellular and Molecular Mechanisms of Inflammation: Receptors of Inflammatory Cells: Structure—Function RelationshipsCharles G. CochraneNoch keine Bewertungen
- Solis N90Dokument2 SeitenSolis N90chrisNoch keine Bewertungen
- Agents Classified by The IARC Monographs, Volumes 1-125 PDFDokument39 SeitenAgents Classified by The IARC Monographs, Volumes 1-125 PDFchrisNoch keine Bewertungen
- Emergency Drug GuidelinesDokument59 SeitenEmergency Drug GuidelinesAries TauNoch keine Bewertungen
- SCOPE Outgoing Manual 2014 PDFDokument23 SeitenSCOPE Outgoing Manual 2014 PDFchrisNoch keine Bewertungen
- Slides From Ten Cate Seminar On UHC, CBE and EPAs July 3 2018 GenevaDokument46 SeitenSlides From Ten Cate Seminar On UHC, CBE and EPAs July 3 2018 GenevachrisNoch keine Bewertungen
- Acs Ca3 BookDokument69 SeitenAcs Ca3 BookchrisNoch keine Bewertungen
- Wcd19 How To Guide Get Social Fa EnglishDokument10 SeitenWcd19 How To Guide Get Social Fa EnglishchrisNoch keine Bewertungen
- Father ForgetsDokument1 SeiteFather ForgetsAlfredo Cumbi CumbiNoch keine Bewertungen
- Good Medical Practice English 1215 PDF 51527435Dokument40 SeitenGood Medical Practice English 1215 PDF 51527435ñkjn100% (1)
- Eng BTSDokument62 SeitenEng BTSKamleshNoch keine Bewertungen
- ATLS Power Point PDFDokument54 SeitenATLS Power Point PDFRizky LumalessilNoch keine Bewertungen
- A174325 PDFDokument141 SeitenA174325 PDFchrisNoch keine Bewertungen
- 3M Mask 6000 SeriesDokument4 Seiten3M Mask 6000 SerieschrisNoch keine Bewertungen
- 7 Paediatric Anatomy Physiology and The Basics of Paediatric AnaesthesiaDokument12 Seiten7 Paediatric Anatomy Physiology and The Basics of Paediatric AnaesthesiakochikaghochiNoch keine Bewertungen
- America'S Romance With Greek RevivalDokument10 SeitenAmerica'S Romance With Greek RevivalchrisNoch keine Bewertungen
- Syllabus PRMDokument3 SeitenSyllabus PRMchrisNoch keine Bewertungen
- The International Medical Students' Congress of BucharestDokument33 SeitenThe International Medical Students' Congress of BucharestchrisNoch keine Bewertungen
- Colloquium 6 TranslatedDokument7 SeitenColloquium 6 TranslatedchrisNoch keine Bewertungen
- Disaster MedicineDokument4 SeitenDisaster MedicinechrisNoch keine Bewertungen
- Candesartan's Analgesic Effects in Rats and MiceDokument3 SeitenCandesartan's Analgesic Effects in Rats and MicechrisNoch keine Bewertungen
- Candesartan's Analgesic Effects in Rats and MiceDokument3 SeitenCandesartan's Analgesic Effects in Rats and MicechrisNoch keine Bewertungen
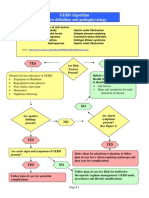
- GERD Algorithm Review Definition and Pathophysiology: NO YESDokument3 SeitenGERD Algorithm Review Definition and Pathophysiology: NO YESdianyNoch keine Bewertungen
- History ObgynDokument37 SeitenHistory ObgynRana WaelNoch keine Bewertungen
- Chapter 21 DigestionDokument96 SeitenChapter 21 DigestionJwnsbdhdNoch keine Bewertungen
- Burnout Syndrome - Stress in Health Care Professionals Working To Fight Covid-19 in Public HospitalsDokument14 SeitenBurnout Syndrome - Stress in Health Care Professionals Working To Fight Covid-19 in Public HospitalsIJAERS JOURNALNoch keine Bewertungen
- Special Populations PDFDokument4 SeitenSpecial Populations PDFLouis TrầnNoch keine Bewertungen
- Risk Factors For Surgical Site InfectionDokument5 SeitenRisk Factors For Surgical Site InfectionElizabeth Mautino CaceresNoch keine Bewertungen
- Basic Geriatric Nursing 6th Edition Williams Test BankDokument10 SeitenBasic Geriatric Nursing 6th Edition Williams Test Bankwheretoenough7rv77Noch keine Bewertungen
- Taking History in MedicineDokument20 SeitenTaking History in Medicineprincemasr6Noch keine Bewertungen
- Granulomatous InflammationDokument20 SeitenGranulomatous InflammationPradeep100% (3)
- Unit 3 Part 1 Introduction To Autoimmune DisordersDokument14 SeitenUnit 3 Part 1 Introduction To Autoimmune DisordersReman AlingasaNoch keine Bewertungen
- Pharm Calcium Channel Blockers (Bahar&Amy) "Vera Dialed The Calcium Channel To Buy A Knife" Verapramil, Diltizaem, NifedipineDokument7 SeitenPharm Calcium Channel Blockers (Bahar&Amy) "Vera Dialed The Calcium Channel To Buy A Knife" Verapramil, Diltizaem, Nifedipinecherrybombaz100% (4)
- Disease Essay-RubricDokument2 SeitenDisease Essay-Rubricapi-321155161Noch keine Bewertungen
- COVID-19 MRNA Pfizer - BioNTech Vaccine Analysis PrintDokument69 SeitenCOVID-19 MRNA Pfizer - BioNTech Vaccine Analysis PrintSkunk BOINoch keine Bewertungen
- Leprosy and RabiesDokument14 SeitenLeprosy and RabiesFayhaa NadeemNoch keine Bewertungen
- Thoracentesis IntroductionDokument8 SeitenThoracentesis Introductionjyoti singhNoch keine Bewertungen
- Understanding the Mind-Body Link in Chronic IllnessDokument3 SeitenUnderstanding the Mind-Body Link in Chronic IllnessJitendra SinghNoch keine Bewertungen
- "Virtopsy" Virtual Alternative For Post-Mortem Investigation in Pandemic Era of Covid-19: Diagnostic Approach To Reduce The Menace of Contagion: - A ReviewDokument6 Seiten"Virtopsy" Virtual Alternative For Post-Mortem Investigation in Pandemic Era of Covid-19: Diagnostic Approach To Reduce The Menace of Contagion: - A ReviewInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- Briefing Practical Literature Searching and Critical Appraisal (Diagnosis and Therapy) - Dr. Lukman Ade Chandra, M.med., M. Phil (2022)Dokument16 SeitenBriefing Practical Literature Searching and Critical Appraisal (Diagnosis and Therapy) - Dr. Lukman Ade Chandra, M.med., M. Phil (2022)Sheila Tirta AyumurtiNoch keine Bewertungen
- The Facts About AidsDokument5 SeitenThe Facts About AidsTAMBAKI EDMONDNoch keine Bewertungen
- Clinical Approach To Respiratory Distress in NewbornDokument29 SeitenClinical Approach To Respiratory Distress in Newbornabhivnair100% (1)
- Ainu Illness&healingDokument21 SeitenAinu Illness&healingRaluca MoiseNoch keine Bewertungen
- Risk Factors and Teaching for Laryngeal Cancer PatientDokument2 SeitenRisk Factors and Teaching for Laryngeal Cancer Patientatarisgurl08100% (1)
- Ii Anatomy+and+physiologyDokument2 SeitenIi Anatomy+and+physiologybillyktoubattsNoch keine Bewertungen
- OSCE Revision Guide: Breaking Bad News, Inhaler Use, Breastfeeding Counseling & MoreDokument19 SeitenOSCE Revision Guide: Breaking Bad News, Inhaler Use, Breastfeeding Counseling & MoreShaikah NNoch keine Bewertungen
- Balance Retraining YardleyDokument10 SeitenBalance Retraining YardleystepwiseclicheNoch keine Bewertungen
- Mental Health Effects of ObesityDokument7 SeitenMental Health Effects of ObesityMohd FaizNoch keine Bewertungen
- Stroke PresentationDokument24 SeitenStroke PresentationKen TokkNoch keine Bewertungen