Das könnte Ihnen auch gefallen
- Ectopic Pregnancy1Dokument34 SeitenEctopic Pregnancy1Kreshimaricon FurigayNoch keine Bewertungen
- Ectopic Pregnancy - MedscapeDokument31 SeitenEctopic Pregnancy - Medscapeantonio91uNoch keine Bewertungen
- Early Pregnancy Problems: Presented byDokument28 SeitenEarly Pregnancy Problems: Presented byMalk OmryNoch keine Bewertungen
- Ectopic Pregnancy5Dokument39 SeitenEctopic Pregnancy5Muhammad AbeeshNoch keine Bewertungen
- Week 2 Cellular LevelDokument7 SeitenWeek 2 Cellular LevelDayledaniel Sorveto100% (1)
- DVT in PregDokument2 SeitenDVT in Pregkhadzx100% (2)
- Changing Trends in Cesarean DeliveryDokument7 SeitenChanging Trends in Cesarean DeliveryEditor_IAIMNoch keine Bewertungen
- Abnormal Uterine BleedingDokument12 SeitenAbnormal Uterine BleedingGilang DermawanNoch keine Bewertungen
- Ectopic Pregnancy William 24thDokument44 SeitenEctopic Pregnancy William 24th林昌恩Noch keine Bewertungen
- Ectopic Pregnancy: Read MoreDokument15 SeitenEctopic Pregnancy: Read MoreVanessa Santos100% (1)
- Deep Vein Thrombosis and Pulmonary Embolism in Pregnancy - Prevention - UpToDateDokument11 SeitenDeep Vein Thrombosis and Pulmonary Embolism in Pregnancy - Prevention - UpToDateGabyta007Noch keine Bewertungen
- Ulcerative ColitisDokument14 SeitenUlcerative ColitisdeepuNoch keine Bewertungen
- Menstrual Disorders: Olufemi Aworinde Lecturer/ Consultant Obstetrician and Gynaecologist, Bowen University, IwoDokument36 SeitenMenstrual Disorders: Olufemi Aworinde Lecturer/ Consultant Obstetrician and Gynaecologist, Bowen University, IwoAkinbani MoyosoreNoch keine Bewertungen
- Pharmacokinetics: - Not Bound To Plasma Proteins - Is Eliminated by The Kidneys and Liver - T1/2 5 MinutesDokument7 SeitenPharmacokinetics: - Not Bound To Plasma Proteins - Is Eliminated by The Kidneys and Liver - T1/2 5 MinutesganotNoch keine Bewertungen
- Acute GlomerulonephritisDokument28 SeitenAcute GlomerulonephritisPaul SinsNoch keine Bewertungen
- Thromboembolism & ThromboprophylaxisDokument48 SeitenThromboembolism & Thromboprophylaxisazida90Noch keine Bewertungen
- Essay On The Dignity of WorkDokument2 SeitenEssay On The Dignity of WorkFarhan AliNoch keine Bewertungen
- Approach To The Surgical PatientDokument51 SeitenApproach To The Surgical Patientsanjivdas100% (1)
- Case Study Presentation: "Ectopic Pregnancy"Dokument8 SeitenCase Study Presentation: "Ectopic Pregnancy"Sherwina Alih-BieberNoch keine Bewertungen
- Case Study-Molar PregnancyDokument14 SeitenCase Study-Molar Pregnancysimbarashe tangwadzana100% (1)
- Preterm LaborDokument41 SeitenPreterm LaborAdistri Kim100% (3)
- Wilms TumorDokument12 SeitenWilms TumorKath CamachoNoch keine Bewertungen
- Wa0000.Dokument34 SeitenWa0000.Abdelrahman AbdouNoch keine Bewertungen
- Gyne - Case 05 Abnormal Uterine BleedingDokument3 SeitenGyne - Case 05 Abnormal Uterine Bleedingcbac1990Noch keine Bewertungen
- C SectionDokument50 SeitenC SectionAlano S. LimgasNoch keine Bewertungen
- Nancy E Fay MD Facog Division of Reproductive MedicineDokument32 SeitenNancy E Fay MD Facog Division of Reproductive MedicineAdityo MulyonoNoch keine Bewertungen
- Epilepsy in Pregnancy JatuDokument57 SeitenEpilepsy in Pregnancy Jatuninjahattori1Noch keine Bewertungen
- POLYCYTHEMIADokument9 SeitenPOLYCYTHEMIAJoeven HilarioNoch keine Bewertungen
- Hydatidiform MoleDokument10 SeitenHydatidiform MoleLisa TurnerNoch keine Bewertungen
- Joint Pain - ApproachDokument32 SeitenJoint Pain - ApproachHassan Bin AjmalNoch keine Bewertungen
- (New) Early Pregnancy Complications RDokument51 Seiten(New) Early Pregnancy Complications RMesk Banat100% (2)
- Premature Rupture of MembranesDokument12 SeitenPremature Rupture of MembranesbafionitaNoch keine Bewertungen
- Abnormal UterineDokument23 SeitenAbnormal Uterinehossam626Noch keine Bewertungen
- 1 - Presentation - Management of Preclamplsia, Mild and ModerateDokument22 Seiten1 - Presentation - Management of Preclamplsia, Mild and ModeratesharonNoch keine Bewertungen
- Pelvic Inflammatory Disease Cause Infertility: A Condition Requiring Closer AttentionDokument60 SeitenPelvic Inflammatory Disease Cause Infertility: A Condition Requiring Closer AttentionVergina ClaudiaNoch keine Bewertungen
- Outline Procedure For TahbsoDokument6 SeitenOutline Procedure For TahbsoMyraNoch keine Bewertungen
- Tropical Splenomegaly SyndromeDokument12 SeitenTropical Splenomegaly SyndromeSaidAandySaida100% (1)
- Information For You: An Ectopic PregnancyDokument25 SeitenInformation For You: An Ectopic PregnancyAnonymous layszXmsNoch keine Bewertungen
- CAD - EBM September 2020 EditionDokument17 SeitenCAD - EBM September 2020 EditionNaga Venkatamanoj Kumar PakalapatiNoch keine Bewertungen
- Shoulder Dystocia 1Dokument38 SeitenShoulder Dystocia 1emilynorchidNoch keine Bewertungen
- Gastric CancerDokument7 SeitenGastric CancerMicah PingawanNoch keine Bewertungen
- Obg Icd-10 Pregnancy, Childbirth, PuerperiumDokument11 SeitenObg Icd-10 Pregnancy, Childbirth, PuerperiumarifianjuariNoch keine Bewertungen
- Fetal Growth DisordersDokument26 SeitenFetal Growth DisordersEdalyn CapiliNoch keine Bewertungen
- Hemorrhagic Conditions in Neonates: DR Hodan Ahmed, Department of Pediatrics and Child Health, Amoud Medical School, AUDokument27 SeitenHemorrhagic Conditions in Neonates: DR Hodan Ahmed, Department of Pediatrics and Child Health, Amoud Medical School, AUAbdisalan hassanNoch keine Bewertungen
- 2.11 SEPTIC ABORTION AND SEPTIC SHOCK. M. Botes PDFDokument4 Seiten2.11 SEPTIC ABORTION AND SEPTIC SHOCK. M. Botes PDFteteh_thikeuNoch keine Bewertungen
- Cervical Insufficiency:: Miscarriage Early (Premature)Dokument2 SeitenCervical Insufficiency:: Miscarriage Early (Premature)Ardelean EmanuelNoch keine Bewertungen
- Cardiac Disease in PregnancyDokument86 SeitenCardiac Disease in PregnancyAustine OdhiamboNoch keine Bewertungen
- Gestational Trophoblastic Disease (Neha Martin Msc. NSG 2nd Year)Dokument13 SeitenGestational Trophoblastic Disease (Neha Martin Msc. NSG 2nd Year)Gunu SinghNoch keine Bewertungen
- Surgery - Pediatric GIT, Abdominal Wall, Neoplasms - 2014ADokument14 SeitenSurgery - Pediatric GIT, Abdominal Wall, Neoplasms - 2014ATwinkle SalongaNoch keine Bewertungen
- Obstetric Maneuvers For Shoulder Dystocia and Associated Fetal MorbidityDokument5 SeitenObstetric Maneuvers For Shoulder Dystocia and Associated Fetal MorbidityBill HarmanNoch keine Bewertungen
- Case Study 2 PTB Plueral EffusionDokument12 SeitenCase Study 2 PTB Plueral EffusionKaren Kate AblesNoch keine Bewertungen
- Uterine Myoma, Sept, 2021Dokument63 SeitenUterine Myoma, Sept, 2021Kerod AbebeNoch keine Bewertungen
- Scaohoid Fracture 4Dokument34 SeitenScaohoid Fracture 4Noor Al Zahraa Ali100% (1)
- PPH 2024Dokument25 SeitenPPH 2024Anthony Mwangi100% (1)
- Cervical CancerDokument5 SeitenCervical Cancerjinoop100% (1)
- Ovarian CancerDokument15 SeitenOvarian CancerAlmasNoch keine Bewertungen
- Abnormal Uterine Bleeding: - Rou'a Eyad - Rahaf EyadDokument35 SeitenAbnormal Uterine Bleeding: - Rou'a Eyad - Rahaf EyadYazeed Asrawi0% (1)
- Benign Lesions of Vulva and VaginaDokument34 SeitenBenign Lesions of Vulva and VaginaCabdiNoch keine Bewertungen
- Mal Presentations Mal PositionsDokument4 SeitenMal Presentations Mal PositionsMelissa Aina Mohd YusofNoch keine Bewertungen
- Can You Help Fairies Find Their HomeDokument1 SeiteCan You Help Fairies Find Their HomeSiska FriedmanNoch keine Bewertungen
- B - Yonanda Adi (Stroke)Dokument10 SeitenB - Yonanda Adi (Stroke)Siska FriedmanNoch keine Bewertungen
- Pre EclampsiaDokument15 SeitenPre EclampsiaSiska FriedmanNoch keine Bewertungen
- D - Rochmanita Safitri (Skoliosis)Dokument59 SeitenD - Rochmanita Safitri (Skoliosis)Siska FriedmanNoch keine Bewertungen
- C - Kavinan Subramaniam - Heart FailureDokument5 SeitenC - Kavinan Subramaniam - Heart FailureSiska FriedmanNoch keine Bewertungen
- FigureDokument1 SeiteFigureSiska FriedmanNoch keine Bewertungen
- Hyperemesis GravidarumDokument12 SeitenHyperemesis GravidarumSiska FriedmanNoch keine Bewertungen
- Ectopic Pregnancy JournalDokument3 SeitenEctopic Pregnancy JournalSiska FriedmanNoch keine Bewertungen
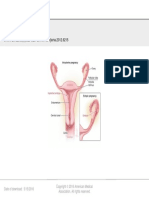
- From: Ectopic Pregnancy: JAMA. 2012 308 (8) :829-829. Doi:10.1001/jama.2012.6215Dokument1 SeiteFrom: Ectopic Pregnancy: JAMA. 2012 308 (8) :829-829. Doi:10.1001/jama.2012.6215Siska FriedmanNoch keine Bewertungen
- Plant Start Up Timeline - 24 Aug 09 - Rev 1Dokument1 SeitePlant Start Up Timeline - 24 Aug 09 - Rev 1Siska FriedmanNoch keine Bewertungen
- Sue Ryder in AlbaniaDokument2 SeitenSue Ryder in AlbaniaShef DomiNoch keine Bewertungen
- Notice: Medical Devices: Recognized Standards List Modifications (Recognition List Number 019)Dokument7 SeitenNotice: Medical Devices: Recognized Standards List Modifications (Recognition List Number 019)Justia.comNoch keine Bewertungen
- Botox EbookDokument15 SeitenBotox Ebookdoraemon100% (2)
- Harmful Side Effects of Loud MusicDokument3 SeitenHarmful Side Effects of Loud Music90002Noch keine Bewertungen
- L2 - Retention & ResistanceDokument20 SeitenL2 - Retention & Resistancetalal_11Noch keine Bewertungen
- Splenic InfarctionDokument20 SeitenSplenic InfarctionMộtHaiBaNoch keine Bewertungen
- ACI Adult Neurological Observation Chart Education PackageDokument101 SeitenACI Adult Neurological Observation Chart Education Packagevanphanthuy110Noch keine Bewertungen
- NP020110 P18table1Dokument1 SeiteNP020110 P18table1Celine SuryaNoch keine Bewertungen
- Disjonction Atlanto-Occipitale PDFDokument9 SeitenDisjonction Atlanto-Occipitale PDFAminou BugattiNoch keine Bewertungen
- Approach To Spontaneous PneumothoraxDokument25 SeitenApproach To Spontaneous PneumothoraxMohdGhazaliAcoyNoch keine Bewertungen
- Anesthesia in Day Care SurgeryDokument143 SeitenAnesthesia in Day Care SurgeryGmkmcNoch keine Bewertungen
- SulbutiamineDokument1 SeiteSulbutiaminezamurd76Noch keine Bewertungen
- Rheumatology SheetDokument54 SeitenRheumatology SheetO.r. CadzNoch keine Bewertungen
- Guidelines For Writing EEG Reports of ACNSDokument4 SeitenGuidelines For Writing EEG Reports of ACNStuanamg66Noch keine Bewertungen
- Journal Reading: Chronic Kidney Disease Related To Renal Tuberculosis: A Case ReportDokument15 SeitenJournal Reading: Chronic Kidney Disease Related To Renal Tuberculosis: A Case ReportnikoapredoNoch keine Bewertungen
- Hypovolemia PresentationDokument5 SeitenHypovolemia PresentationjavibruinNoch keine Bewertungen
- Traumatic HyphemaDokument4 SeitenTraumatic HyphemaFiny FaradisaNoch keine Bewertungen
- Hospital Administratin Control RoomDokument9 SeitenHospital Administratin Control RoomMohan DesaiNoch keine Bewertungen
- HAAD Policy On Medical WasteDokument10 SeitenHAAD Policy On Medical WasteibrahimkhansahilNoch keine Bewertungen
- Ellie Suse ResumeDokument2 SeitenEllie Suse Resumeapi-439303465Noch keine Bewertungen
- Ureteroureterostomy For Reflux Duplex SystemsDokument5 SeitenUreteroureterostomy For Reflux Duplex Systemsjithin rNoch keine Bewertungen
- ENT Notes For Med StudentsDokument4 SeitenENT Notes For Med Studentsnikki100% (1)
- Access, Orientation and Security.: Tri-Tome PCDokument2 SeitenAccess, Orientation and Security.: Tri-Tome PCNorberto MartinezNoch keine Bewertungen
- B. Within 24 Hours After DischargeDokument15 SeitenB. Within 24 Hours After DischargeRichard SonsingNoch keine Bewertungen
- Chemotherapeutic AgentDokument29 SeitenChemotherapeutic AgentQurrataini IbanezNoch keine Bewertungen
- Resume Sample For NursesDokument7 SeitenResume Sample For NursesafmrpgmgobwuseNoch keine Bewertungen
- HHS Public Access: How Schizophrenia Develops: Cognitive and Brain Mechanisms Underlying Onset of PsychosisDokument25 SeitenHHS Public Access: How Schizophrenia Develops: Cognitive and Brain Mechanisms Underlying Onset of PsychosisNoriNoch keine Bewertungen
- S RL 31072018 Desmoplastic FibromaDokument23 SeitenS RL 31072018 Desmoplastic FibromaAnonymous bE4VegCcNoch keine Bewertungen
- SOP Blood TranfussionDokument3 SeitenSOP Blood TranfussionDiana SafitriNoch keine Bewertungen
- Eliza Dobrin CVDokument2 SeitenEliza Dobrin CVALEX DOBRINNoch keine Bewertungen