Das könnte Ihnen auch gefallen
- Randomized Trial of Plastic Bags To Prevent TermDokument8 SeitenRandomized Trial of Plastic Bags To Prevent TermkemalmiaNoch keine Bewertungen
- Perineal CareDokument4 SeitenPerineal CareJny SherpaNoch keine Bewertungen
- RD ManualDokument6 SeitenRD Manualapple m.Noch keine Bewertungen
- Perinal Care FemaleDokument1 SeitePerinal Care FemaleRaquel M. MendozaNoch keine Bewertungen
- Assisting For Endotracheal IntubationDokument16 SeitenAssisting For Endotracheal IntubationSREEDEVI T SURESH100% (1)
- Course Syllabus in Primary Health Care 1Dokument7 SeitenCourse Syllabus in Primary Health Care 1Regie Arceo BautistaNoch keine Bewertungen
- Saint Paul University Philippines: School of Nursing and Allied Health SciencesDokument3 SeitenSaint Paul University Philippines: School of Nursing and Allied Health SciencesRaRe TVNoch keine Bewertungen
- Abdominal Paracentesis Procedure GuideDokument14 SeitenAbdominal Paracentesis Procedure Guideesther100% (1)
- Nursing Ear Irrigation ChecklistDokument1 SeiteNursing Ear Irrigation ChecklistOrl Trinidad0% (1)
- Dilation and Curettage (D&C)Dokument3 SeitenDilation and Curettage (D&C)Jane ElloNoch keine Bewertungen
- Fundal Height MeasurementDokument4 SeitenFundal Height MeasurementChanta MaharjanNoch keine Bewertungen
- Chest Physiotherapy TechniquesDokument9 SeitenChest Physiotherapy TechniquesLenny AlfianiNoch keine Bewertungen
- 1 - EINC With InstrumentationDokument39 Seiten1 - EINC With InstrumentationDaenna Corrine JerezaNoch keine Bewertungen
- Nightingale Institute of Nursing Noida: ON A.V. Aids Exhibition (Subject - Nursing Education)Dokument6 SeitenNightingale Institute of Nursing Noida: ON A.V. Aids Exhibition (Subject - Nursing Education)Bhawna JoshiNoch keine Bewertungen
- Bag Technique ChecklistDokument2 SeitenBag Technique ChecklistAliah Mae Alvarez100% (1)
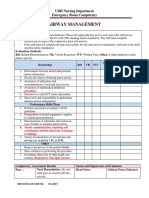
- Emergency Room Airway Management CompetencyDokument2 SeitenEmergency Room Airway Management CompetencyANNETTE GUEVARRANoch keine Bewertungen
- Tube Feeding ChecklistDokument1 SeiteTube Feeding ChecklistDanica PadillaNoch keine Bewertungen
- Trach Suction ChecklistDokument2 SeitenTrach Suction ChecklistJE MagbanuaNoch keine Bewertungen
- Checklist For The VS Measurement (TPR and BP) A. Temperature A.1. Axillary Temperature (Digital Thermometer) Done Needs PracticeDokument3 SeitenChecklist For The VS Measurement (TPR and BP) A. Temperature A.1. Axillary Temperature (Digital Thermometer) Done Needs PracticeCyrillNoch keine Bewertungen
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- Procedure Checklist Chapter 31: Logrolling A PatientDokument2 SeitenProcedure Checklist Chapter 31: Logrolling A PatientjthsNoch keine Bewertungen
- Safe Normal Vaginal Delivery GuideDokument10 SeitenSafe Normal Vaginal Delivery GuideHuirem AnilaNoch keine Bewertungen
- Assisting A Patient With AmbulationDokument3 SeitenAssisting A Patient With AmbulationLindsay Fernandez100% (1)
- Course Outline-Ncm109Dokument10 SeitenCourse Outline-Ncm109Charmagne Yanga EpantoNoch keine Bewertungen
- Procedure Checklist Chapter 23: Inserting A Rectal SuppositoryDokument1 SeiteProcedure Checklist Chapter 23: Inserting A Rectal SuppositoryjthsNoch keine Bewertungen
- Sess 1 Global StrategyDokument12 SeitenSess 1 Global StrategydaveNoch keine Bewertungen
- Comparing blood donation knowledge among science and non-science studentsDokument10 SeitenComparing blood donation knowledge among science and non-science studentsGaoudam NatarajanNoch keine Bewertungen
- Turning a Client in BedDokument2 SeitenTurning a Client in Bedbevzie datu100% (1)
- Monitoring The Progress of Labor: Marissa Villacarlos Nualla, MD, Fpogs, Fpsuog Mcu-College of MedicineDokument58 SeitenMonitoring The Progress of Labor: Marissa Villacarlos Nualla, MD, Fpogs, Fpsuog Mcu-College of MedicineRozzie ReyesNoch keine Bewertungen
- Cleansing Bed BathDokument16 SeitenCleansing Bed BathRoger ViloNoch keine Bewertungen
- Restraints StudentsDokument3 SeitenRestraints StudentsMaggay LarsNoch keine Bewertungen
- Assessing Body Temperature: Goal: Obtain Baseline Temperature Data For Comparing Future CommentsDokument3 SeitenAssessing Body Temperature: Goal: Obtain Baseline Temperature Data For Comparing Future CommentsJamie SimsNoch keine Bewertungen
- Notes On Baby Bath - Care of The Mother During The Postpartum PeriodDokument12 SeitenNotes On Baby Bath - Care of The Mother During The Postpartum PeriodOink TopusNoch keine Bewertungen
- Essential Newborn Care StepsDokument8 SeitenEssential Newborn Care StepsRaven Torres100% (1)
- Newborn Care Guide for Simulated Immediate CareDokument8 SeitenNewborn Care Guide for Simulated Immediate CareIsabelleNoch keine Bewertungen
- Levels of PreventionDokument3 SeitenLevels of PreventionJustJ ThingsNoch keine Bewertungen
- Intravenous Therapy: Bicol University Tabaco Campus Tabaco CityDokument4 SeitenIntravenous Therapy: Bicol University Tabaco Campus Tabaco CityWeeaboo Franz VlogsNoch keine Bewertungen
- NGT GavageDokument29 SeitenNGT GavageMaan LapitanNoch keine Bewertungen
- Taking Vital Signs Temperature, Pulse, Respiration, Blood Pressure DefinitionDokument20 SeitenTaking Vital Signs Temperature, Pulse, Respiration, Blood Pressure DefinitionRohlen BaguioNoch keine Bewertungen
- Anthropometric Measurements, Plotting and InterpretationDokument31 SeitenAnthropometric Measurements, Plotting and Interpretationokwadha simionNoch keine Bewertungen
- Leopolds Manuever Final 21aDokument27 SeitenLeopolds Manuever Final 21aArun Roa DanielNoch keine Bewertungen
- Bag Technique Checklists CHN 1 (SL)Dokument3 SeitenBag Technique Checklists CHN 1 (SL)Krisa AdornaNoch keine Bewertungen
- Competency Checklist Apical and Radial PulseDokument2 SeitenCompetency Checklist Apical and Radial PulseJobelle AcenaNoch keine Bewertungen
- Adventist University of The Philippines: Urinary Cathetirization P RIS RemarksDokument2 SeitenAdventist University of The Philippines: Urinary Cathetirization P RIS RemarksAnnie AlbertoNoch keine Bewertungen
- BS Nursing Program OutcomesDokument20 SeitenBS Nursing Program Outcomesۦۦ JamesNoch keine Bewertungen
- Essential Intrapartum and Newborn CareDokument37 SeitenEssential Intrapartum and Newborn CareVenice s SantosNoch keine Bewertungen
- Wound Care Procedure StudentsDokument2 SeitenWound Care Procedure StudentsJan Philippe BelandoNoch keine Bewertungen
- Steps in Essential Newborn CareDokument12 SeitenSteps in Essential Newborn CareCedy L. CieloNoch keine Bewertungen
- Wound CareDokument3 SeitenWound CaregrangerhermionepNoch keine Bewertungen
- Applying Restraint Nursing SkillDokument2 SeitenApplying Restraint Nursing SkillEiichiro BertoNoch keine Bewertungen
- Administering Pulse OxDokument2 SeitenAdministering Pulse OxjepoiNoch keine Bewertungen
- Perineal CareDokument3 SeitenPerineal CareNikko Rafael RobillosNoch keine Bewertungen
- Immediate Care of The NewbornDokument8 SeitenImmediate Care of The NewbornksjsellsNoch keine Bewertungen
- High Risk PregnancyDokument10 SeitenHigh Risk PregnancyRoy Mujeres CabueñasNoch keine Bewertungen
- Case Analysis RLE MODULE TEMPLATE Nursery 1 (One)Dokument7 SeitenCase Analysis RLE MODULE TEMPLATE Nursery 1 (One)PanJan BalNoch keine Bewertungen
- Topical skin procedure checklistDokument5 SeitenTopical skin procedure checklistpramod kumawatNoch keine Bewertungen
- Name: - Date Performed: - Year & SectionDokument1 SeiteName: - Date Performed: - Year & SectionFrancis GongNoch keine Bewertungen
- CMC 5 Foley Catheter Insertion ProcedureDokument6 SeitenCMC 5 Foley Catheter Insertion ProcedureRosevick BadocoNoch keine Bewertungen
- Nursing RLEDokument19 SeitenNursing RLEPatricia AdiaoNoch keine Bewertungen
- NGT LavageDokument2 SeitenNGT LavageAngela Joy AmparadoNoch keine Bewertungen
- Pengaruh Edukasi Terhadap Pengetahuan, Pola Makan Dan Kadar Glukosa DarahDokument8 SeitenPengaruh Edukasi Terhadap Pengetahuan, Pola Makan Dan Kadar Glukosa DarahIchy Rizki Abdul GaniNoch keine Bewertungen
- Pedoman Diet Diabetes MelitusDokument45 SeitenPedoman Diet Diabetes Melitus51limasatuNoch keine Bewertungen
- Diabetes Mellitus 1Dokument35 SeitenDiabetes Mellitus 1Delfi ratnaNoch keine Bewertungen
- 233 130 1 PBDokument8 Seiten233 130 1 PBari_julian94Noch keine Bewertungen
- Jurnal KesehatanDokument12 SeitenJurnal KesehatanRizqi Puji LestariNoch keine Bewertungen
- Fundamentals Nursing Active Learning 1st Edition Yoost Crawford - Test BankDokument44 SeitenFundamentals Nursing Active Learning 1st Edition Yoost Crawford - Test BankRaymondCenteno100% (3)
- 05 Abpg2103 Topic 1Dokument14 Seiten05 Abpg2103 Topic 1Ummu SolihahNoch keine Bewertungen
- NURS FPX 6614 Assessment 3 Disseminating The Evidence Scholarly Video Media SubmissionDokument7 SeitenNURS FPX 6614 Assessment 3 Disseminating The Evidence Scholarly Video Media SubmissionEmma WatsonNoch keine Bewertungen
- PRC Cases FormDokument5 SeitenPRC Cases FormtwothumbsNoch keine Bewertungen
- Large Hospital SystemsDokument732 SeitenLarge Hospital SystemsMutai JoseahNoch keine Bewertungen
- MRI Scanning and OrthodonticsDokument7 SeitenMRI Scanning and OrthodonticsAmit SagarNoch keine Bewertungen
- Diabetes Mellitus (Case Study)Dokument13 SeitenDiabetes Mellitus (Case Study)Narie TungpalanNoch keine Bewertungen
- Protective Stabilization For Pediatric Dental PatientsDokument6 SeitenProtective Stabilization For Pediatric Dental Patientsangela faustinaNoch keine Bewertungen
- CACVS2016 AbstractBookDokument100 SeitenCACVS2016 AbstractBookChuk IfeanyiNoch keine Bewertungen
- Hemolytic AnemiaDokument6 SeitenHemolytic AnemiaLupita Yessica Tarigan0% (1)
- Gestational Diabetes Brochure ENGDokument2 SeitenGestational Diabetes Brochure ENGP Zamora100% (2)
- 16th Lect Physical Therapy ModalitiesDokument46 Seiten16th Lect Physical Therapy ModalitiesPrincess Faye Tiongson ChavezNoch keine Bewertungen
- Fundamentals of Nursing Exam 2 (50 Items)Dokument17 SeitenFundamentals of Nursing Exam 2 (50 Items)TamiyaPhil100% (2)
- Academic Reading SampleDokument5 SeitenAcademic Reading SampleYosefOriolNoch keine Bewertungen
- Esthetic DentistryDokument346 SeitenEsthetic Dentistryreered100% (3)
- Maralgia ParastheticaDokument7 SeitenMaralgia ParastheticaShahazad ShaikNoch keine Bewertungen
- Faecal Incontinence in Adults - ReviewDokument12 SeitenFaecal Incontinence in Adults - Reviewi can always make u smile :DNoch keine Bewertungen
- Validity of The FOUR Score Coma Scale in The Medical Intensive Care Unit 2009 PDFDokument8 SeitenValidity of The FOUR Score Coma Scale in The Medical Intensive Care Unit 2009 PDFlithium2203Noch keine Bewertungen
- Nandita Sundarapandian ResumeDokument3 SeitenNandita Sundarapandian Resumeapi-334305820Noch keine Bewertungen
- IM ShelfDokument100 SeitenIM Shelfomarmd21Noch keine Bewertungen
- The Utah STEMI SystemDokument4 SeitenThe Utah STEMI SystemState of UtahNoch keine Bewertungen
- Philips Achieva 3.0T TXDokument14 SeitenPhilips Achieva 3.0T TXLate ArtistNoch keine Bewertungen
- Procedure Competency Assessment Tool - Slit Lamp ExaminationDokument2 SeitenProcedure Competency Assessment Tool - Slit Lamp ExaminationAmeng GosimNoch keine Bewertungen
- Controversial Developments in MedicineDokument7 SeitenControversial Developments in MedicineEvan HawthorneNoch keine Bewertungen
- MS ISO 15189 Medical Lab AccreditationDokument19 SeitenMS ISO 15189 Medical Lab Accreditationmzaim100% (1)
- DDH Diagnosis and Treatment in 8-Week-Old InfantDokument5 SeitenDDH Diagnosis and Treatment in 8-Week-Old InfantMavra zNoch keine Bewertungen
- Thoracic Trauma TreatmentDokument77 SeitenThoracic Trauma TreatmentAnonymous GsvDOlQuSNoch keine Bewertungen
- Bupa International Claim Form: 1 Patient'S DetailsDokument4 SeitenBupa International Claim Form: 1 Patient'S DetailsRealty SolutionsNoch keine Bewertungen
- FDA Briefing Book - TOBIDokument135 SeitenFDA Briefing Book - TOBISnigdha Santra SaxenaNoch keine Bewertungen
- MCQ RespiratoryDokument15 SeitenMCQ Respiratoryanaphysioforyou100% (1)