Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Drug StudyDokument34 SeitenDrug StudyMarco MoralesNoch keine Bewertungen
- MCN Review NotesDokument141 SeitenMCN Review NotesMelrose Saludares SumugatNoch keine Bewertungen
- YAWAADokument10 SeitenYAWAAZyrene CapulongNoch keine Bewertungen
- Myoma Final Power PointDokument45 SeitenMyoma Final Power Pointicesexy100% (1)
- E Cart DrugsDokument2 SeitenE Cart DrugsxmitchxNoch keine Bewertungen
- Drug Study - Nalbuphine (Nubain)Dokument3 SeitenDrug Study - Nalbuphine (Nubain)Maria Theresa BuscasNoch keine Bewertungen
- Concept Of: (The Fifth Vital Sign)Dokument43 SeitenConcept Of: (The Fifth Vital Sign)Mae DacerNoch keine Bewertungen
- Lecture 2 Opoid Analgesics PDFDokument12 SeitenLecture 2 Opoid Analgesics PDFAbdelrahman WaelNoch keine Bewertungen
- Scenario Flow and ScriptDokument6 SeitenScenario Flow and ScriptJhoneric Vencer EscultorNoch keine Bewertungen
- Acute Appendicitis With Down SyndromeDokument88 SeitenAcute Appendicitis With Down SyndromeVinzii DrtNoch keine Bewertungen
- Nalbuphine HydrochlorideDokument6 SeitenNalbuphine HydrochlorideMarie Therese Montaño Subong100% (1)
- DRUG STUDY - Nalbuphine HydrochlorideDokument2 SeitenDRUG STUDY - Nalbuphine HydrochlorideCarson BirthNoch keine Bewertungen
- 13-Opioids Lecture 1Dokument41 Seiten13-Opioids Lecture 1api-343631539100% (1)
- K10 Opioid AnalgesicsDokument30 SeitenK10 Opioid AnalgesicsLa Lydia TampubolonNoch keine Bewertungen
- Or Drug StudyDokument7 SeitenOr Drug StudyNikki M. ArapolNoch keine Bewertungen
- Drug StudyDokument12 SeitenDrug StudyAnne Marie Angelica BilonoNoch keine Bewertungen
- Pain Relief in Labour (English)Dokument60 SeitenPain Relief in Labour (English)lieynna4996100% (2)
- Drug Study CSDokument7 SeitenDrug Study CSFrancis MendozaNoch keine Bewertungen
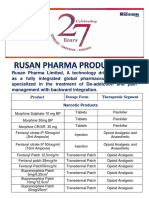
- Rusan Pharma Product ListDokument4 SeitenRusan Pharma Product ListSanjay SharmaNoch keine Bewertungen
- Drug Study Celecoxib NubainDokument4 SeitenDrug Study Celecoxib NubainMaiko TyNoch keine Bewertungen
- Common DrugsDokument15 SeitenCommon DrugsKate Penelope DalidNoch keine Bewertungen
- Week 6 - Antiparkinsonism AgentsDokument18 SeitenWeek 6 - Antiparkinsonism AgentsDino MicaNoch keine Bewertungen
- Drug StudyDokument9 SeitenDrug StudyJeanette Leigh BravoNoch keine Bewertungen
- NCP 1Dokument7 SeitenNCP 1Roldan VidadNoch keine Bewertungen
- Rafin NCP and Drug StudyDokument7 SeitenRafin NCP and Drug StudyCezanne CruzNoch keine Bewertungen
- Discussed PharmaDokument6 SeitenDiscussed PharmaNataly AlbannaNoch keine Bewertungen
- Drug StudyDokument13 SeitenDrug StudyGi Ey ElNoch keine Bewertungen
- Hemorrhagic Cerebro Vascular DiseaseDokument37 SeitenHemorrhagic Cerebro Vascular Diseasejbvaldez100% (1)
- Week 06 - Antiparkinsonism AgentsDokument18 SeitenWeek 06 - Antiparkinsonism AgentsDino MicaNoch keine Bewertungen
- NAVLE Anesthetic Pharmacology Review 2018 PDFDokument63 SeitenNAVLE Anesthetic Pharmacology Review 2018 PDFmmatthew74Noch keine Bewertungen