Das könnte Ihnen auch gefallen
- Comprehensive Geriatric AssessmentDokument26 SeitenComprehensive Geriatric AssessmentGoddy Manzano100% (1)
- Assessing Older Adults' Health and FunctioningDokument11 SeitenAssessing Older Adults' Health and FunctioningJordan Abosama MamalumpongNoch keine Bewertungen
- Nursing Assessment of Older AdultsDokument6 SeitenNursing Assessment of Older AdultsMatthew RayburnNoch keine Bewertungen
- Comprehensive Geriatric AssessmentDokument25 SeitenComprehensive Geriatric Assessmentsantosestrella100% (6)
- Geri Assess Tools ArticleDokument9 SeitenGeri Assess Tools ArticleThesmith FamNoch keine Bewertungen
- Geriatric Assessment Aids Diagnosis, Treatment Planning for Older AdultsDokument4 SeitenGeriatric Assessment Aids Diagnosis, Treatment Planning for Older Adultsaila angNoch keine Bewertungen
- Comprehensive: Geriatric AssessmentDokument38 SeitenComprehensive: Geriatric AssessmentDingsNoch keine Bewertungen
- Health Psych: MSE for Chronic IllnessDokument19 SeitenHealth Psych: MSE for Chronic IllnessYashika Jain -63Noch keine Bewertungen
- Assessment of Older AdultsDokument34 SeitenAssessment of Older AdultsStephanie Mhae TabasaNoch keine Bewertungen
- Family Nursing Care Plan A, D, PDokument44 SeitenFamily Nursing Care Plan A, D, PYuunaFuentesLegaspiNoch keine Bewertungen
- Comprehensive Geriatric Assessment: by Dr. Zinab AlatawiDokument37 SeitenComprehensive Geriatric Assessment: by Dr. Zinab AlatawiOne life To live SaudiahNoch keine Bewertungen
- Nursing Process in Psychiatric Unit - 3Dokument138 SeitenNursing Process in Psychiatric Unit - 3Lina DsouzaNoch keine Bewertungen
- The Nursing Process in Psychiatric/Mental Health Nursing: PlanningDokument49 SeitenThe Nursing Process in Psychiatric/Mental Health Nursing: PlanningJonalynCollodChewacheo50% (2)
- Assessment Is Making Assumptions. When You See It, You Attach It ToDokument18 SeitenAssessment Is Making Assumptions. When You See It, You Attach It ToDonn Patrick AlegreNoch keine Bewertungen
- Care of the Older Adult: Effective Communication and AssessmentDokument67 SeitenCare of the Older Adult: Effective Communication and AssessmentShazich Keith Lacbay100% (1)
- Geriatric AssessmentDokument27 SeitenGeriatric AssessmentNeil Philip MaturanNoch keine Bewertungen
- Module 3 - Assessment of The Health StatusDokument43 SeitenModule 3 - Assessment of The Health StatusAYTONA, JAMAICA F.Noch keine Bewertungen
- 006 Chapter 4 Clinical AssessmentDokument12 Seiten006 Chapter 4 Clinical AssessmentMary Ann Bautista PerladoNoch keine Bewertungen
- HEALTH ASSESSMENT and Its ImportanceDokument9 SeitenHEALTH ASSESSMENT and Its ImportanceJayita Gayen DuttaNoch keine Bewertungen
- Geriatrics Screening and AssessmentDokument12 SeitenGeriatrics Screening and AssessmentMagdalena Contardo CisternasNoch keine Bewertungen
- Family Nursing Process - 1Dokument14 SeitenFamily Nursing Process - 1Reese TañedoNoch keine Bewertungen
- Introduction to Health AssessmentDokument8 SeitenIntroduction to Health AssessmentHung PhanNoch keine Bewertungen
- MENTAL HEALTH NURSING STANDARDSDokument33 SeitenMENTAL HEALTH NURSING STANDARDSSANU RAMASWAMY100% (1)
- Nursing Health Assessment: Akram Mohammad Abusalah BNS, MSN, Ph. D. Islamic University of Gaza StripDokument262 SeitenNursing Health Assessment: Akram Mohammad Abusalah BNS, MSN, Ph. D. Islamic University of Gaza StripBheru LalNoch keine Bewertungen
- Presentation Family Health Nursing Process - Assessment Ver 2-1Dokument75 SeitenPresentation Family Health Nursing Process - Assessment Ver 2-1Elesis samaNoch keine Bewertungen
- Introduction To Psychological Assessment and PsychodiagnosisDokument75 SeitenIntroduction To Psychological Assessment and PsychodiagnosisNishesh AcharyaNoch keine Bewertungen
- Geriatric Nursing MidtermDokument67 SeitenGeriatric Nursing MidtermMadeline N. Gerzon100% (2)
- Geriatric Assessment ToolsDokument51 SeitenGeriatric Assessment ToolsKayoo_167% (3)
- Assessment of The Health Status of Older PersonsDokument50 SeitenAssessment of The Health Status of Older PersonsKim GarciaNoch keine Bewertungen
- Health AppraisalDokument22 SeitenHealth AppraisalCharlene Fadrigon-OtazuNoch keine Bewertungen
- Psychosocial NursingDokument21 SeitenPsychosocial NursingAngeline AngelesNoch keine Bewertungen
- Dementia Outcomes Care Plan ToolDokument67 SeitenDementia Outcomes Care Plan ToolDanut GorganNoch keine Bewertungen
- Realosa PresentationDokument14 SeitenRealosa PresentationSharalyn SiaNoch keine Bewertungen
- Running Head: Effectiveness of Dementia Inteventions 1Dokument12 SeitenRunning Head: Effectiveness of Dementia Inteventions 1John Mureithi NjugunaNoch keine Bewertungen
- Principles of GeriatricsDokument12 SeitenPrinciples of GeriatricsEveryday LearnerNoch keine Bewertungen
- Clinical Interview and ObservationDokument47 SeitenClinical Interview and Observationmlssmnn100% (1)
- Comprehensive Assessment: The Keys To Unlocking The Mystery of AssessmentDokument162 SeitenComprehensive Assessment: The Keys To Unlocking The Mystery of AssessmentSuganya BalachandranNoch keine Bewertungen
- Comprehensive Geriatric AssessmentDokument6 SeitenComprehensive Geriatric AssessmentAnne Laureta100% (1)
- Chapter 06Dokument7 SeitenChapter 06loveteddybear0% (2)
- Learning How To Live Life Is The Best Thing You Can Give YourselfDokument15 SeitenLearning How To Live Life Is The Best Thing You Can Give YourselfCiedelle Honey Lou DimaligNoch keine Bewertungen
- CognitiveDokument19 SeitenCognitiveLaila MajenumNoch keine Bewertungen
- Measures The Status of The FamilyDokument7 SeitenMeasures The Status of The FamilyKitkat Aquino Cabugwas100% (1)
- CHN - LAB - Family Health NursingDokument9 SeitenCHN - LAB - Family Health NursingRaynelah AnnNoch keine Bewertungen
- Family Health Nursing ProcessDokument31 SeitenFamily Health Nursing ProcessReniella HidalgoNoch keine Bewertungen
- Family Health Nursing Process GuideDokument25 SeitenFamily Health Nursing Process GuideLovely OxemerNoch keine Bewertungen
- Nursing Assessment Process: A Comprehensive GuideDokument22 SeitenNursing Assessment Process: A Comprehensive GuideNami Castañas Dela CalzadaNoch keine Bewertungen
- Assessment of Older Person With Focus On FunctionDokument18 SeitenAssessment of Older Person With Focus On FunctionMAE DEVILLANoch keine Bewertungen
- Comprehensive Geriatric AssessmentDokument87 SeitenComprehensive Geriatric AssessmentNurrahmanita AzizaNoch keine Bewertungen
- Assessment in Geriatric PatientsDokument14 SeitenAssessment in Geriatric Patientsنور حسليندا اسحاقNoch keine Bewertungen
- Nursing Process in Psychiatric NursingDokument14 SeitenNursing Process in Psychiatric NursingJomark Palgan100% (1)
- Chapter5Dokument42 SeitenChapter5peachypeachyNoch keine Bewertungen
- Gordon's Functional Health PatternsDokument10 SeitenGordon's Functional Health Patternsakoeljames8543Noch keine Bewertungen
- Geriatric AssessmentDokument5 SeitenGeriatric AssessmentP.Senthil SelvamNoch keine Bewertungen
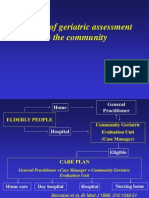
- The Use of Geriatric Assessment in The CommunityDokument16 SeitenThe Use of Geriatric Assessment in The Communityhendra2darmawanNoch keine Bewertungen
- Comprehensive Geriatric Assessment (Cga) by Dr. Monday J. Zaccheaus NewDokument55 SeitenComprehensive Geriatric Assessment (Cga) by Dr. Monday J. Zaccheaus NewDr. Amb. Monday ZaccheausNoch keine Bewertungen
- Children's Medication Toolbox: Managing, Monitoring and Improving Your Child's Response to MedicationVon EverandChildren's Medication Toolbox: Managing, Monitoring and Improving Your Child's Response to MedicationNoch keine Bewertungen
- Physician Assistant PANCE & PANRE: a QuickStudy Laminated Reference GuideVon EverandPhysician Assistant PANCE & PANRE: a QuickStudy Laminated Reference GuideNoch keine Bewertungen
- Case Illustration of Professional Ethics & Psychotherapy Case StudiesVon EverandCase Illustration of Professional Ethics & Psychotherapy Case StudiesNoch keine Bewertungen
- Therapist's Guide to Pediatric Affect and Behavior RegulationVon EverandTherapist's Guide to Pediatric Affect and Behavior RegulationNoch keine Bewertungen
- Nutritional Counselling. How To Motivate People To Correct Their Eating HabitsVon EverandNutritional Counselling. How To Motivate People To Correct Their Eating HabitsNoch keine Bewertungen
- Pediatric Nursing Care Plans and Assessment QuestionsDokument13 SeitenPediatric Nursing Care Plans and Assessment QuestionsSteffi MurielNoch keine Bewertungen
- Pathophysiology of Chronic Kidney Disease (CKDDokument5 SeitenPathophysiology of Chronic Kidney Disease (CKDSteffi MurielNoch keine Bewertungen
- Hi! We Will Top The Nursing Licensure Board Exam!!! Claim It!Dokument1 SeiteHi! We Will Top The Nursing Licensure Board Exam!!! Claim It!Steffi MurielNoch keine Bewertungen
- CCUDokument5 SeitenCCUSteffi MurielNoch keine Bewertungen
- Drug Study NccuDokument2 SeitenDrug Study NccuSteffi MurielNoch keine Bewertungen
- Ca2 HW1Dokument1 SeiteCa2 HW1Steffi MurielNoch keine Bewertungen
- Pathophysiology of Atherosclerosis and Myocardial InfarctionDokument2 SeitenPathophysiology of Atherosclerosis and Myocardial InfarctionSteffi MurielNoch keine Bewertungen
- Pathophysiology of Atherosclerosis and Myocardial InfarctionDokument2 SeitenPathophysiology of Atherosclerosis and Myocardial InfarctionSteffi MurielNoch keine Bewertungen
- Ccu - CaseanaDokument17 SeitenCcu - CaseanaSteffi MurielNoch keine Bewertungen
- Ccu Patho AcsDokument2 SeitenCcu Patho AcsSteffi MurielNoch keine Bewertungen
- CCUDokument6 SeitenCCUSteffi MurielNoch keine Bewertungen
- Nursing Care Plan for Hypokalemia and AnemiaDokument3 SeitenNursing Care Plan for Hypokalemia and AnemiaSteffi MurielNoch keine Bewertungen
- Drugs MOA I & Ci Se & Ar Nursing Considerations Generic: Indications:-CnsDokument7 SeitenDrugs MOA I & Ci Se & Ar Nursing Considerations Generic: Indications:-CnsSteffi MurielNoch keine Bewertungen
- A. Demographic: Patient's ProfileDokument2 SeitenA. Demographic: Patient's ProfileSteffi MurielNoch keine Bewertungen
- DRUGsssDokument2 SeitenDRUGsssSteffi MurielNoch keine Bewertungen
- Why Autism HappensDokument12 SeitenWhy Autism HappensSteffi MurielNoch keine Bewertungen
- CellulitisDokument1 SeiteCellulitisSteffi MurielNoch keine Bewertungen
- Case 20-2016Dokument20 SeitenCase 20-2016Steffi MurielNoch keine Bewertungen
- 3 NCP Ineffective Tissue PerfusionDokument2 Seiten3 NCP Ineffective Tissue PerfusionSteffi MurielNoch keine Bewertungen
- Chest Imaging Case Study of Persistent Pleural EffusionDokument2 SeitenChest Imaging Case Study of Persistent Pleural EffusionSteffi MurielNoch keine Bewertungen
- Assessment Nursing Diagnosis Nursing InterventionDokument2 SeitenAssessment Nursing Diagnosis Nursing InterventionSteffi MurielNoch keine Bewertungen
- Case 20-2016Dokument20 SeitenCase 20-2016Steffi MurielNoch keine Bewertungen
- End-Stage Renal Disease Case PresentationDokument2 SeitenEnd-Stage Renal Disease Case PresentationSteffi MurielNoch keine Bewertungen
- Patient's Profile A Demographic DataDokument2 SeitenPatient's Profile A Demographic DataSteffi MurielNoch keine Bewertungen
- Top 3 References for Job ApplicationDokument1 SeiteTop 3 References for Job ApplicationSteffi MurielNoch keine Bewertungen
- Case 21Dokument3 SeitenCase 21Steffi MurielNoch keine Bewertungen
- 20 NCP Impaired Skin IntegrityDokument4 Seiten20 NCP Impaired Skin IntegritySteffi MurielNoch keine Bewertungen
- 32-Year-Old Man in Unresponsive State With Liver FailureDokument2 Seiten32-Year-Old Man in Unresponsive State With Liver FailureSteffi MurielNoch keine Bewertungen
- Complications of IV TherapyDokument10 SeitenComplications of IV TherapySteffi MurielNoch keine Bewertungen
- 32-Year-Old Man in Unresponsive State With Liver FailureDokument2 Seiten32-Year-Old Man in Unresponsive State With Liver FailureSteffi MurielNoch keine Bewertungen
- Fy20 RedresourcedirectoryDokument70 SeitenFy20 Redresourcedirectoryapi-351984804Noch keine Bewertungen
- Speck - Spiritual Care in Health CareDokument6 SeitenSpeck - Spiritual Care in Health Caremasmicko07Noch keine Bewertungen
- Principles of Pain AssessmentDokument9 SeitenPrinciples of Pain AssessmentNDJNoch keine Bewertungen
- Ethics Committee Resignation LetterDokument3 SeitenEthics Committee Resignation LetterCVRecordNoch keine Bewertungen
- Palliative Care of Stomach CancerDokument16 SeitenPalliative Care of Stomach Cancerurmila prajapatiNoch keine Bewertungen
- 2016 EdBookDokument931 Seiten2016 EdBookvarun7189100% (1)
- Helping Tree DigbyDokument1 SeiteHelping Tree Digbyapi-287789123Noch keine Bewertungen
- Eng 1010 Final Informative Research Paper 2Dokument7 SeitenEng 1010 Final Informative Research Paper 2api-317626858Noch keine Bewertungen
- Delgado Guay (2015)Dokument7 SeitenDelgado Guay (2015)Aprilla Ayu WulandariNoch keine Bewertungen
- Providing palliative care guidance for COVID-19 pandemicDokument3 SeitenProviding palliative care guidance for COVID-19 pandemicIndiara MartinsNoch keine Bewertungen
- 114 Week 6 PPT Narrative GabuleDokument2 Seiten114 Week 6 PPT Narrative GabuleDudil GoatNoch keine Bewertungen
- Women & CancerDokument23 SeitenWomen & CancerSri PurwatiningsihNoch keine Bewertungen
- Burdens of Family Caregiving at The End of LifeDokument6 SeitenBurdens of Family Caregiving at The End of LifeNurul ShahirahNoch keine Bewertungen
- Encyclopedia of Cancer PDFDokument461 SeitenEncyclopedia of Cancer PDFBachtiar Muhammad ArifNoch keine Bewertungen
- Erona Ress: Teaching The TeachersDokument16 SeitenErona Ress: Teaching The TeachersAnonymous 9eadjPSJNgNoch keine Bewertungen
- Clinical Supervision: A Structured Approach To Best PracticeDokument17 SeitenClinical Supervision: A Structured Approach To Best PracticeChandra_riauNoch keine Bewertungen
- Chapter 36 Death Study GuideDokument25 SeitenChapter 36 Death Study GuideDaniel McVayNoch keine Bewertungen
- End of Life Care PPPDokument43 SeitenEnd of Life Care PPPElaine SUNoch keine Bewertungen
- Topic 1: © Aspire Training & ConsultingDokument20 SeitenTopic 1: © Aspire Training & ConsultingMashael SulimanNoch keine Bewertungen
- Deconstructing Death: Using Mindfulness To Manage Life's Ultimate TransitionDokument27 SeitenDeconstructing Death: Using Mindfulness To Manage Life's Ultimate TransitionMarco0115Noch keine Bewertungen
- Patient-Centered Care: Case Studies On End of Life: AP HCH C ' NDokument9 SeitenPatient-Centered Care: Case Studies On End of Life: AP HCH C ' NastriNoch keine Bewertungen
- Patient Admission Hospital Admission ChecklistDokument6 SeitenPatient Admission Hospital Admission ChecklistSweetly MamukoNoch keine Bewertungen
- Honey Wounds CancerDokument6 SeitenHoney Wounds CancerburhanNoch keine Bewertungen
- End-of-life care nursing values and ethicsDokument7 SeitenEnd-of-life care nursing values and ethicsRM DemetilloNoch keine Bewertungen
- Rundown AcaraDokument3 SeitenRundown Acaradedy nurmantoroNoch keine Bewertungen
- MBBS Curriculum 2019Dokument330 SeitenMBBS Curriculum 2019childicuNoch keine Bewertungen
- Social Workers in Hospice and Palliative Care: Occupational ProfileDokument10 SeitenSocial Workers in Hospice and Palliative Care: Occupational ProfileCharu JainNoch keine Bewertungen
- Compliance Audit ToolDokument11 SeitenCompliance Audit TooljhonronNoch keine Bewertungen
- Colon Ca Case Study For Ring BoundDokument66 SeitenColon Ca Case Study For Ring BoundMary EnsomoNoch keine Bewertungen
- Core Competency Domain Three: Interprofessional CommunicationDokument5 SeitenCore Competency Domain Three: Interprofessional CommunicationwdyafrmaNoch keine Bewertungen