Das könnte Ihnen auch gefallen
- Upper and Lower GI Bleeding Differential DiagnosesDokument3 SeitenUpper and Lower GI Bleeding Differential DiagnosesKEn PilapilNoch keine Bewertungen
- Past Years SNQ Answer by RCSIDokument47 SeitenPast Years SNQ Answer by RCSIhelamahjoubmounirdmo100% (1)
- Core Topics in Internal MedicineDokument4 SeitenCore Topics in Internal MedicineKristina Anne CoNoch keine Bewertungen
- Prepared by Inzar Yasin Ammar LabibDokument47 SeitenPrepared by Inzar Yasin Ammar LabibJohn Clements Galiza100% (1)
- Torsade De Pointes, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandTorsade De Pointes, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- Dyspnea PresentationDokument37 SeitenDyspnea PresentationamgoperaNoch keine Bewertungen
- Critical Care in PregnancyDokument21 SeitenCritical Care in PregnancyamuzaNoch keine Bewertungen
- Problem-based Approach to Gastroenterology and HepatologyVon EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNoch keine Bewertungen
- PericarditisDokument29 SeitenPericarditisPavin KumarNoch keine Bewertungen
- Hypertensive Emergencies in The Emergency DepartmentDokument13 SeitenHypertensive Emergencies in The Emergency DepartmentLuis Lopez RevelesNoch keine Bewertungen
- MCQDokument33 SeitenMCQSean Purrier50% (2)
- Acute Stroke ManagementDokument8 SeitenAcute Stroke ManagementГурам ЧахвадзеNoch keine Bewertungen
- Newborn EmergenciesDokument83 SeitenNewborn EmergencieshwelpNoch keine Bewertungen
- Notes On History Taking in The Cardiovascular SystemDokument9 SeitenNotes On History Taking in The Cardiovascular Systemmdjohar72100% (1)
- Brain AbscessDokument25 SeitenBrain AbscessprembarnabasNoch keine Bewertungen
- Mohammed Gogandy - Puerperium History Sheet & - 40 2007-2008& - 41 PDFDokument2 SeitenMohammed Gogandy - Puerperium History Sheet & - 40 2007-2008& - 41 PDFJennifer Ross-ComptisNoch keine Bewertungen
- Pericardial DiseaseDokument59 SeitenPericardial DiseaseGunawan Yoga100% (1)
- SABER IM PrometricDokument71 SeitenSABER IM Prometricisra zaidNoch keine Bewertungen
- Hemoptysis - Case Presentation and DiscussionDokument52 SeitenHemoptysis - Case Presentation and DiscussionPGHC100% (1)
- Vasopressors in ShockDokument8 SeitenVasopressors in ShockOrion JohnNoch keine Bewertungen
- Venous ThromboembolismDokument49 SeitenVenous Thromboembolismadamu mohammadNoch keine Bewertungen
- Hypertensive CrisisDokument28 SeitenHypertensive CrisisJacob Alexander MarpaungNoch keine Bewertungen
- ECG Interpretation DR - Rawan AlshreemDokument25 SeitenECG Interpretation DR - Rawan AlshreemMarymii Al-sahlawiiNoch keine Bewertungen
- Anemia in ChildrenDokument9 SeitenAnemia in ChildrenVillegas Sepúlveda AbrahamNoch keine Bewertungen
- Red Eye Poster HiresDokument1 SeiteRed Eye Poster HiresAndrew CheongNoch keine Bewertungen
- NeonatologyDokument4 SeitenNeonatologyteslimolakunleraji100% (1)
- Common Histories and Red Flags Presentation Noninteractive VersionDokument21 SeitenCommon Histories and Red Flags Presentation Noninteractive VersionesmarNoch keine Bewertungen
- Amboss Hemolytic AnemiaDokument16 SeitenAmboss Hemolytic AnemiaAhmed Ali100% (2)
- Approach To TruamaDokument29 SeitenApproach To TruamaIbsa ShumaNoch keine Bewertungen
- Approach To Septic ShockDokument16 SeitenApproach To Septic ShockRaja EllysyaNoch keine Bewertungen
- 58 Cases History and Physical Exam BookDokument102 Seiten58 Cases History and Physical Exam BookeleazarmdNoch keine Bewertungen
- Sudden Maternal Collapse: Max Brinsmead MB Bs PHD May 2015Dokument23 SeitenSudden Maternal Collapse: Max Brinsmead MB Bs PHD May 2015DrChauhanNoch keine Bewertungen
- ThyroidDokument49 SeitenThyroidAbeer RadiNoch keine Bewertungen
- Pericarditis 65 SlidesDokument65 SeitenPericarditis 65 SlidesAtifBhoreNoch keine Bewertungen
- CardiomyopathyDokument17 SeitenCardiomyopathysarguss1450% (2)
- Oscesbook 1Dokument38 SeitenOscesbook 1PasTestBooks100% (1)
- SYLLABUS Internal Medicine Junior ClerkshipDokument15 SeitenSYLLABUS Internal Medicine Junior ClerkshipAloah122346Noch keine Bewertungen
- HX TakingDokument37 SeitenHX TakingAya SalahNoch keine Bewertungen
- Upper GIT BleedingDokument69 SeitenUpper GIT BleedingSoleh Ramly100% (1)
- Clinical ExDokument123 SeitenClinical ExDeepti ChaharNoch keine Bewertungen
- MEDICALLY COMPROMISED Patients in Orthodontics / Orthodontic Courses by Indian Dental AcademyDokument107 SeitenMEDICALLY COMPROMISED Patients in Orthodontics / Orthodontic Courses by Indian Dental Academyindian dental academyNoch keine Bewertungen
- Internal Medicine Sample Osce Examination Component Questions eDokument2 SeitenInternal Medicine Sample Osce Examination Component Questions eFajar ChampionNoch keine Bewertungen
- History and ExaminationDokument6 SeitenHistory and ExaminationQuartz_usuNoch keine Bewertungen
- CopdDokument35 SeitenCopdNurhidayahNoch keine Bewertungen
- OSCE - Chest PainDokument2 SeitenOSCE - Chest PaincgalongNoch keine Bewertungen
- RCSI Clinical Examinations in Medicine 2018-19Dokument189 SeitenRCSI Clinical Examinations in Medicine 2018-19Rebecca MarshallNoch keine Bewertungen
- Past Paper (No Answer)Dokument170 SeitenPast Paper (No Answer)Hariharan NarendranNoch keine Bewertungen
- Preparing For The Prescribing Safety AssessmentDokument36 SeitenPreparing For The Prescribing Safety AssessmentChAndrewNoch keine Bewertungen
- Transfusion-Related Acute Lung Injury (TRALI)Dokument20 SeitenTransfusion-Related Acute Lung Injury (TRALI)WilliamRayCassidyNoch keine Bewertungen
- PediatricsDokument321 SeitenPediatricsAlenaNoch keine Bewertungen
- CardiologyDokument6 SeitenCardiologyFrancis FransNoch keine Bewertungen
- Murmur EvaluationDokument4 SeitenMurmur EvaluationManjunath GeminiNoch keine Bewertungen
- Hypertrophic CardiomyopathyDokument57 SeitenHypertrophic CardiomyopathycynNoch keine Bewertungen
- Rheumatic Heart Disease AustrliaDokument63 SeitenRheumatic Heart Disease AustrliaMuhammad Reza100% (2)
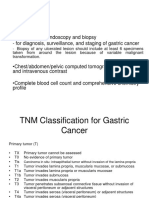
- Workup:: - Upper GI Tract Endoscopy and Biopsy - For Diagnosis, Surveillance, and Staging of Gastric CancerDokument3 SeitenWorkup:: - Upper GI Tract Endoscopy and Biopsy - For Diagnosis, Surveillance, and Staging of Gastric CancermmmalcampoNoch keine Bewertungen
- Adult VitalsDokument5 SeitenAdult VitalsmmmalcampoNoch keine Bewertungen
- Disease/Infection Etiologic Agent Incubatio N Period Rash Pattern/ Occurence Assoc. S/S TreatmentDokument10 SeitenDisease/Infection Etiologic Agent Incubatio N Period Rash Pattern/ Occurence Assoc. S/S TreatmentmmmalcampoNoch keine Bewertungen
- Osce-Hema 2Dokument5 SeitenOsce-Hema 2mmmalcampoNoch keine Bewertungen
- Solubility Product ConstantsDokument6 SeitenSolubility Product ConstantsBilal AhmedNoch keine Bewertungen
- CSE 202.04 Inspection of Concrete StructuresDokument67 SeitenCSE 202.04 Inspection of Concrete StructuresJellyn BaseNoch keine Bewertungen
- Curriculum Guide Ay 2021-2022: Dr. Gloria Lacson Foundation Colleges, IncDokument9 SeitenCurriculum Guide Ay 2021-2022: Dr. Gloria Lacson Foundation Colleges, IncJean Marie Itang GarciaNoch keine Bewertungen
- UM-140-D00221-07 SeaTrac Developer Guide (Firmware v2.4)Dokument154 SeitenUM-140-D00221-07 SeaTrac Developer Guide (Firmware v2.4)Antony Jacob AshishNoch keine Bewertungen
- Agency Canvas Ing PresentationDokument27 SeitenAgency Canvas Ing Presentationkhushi jaiswalNoch keine Bewertungen
- BLP#1 - Assessment of Community Initiative (3 Files Merged)Dokument10 SeitenBLP#1 - Assessment of Community Initiative (3 Files Merged)John Gladhimer CanlasNoch keine Bewertungen
- Hand Out Fire SurpressDokument69 SeitenHand Out Fire SurpressSeptiawanWandaNoch keine Bewertungen
- Math 9 Quiz 4Dokument3 SeitenMath 9 Quiz 4Lin SisombounNoch keine Bewertungen
- Low Budget Music Promotion and PublicityDokument41 SeitenLow Budget Music Promotion and PublicityFola Folayan100% (3)
- Forex Day Trading SystemDokument17 SeitenForex Day Trading SystemSocial Malik100% (1)
- Pulmonary EmbolismDokument48 SeitenPulmonary Embolismganga2424100% (3)
- Codan Rubber Modern Cars Need Modern Hoses WebDokument2 SeitenCodan Rubber Modern Cars Need Modern Hoses WebYadiNoch keine Bewertungen
- Smart Gas Leakage Detection With Monitoring and Automatic Safety SystemDokument4 SeitenSmart Gas Leakage Detection With Monitoring and Automatic Safety SystemYeasin Arafat FahadNoch keine Bewertungen
- Product Manual 26086 (Revision E) : EGCP-2 Engine Generator Control PackageDokument152 SeitenProduct Manual 26086 (Revision E) : EGCP-2 Engine Generator Control PackageErick KurodaNoch keine Bewertungen
- Importance of Communications 05sept2023Dokument14 SeitenImportance of Communications 05sept2023Sajib BhattacharyaNoch keine Bewertungen
- Experiment - 1: Batch (Differential) Distillation: 1. ObjectiveDokument30 SeitenExperiment - 1: Batch (Differential) Distillation: 1. ObjectiveNaren ParasharNoch keine Bewertungen
- HRMDokument118 SeitenHRMKarthic KasiliaNoch keine Bewertungen
- Focus Edition From GC: Phosphate Bonded Investments For C&B TechniquesDokument35 SeitenFocus Edition From GC: Phosphate Bonded Investments For C&B TechniquesAlexis De Jesus FernandezNoch keine Bewertungen
- Genomic Tools For Crop ImprovementDokument41 SeitenGenomic Tools For Crop ImprovementNeeru RedhuNoch keine Bewertungen
- FpsecrashlogDokument19 SeitenFpsecrashlogtim lokNoch keine Bewertungen
- HepaDokument1 SeiteHepasenthilarasu5100% (1)
- Phylogeny Practice ProblemsDokument3 SeitenPhylogeny Practice ProblemsSusan Johnson100% (1)
- 1.water, Acids, Bases, Buffer Solutions in BiochemistryDokument53 Seiten1.water, Acids, Bases, Buffer Solutions in BiochemistryÇağlaNoch keine Bewertungen
- Eurocode 3: Design of Steel Structures "ReadyDokument26 SeitenEurocode 3: Design of Steel Structures "Readywazydotnet80% (10)
- Chinese Paper Cutting Work SheetDokument4 SeitenChinese Paper Cutting Work Sheet黃梓Noch keine Bewertungen
- Chapter 2Dokument8 SeitenChapter 2Fahmia MidtimbangNoch keine Bewertungen
- Instructions For Preparing Manuscript For Ulunnuha (2019 Template Version) Title (English and Arabic Version)Dokument4 SeitenInstructions For Preparing Manuscript For Ulunnuha (2019 Template Version) Title (English and Arabic Version)Lailatur RahmiNoch keine Bewertungen
- Pipe Cleaner Lesson PlanDokument2 SeitenPipe Cleaner Lesson PlanTaylor FranklinNoch keine Bewertungen
- Virtual Assets Act, 2022Dokument18 SeitenVirtual Assets Act, 2022Rapulu UdohNoch keine Bewertungen
- Acc116 Dec 2022 - Q - Test 1Dokument6 SeitenAcc116 Dec 2022 - Q - Test 12022825274100% (1)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Von EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Bewertung: 3 von 5 Sternen3/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedBewertung: 4.5 von 5 Sternen4.5/5 (82)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDVon EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDBewertung: 5 von 5 Sternen5/5 (3)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionVon EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionBewertung: 4 von 5 Sternen4/5 (404)
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (32)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeVon EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeBewertung: 2 von 5 Sternen2/5 (1)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesVon EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesBewertung: 4.5 von 5 Sternen4.5/5 (1412)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsVon EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNoch keine Bewertungen
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsVon EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsBewertung: 4 von 5 Sternen4/5 (4)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsVon EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsBewertung: 5 von 5 Sternen5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisVon EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisBewertung: 4.5 von 5 Sternen4.5/5 (42)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaVon EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Comfort of Crows: A Backyard YearVon EverandThe Comfort of Crows: A Backyard YearBewertung: 4.5 von 5 Sternen4.5/5 (23)
- The Obesity Code: Unlocking the Secrets of Weight LossVon EverandThe Obesity Code: Unlocking the Secrets of Weight LossBewertung: 4 von 5 Sternen4/5 (6)
- Why We Die: The New Science of Aging and the Quest for ImmortalityVon EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityBewertung: 4.5 von 5 Sternen4.5/5 (6)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisVon EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisBewertung: 3.5 von 5 Sternen3.5/5 (2)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeVon EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeBewertung: 4.5 von 5 Sternen4.5/5 (254)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Von EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Bewertung: 4.5 von 5 Sternen4.5/5 (110)
- To Explain the World: The Discovery of Modern ScienceVon EverandTo Explain the World: The Discovery of Modern ScienceBewertung: 3.5 von 5 Sternen3.5/5 (51)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsVon EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsBewertung: 4.5 von 5 Sternen4.5/5 (39)
- The Marshmallow Test: Mastering Self-ControlVon EverandThe Marshmallow Test: Mastering Self-ControlBewertung: 4.5 von 5 Sternen4.5/5 (60)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingVon EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingBewertung: 4 von 5 Sternen4/5 (1138)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessVon EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessBewertung: 4.5 von 5 Sternen4.5/5 (328)