Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (120)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Adult Carer Quality of Life Questionnaire (AC-QoL)Dokument14 SeitenAdult Carer Quality of Life Questionnaire (AC-QoL)Andi SusiloNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- What, Why and How To Evaluate CurriculumDokument19 SeitenWhat, Why and How To Evaluate Curriculum555555555-589576100% (2)
- Assessmentof Fluency Disorders Chapter 13Dokument53 SeitenAssessmentof Fluency Disorders Chapter 13Sadaf RizwanhumayoonNoch keine Bewertungen
- Baron-Cohen Theories of The Autistic Mind 2008Dokument5 SeitenBaron-Cohen Theories of The Autistic Mind 2008Fris Guinnea SwasonoNoch keine Bewertungen
- Test Bank For Leadership Theory Application and Skill Development 6th Edition LussierDokument53 SeitenTest Bank For Leadership Theory Application and Skill Development 6th Edition Lussiera204491073Noch keine Bewertungen
- MBA Assignment ExampleDokument21 SeitenMBA Assignment ExampleZamo Mkhwanazi75% (4)
- The Artist Is PresentDokument10 SeitenThe Artist Is Presentsancho108Noch keine Bewertungen
- Business Vocabulary in Use AdvancedDokument6 SeitenBusiness Vocabulary in Use AdvancedMadina Abdresheva100% (1)
- Seven Healthy Habits PlansDokument4 SeitenSeven Healthy Habits Plansjessica_dilsaverNoch keine Bewertungen
- Training Design - PRIMALS 4-6 (Math)Dokument3 SeitenTraining Design - PRIMALS 4-6 (Math)oliver100% (2)
- Perdevshs q1 Mod2 Understandingtheconnectionsbetweenthoughtsfeelingsandbehavior v1Dokument29 SeitenPerdevshs q1 Mod2 Understandingtheconnectionsbetweenthoughtsfeelingsandbehavior v1Michael GarciaNoch keine Bewertungen
- Teaching Methodologies in TESOL: PPP vs. TBLDokument11 SeitenTeaching Methodologies in TESOL: PPP vs. TBLMarta100% (10)
- CPE3201 Workplace Counselling PDFDokument15 SeitenCPE3201 Workplace Counselling PDFArif BudimanNoch keine Bewertungen
- Performance Comitment FormDokument5 SeitenPerformance Comitment Formjenny manatadNoch keine Bewertungen
- Principles: of Marketing Global EditionDokument47 SeitenPrinciples: of Marketing Global EditionNgoc PhamNoch keine Bewertungen
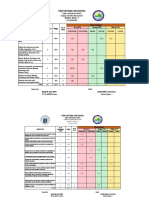
- Mapeh 9 Tos 1ST QuarterDokument5 SeitenMapeh 9 Tos 1ST QuarterKrizha Kate MontausNoch keine Bewertungen
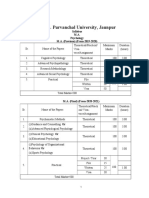
- M.A. I II Psychology SyllabusDokument14 SeitenM.A. I II Psychology SyllabusArunodaya Tripathi ArunNoch keine Bewertungen
- Conversational DiscourseDokument71 SeitenConversational DiscourseesameeeNoch keine Bewertungen
- Exercise Addiction A Literature ReviewDokument7 SeitenExercise Addiction A Literature Reviewc5sq1b48100% (1)
- Trends, Networks, and Critical Thinking Skills in 20 CenturyDokument8 SeitenTrends, Networks, and Critical Thinking Skills in 20 CenturyRaymond ZafraNoch keine Bewertungen
- Personal Statement-Final Draft PortfolioDokument3 SeitenPersonal Statement-Final Draft Portfolioapi-592388368Noch keine Bewertungen
- Strategic Decision MakingDokument16 SeitenStrategic Decision MakingAnkit SinglaNoch keine Bewertungen
- 3.1.5.I Think Theref I Sing Flint - 01 PDFDokument9 Seiten3.1.5.I Think Theref I Sing Flint - 01 PDFAline LeGrand100% (1)
- Values S3Dokument5 SeitenValues S3Alice KrodeNoch keine Bewertungen
- Civic Lesson Y2 RespectDokument1 SeiteCivic Lesson Y2 RespectLogiswari KrishnanNoch keine Bewertungen
- Lesson-Exemplar English9 Melc-1Dokument5 SeitenLesson-Exemplar English9 Melc-1Pethy DecendarioNoch keine Bewertungen
- Writing Sample 1Dokument17 SeitenWriting Sample 1api-540614663Noch keine Bewertungen
- Circle Time Activity Evaluation FormDokument2 SeitenCircle Time Activity Evaluation Formapi-224888954Noch keine Bewertungen
- FS 7 PortfolioDokument8 SeitenFS 7 PortfolioAlyzza Kara Acabal100% (1)
- EFA 219 Module 5 - Sociological Foundations of EducationDokument5 SeitenEFA 219 Module 5 - Sociological Foundations of EducationGATTE EMILENoch keine Bewertungen