Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Planet Maths 5th - Sample PagesDokument30 SeitenPlanet Maths 5th - Sample PagesEdTech Folens48% (29)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Full Moon RitualsDokument22 SeitenFull Moon RitualsJP83% (6)
- Internship Report On Effects of Promotion System On Employee Job Satisfaction of Janata Bank Ltd.Dokument57 SeitenInternship Report On Effects of Promotion System On Employee Job Satisfaction of Janata Bank Ltd.Tareq Alam100% (1)
- Biutiful by The-Lake-2019-FoodDokument1 SeiteBiutiful by The-Lake-2019-Foodstud.10xNoch keine Bewertungen
- UNITATEA - 2 EnglezDokument4 SeitenUNITATEA - 2 Englezstud.10xNoch keine Bewertungen
- Planning For CoronavirusDokument4 SeitenPlanning For Coronavirusstud.10xNoch keine Bewertungen
- A Coordinated Global Research Roadmap:: 2019 Novel CoronavirusDokument36 SeitenA Coordinated Global Research Roadmap:: 2019 Novel CoronavirusManuel OropezaNoch keine Bewertungen
- Power and Leadership: Unitatea 3Dokument4 SeitenPower and Leadership: Unitatea 3stud.10xNoch keine Bewertungen
- En Pricelist Online HIGHTECH BerarieDokument3 SeitenEn Pricelist Online HIGHTECH Berariestud.10xNoch keine Bewertungen
- UNITATEA - 4 EnglezaDokument3 SeitenUNITATEA - 4 Englezastud.10xNoch keine Bewertungen
- UNITATEA - 5 EnglezaDokument3 SeitenUNITATEA - 5 Englezastud.10xNoch keine Bewertungen
- Tiling FloorsDokument4 SeitenTiling FloorsApollyonNoch keine Bewertungen
- Biological Pollutants in Your Home PDFDokument4 SeitenBiological Pollutants in Your Home PDFCarolea SabinaNoch keine Bewertungen
- Unitatea 6: Does Altruism Exist ? (Part 2)Dokument6 SeitenUnitatea 6: Does Altruism Exist ? (Part 2)stud.10xNoch keine Bewertungen
- Different Types of Hammers PDFDokument3 SeitenDifferent Types of Hammers PDFKyrios PantelisNoch keine Bewertungen
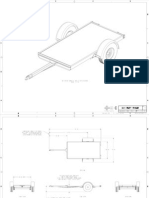
- 4x8 Utility Trailer-DrawingsDokument18 Seiten4x8 Utility Trailer-Drawingscualete100% (1)
- Wilderness Survival Techniques and TipsDokument4 SeitenWilderness Survival Techniques and TipsBudulan RaduNoch keine Bewertungen
- 11 Steps To Survival - Canada Emergency Measurses OrganizationDokument25 Seiten11 Steps To Survival - Canada Emergency Measurses OrganizationChristopher WilfordNoch keine Bewertungen
- 870 Emergency Food Preparation Militia Cookbook PDFDokument37 Seiten870 Emergency Food Preparation Militia Cookbook PDFodhiseoNoch keine Bewertungen
- Enjoy Yeast Breads - FN283Dokument37 SeitenEnjoy Yeast Breads - FN283ravenseye100% (1)
- 11 Steps To Survival - Canada Emergency Measurses OrganizationDokument25 Seiten11 Steps To Survival - Canada Emergency Measurses OrganizationChristopher WilfordNoch keine Bewertungen
- Criterii de Elaborare LicentaDokument2 SeitenCriterii de Elaborare Licentastud.10xNoch keine Bewertungen
- Mathematics - Grade 9 - First QuarterDokument9 SeitenMathematics - Grade 9 - First QuarterSanty Enril Belardo Jr.Noch keine Bewertungen
- Number SystemsDokument165 SeitenNumber SystemsapamanNoch keine Bewertungen
- Brain Imaging TechniquesDokument6 SeitenBrain Imaging TechniquesIlika Guha MajumdarNoch keine Bewertungen
- Mathematicaleconomics PDFDokument84 SeitenMathematicaleconomics PDFSayyid JifriNoch keine Bewertungen
- PsychFirstAidSchools PDFDokument186 SeitenPsychFirstAidSchools PDFAna ChicasNoch keine Bewertungen
- Interfaces and Inheritance in JavaDokument1 SeiteInterfaces and Inheritance in JavaegdejuanaNoch keine Bewertungen
- Radiography Safety ProcedureDokument9 SeitenRadiography Safety ProcedureأحمدآلزهوNoch keine Bewertungen
- Ernesto Sirolli - Eenterprise FacilitationDokument300 SeitenErnesto Sirolli - Eenterprise FacilitationFrancis James Leite Marques PereiraNoch keine Bewertungen
- Roman Villas at Tor Marancia and CentocelleDokument10 SeitenRoman Villas at Tor Marancia and CentocelleIgor ĆirkovićNoch keine Bewertungen
- Argumentative Essay Project DescriptionDokument5 SeitenArgumentative Essay Project DescriptionKaren Jh MoncayoNoch keine Bewertungen
- Tugas, MO - REVIEW JURNAL JIT - Ikomang Aditya Prawira Nugraha (1902612010304)Dokument12 SeitenTugas, MO - REVIEW JURNAL JIT - Ikomang Aditya Prawira Nugraha (1902612010304)MamanxNoch keine Bewertungen
- Sri Guru Parampara Stotram CompressDokument14 SeitenSri Guru Parampara Stotram CompressSatishPavurayalaNoch keine Bewertungen
- (Paper-2) 20th Century Indian Writing: Saadat Hasan Manto: Toba Tek SinghDokument18 Seiten(Paper-2) 20th Century Indian Writing: Saadat Hasan Manto: Toba Tek SinghApexa Kerai67% (3)
- MISKDokument134 SeitenMISKmusyokaNoch keine Bewertungen
- DLL Week 5Dokument3 SeitenDLL Week 5Nen CampNoch keine Bewertungen
- Biblehub Com Commentaries Matthew 3 17 HTMDokument21 SeitenBiblehub Com Commentaries Matthew 3 17 HTMSorin TrimbitasNoch keine Bewertungen
- 9.2 Volumetric Analysis PDFDokument24 Seiten9.2 Volumetric Analysis PDFJoaquinNoch keine Bewertungen
- Professional Education Pre-Licensure Examination For TeachersDokument12 SeitenProfessional Education Pre-Licensure Examination For TeachersJudy Mae ManaloNoch keine Bewertungen
- Reaction PaperDokument3 SeitenReaction PaperCecille Robles San JoseNoch keine Bewertungen
- Darkness Points Reminder 2Dokument2 SeitenDarkness Points Reminder 2Tata YoyoNoch keine Bewertungen
- Unsung Ancient African Indigenous Heroines and HerosDokument27 SeitenUnsung Ancient African Indigenous Heroines and Herosmsipaa30Noch keine Bewertungen
- Symbiosis National Aptitude Test (SNAP) 2004: InstructionsDokument21 SeitenSymbiosis National Aptitude Test (SNAP) 2004: InstructionsHarsh JainNoch keine Bewertungen
- Acidity (As Acetic Acid) On Undenatured and Denatured EthanolDokument10 SeitenAcidity (As Acetic Acid) On Undenatured and Denatured EthanolVinh NguyenNoch keine Bewertungen
- Character Formation 1: Nationalism and PatriotismDokument11 SeitenCharacter Formation 1: Nationalism and Patriotismban diaz100% (1)
- Boden 2015 Mass Media Playground of StereotypingDokument16 SeitenBoden 2015 Mass Media Playground of StereotypingMiguel CuevaNoch keine Bewertungen
- Resume of Masterchef Contestant, Melissa GutierrezDokument3 SeitenResume of Masterchef Contestant, Melissa GutierrezMikhail GalatinovNoch keine Bewertungen
- Customer Refund: Responsibility: Yodlee US AR Super User Navigation: Transactions TransactionsDokument12 SeitenCustomer Refund: Responsibility: Yodlee US AR Super User Navigation: Transactions TransactionsAziz KhanNoch keine Bewertungen