Das könnte Ihnen auch gefallen
- Handbook of Inpatient EndocrinologyVon EverandHandbook of Inpatient EndocrinologyRajesh K. GargNoch keine Bewertungen
- Growth After Adenotonsillectomy For Obstructive Sleep Apnea: An RCTDokument10 SeitenGrowth After Adenotonsillectomy For Obstructive Sleep Apnea: An RCTCalvin AffendyNoch keine Bewertungen
- Growth After AdenotonsillectomyDokument10 SeitenGrowth After AdenotonsillectomyfriscahalimNoch keine Bewertungen
- Effects of A Neurodevelopmental Treatment Based.3Dokument13 SeitenEffects of A Neurodevelopmental Treatment Based.3ivairmatiasNoch keine Bewertungen
- Gomez Conesa2016Dokument1 SeiteGomez Conesa2016Maura Pilquiman MaldonadoNoch keine Bewertungen
- Prader WilliDokument16 SeitenPrader WilliGabriela DrăgoiNoch keine Bewertungen
- Daily Prednisone Treatment in Duchenne Muscular Dystrophy in Southwest ChinaDokument7 SeitenDaily Prednisone Treatment in Duchenne Muscular Dystrophy in Southwest ChinaEduardoNoch keine Bewertungen
- E236 FullDokument9 SeitenE236 FullBelinda SuhuyanlyNoch keine Bewertungen
- Deformidad Craneal y Desarrollo MotorDokument9 SeitenDeformidad Craneal y Desarrollo MotordianareinaNoch keine Bewertungen
- Idiopathic Short Stature Definition EpidDokument9 SeitenIdiopathic Short Stature Definition Epidfrancisco perezNoch keine Bewertungen
- 26 Audh Ampun Aduh AmpunDokument3 Seiten26 Audh Ampun Aduh Ampundel AjjahNoch keine Bewertungen
- Childhood Obesity-Knowledge, Attitudes, and Practices of European Pediatric Care Providers (Pediatrics2013)Dokument11 SeitenChildhood Obesity-Knowledge, Attitudes, and Practices of European Pediatric Care Providers (Pediatrics2013)jose matosNoch keine Bewertungen
- Down 3 - 5 MesesDokument8 SeitenDown 3 - 5 MesesJeancarlosTerapiaFisicaNoch keine Bewertungen
- Lowe 2015Dokument9 SeitenLowe 2015ﻱﺪﺢ ﺁﻏﻦﻎNoch keine Bewertungen
- Adolescents DMT1Dokument8 SeitenAdolescents DMT1Mia ValdesNoch keine Bewertungen
- Osteopathic Treatment of Infants in Their First Year of Life: A Prospective Multicenter Observational Study (OSTINF Study)Dokument12 SeitenOsteopathic Treatment of Infants in Their First Year of Life: A Prospective Multicenter Observational Study (OSTINF Study)ElisangelaNoch keine Bewertungen
- 2022 General Movements e Desenvolvimento Aos 2 AnosDokument13 Seiten2022 General Movements e Desenvolvimento Aos 2 AnosCibelle FormigaNoch keine Bewertungen
- Exercise Effects For Children With Autism Spectrum Disorder: Metabolic Health, Autistic Traits, and Quality of LifeDokument21 SeitenExercise Effects For Children With Autism Spectrum Disorder: Metabolic Health, Autistic Traits, and Quality of LifeNatalia Fernanda Trigo EspinozaNoch keine Bewertungen
- ADHD, Stimulant Treatment, and GrowthDokument10 SeitenADHD, Stimulant Treatment, and GrowthSyaika Amelia ZahraNoch keine Bewertungen
- Growth in Cerebral Palsy Children Between 3-13 Years in Urban Dharwad, IndiaDokument7 SeitenGrowth in Cerebral Palsy Children Between 3-13 Years in Urban Dharwad, IndiaDr. Krishna N. Sharma100% (1)
- J. Pediatr. Psychol. 2003 Dieter 403 11Dokument10 SeitenJ. Pediatr. Psychol. 2003 Dieter 403 11knikmahNoch keine Bewertungen
- NIH Public Access: A Two Year Randomized Controlled Trial of Progressive Resistance Exercise For Parkinson's DiseaseDokument18 SeitenNIH Public Access: A Two Year Randomized Controlled Trial of Progressive Resistance Exercise For Parkinson's DiseaseAnisa SafutriNoch keine Bewertungen
- Nejm ArticleDokument10 SeitenNejm Articlemadimadi11Noch keine Bewertungen
- Art Borrador 2Dokument10 SeitenArt Borrador 2Laura jasbleidy Gutiérrez agudeloNoch keine Bewertungen
- Etiologies and Early Diagnosis of Short Stature and Growth Failure in Children and AdolescentsDokument20 SeitenEtiologies and Early Diagnosis of Short Stature and Growth Failure in Children and AdolescentsAnonymous 4N1GrDNoch keine Bewertungen
- Malone Final SignedDokument29 SeitenMalone Final Signedapi-622666324Noch keine Bewertungen
- Parental Obesity and Early Childhood Development: BackgroundDokument12 SeitenParental Obesity and Early Childhood Development: BackgroundJejem Marandra EmkamasNoch keine Bewertungen
- Health-Related Quality of Life and Intellectual Functioning in Children in Remission From Acute Lymphoblastic LeukaemiaDokument7 SeitenHealth-Related Quality of Life and Intellectual Functioning in Children in Remission From Acute Lymphoblastic LeukaemiaancoursNoch keine Bewertungen
- 2016 Article 23Dokument8 Seiten2016 Article 23Vandy IkraNoch keine Bewertungen
- Ijrm 11 583 PDFDokument6 SeitenIjrm 11 583 PDFAnsoriNoch keine Bewertungen
- Longitudinal Study of Growth of Children With Unilateral Cleft-Lip Palate From Birth To Two Years of AgeDokument7 SeitenLongitudinal Study of Growth of Children With Unilateral Cleft-Lip Palate From Birth To Two Years of AgeCarlos CastañedaNoch keine Bewertungen
- Peds 2012-1835Dokument8 SeitenPeds 2012-1835Naraianne FerreiraNoch keine Bewertungen
- Laporan PendahuluanDokument11 SeitenLaporan Pendahuluanayu noviaindriyani19Noch keine Bewertungen
- Dyw 236Dokument12 SeitenDyw 236Fatamorgana AbdullahNoch keine Bewertungen
- Symptom Profiles of Autism Spectrum Disorder in Tuberous Sclerosis ComplexDokument14 SeitenSymptom Profiles of Autism Spectrum Disorder in Tuberous Sclerosis ComplexWhyra Namikaze ComeyNoch keine Bewertungen
- Melatonina (2017) Gringras P. Niños 3-5mgDokument31 SeitenMelatonina (2017) Gringras P. Niños 3-5mgAlumno del Doctorado FarmacologiaNoch keine Bewertungen
- Growth and Health in Children With Moderate-to-Severe Cerebral PalsyDokument11 SeitenGrowth and Health in Children With Moderate-to-Severe Cerebral PalsyNudyan BetharinaNoch keine Bewertungen
- Down SyndromeDokument12 SeitenDown SyndromeaidaeimanNoch keine Bewertungen
- To Study Correlation of Insulin Resistance With Physical Activity in Children / AdolescentsDokument4 SeitenTo Study Correlation of Insulin Resistance With Physical Activity in Children / AdolescentsIJAR JOURNALNoch keine Bewertungen
- Paediatrica Indonesiana: Original ArticleDokument5 SeitenPaediatrica Indonesiana: Original ArticleNisak HumairokNoch keine Bewertungen
- Research Paper On Duchenne Muscular DystrophyDokument4 SeitenResearch Paper On Duchenne Muscular Dystrophycantfp00100% (1)
- Leschek 2004Dokument9 SeitenLeschek 2004GutoGonçalvesNoch keine Bewertungen
- Wang 2015Dokument8 SeitenWang 2015mammon mammonovNoch keine Bewertungen
- Specific Treatment of Prader Willi Syndrome Through Cyclical Rehabilitation ProgrammesDokument12 SeitenSpecific Treatment of Prader Willi Syndrome Through Cyclical Rehabilitation Programmesvcnflga08Noch keine Bewertungen
- Health Outcomes Associated With Micronutrient-Fortified Complementary Foods in Infants and Young Children Aged 6-23 Months - A Systematic Review and Meta-AnalysisDokument12 SeitenHealth Outcomes Associated With Micronutrient-Fortified Complementary Foods in Infants and Young Children Aged 6-23 Months - A Systematic Review and Meta-AnalysisIra DwijayantiNoch keine Bewertungen
- MR KRISTIAN DAMGAARD LYNG (Orcid ID: 0000-0001-8668-691X) DR SINEAD HOLDEN (Orcid ID: 0000-0002-7314-2152)Dokument18 SeitenMR KRISTIAN DAMGAARD LYNG (Orcid ID: 0000-0001-8668-691X) DR SINEAD HOLDEN (Orcid ID: 0000-0002-7314-2152)Afifah Nur FauzaniNoch keine Bewertungen
- 10.7556 Jaoa.1992.92.6.729Dokument16 Seiten10.7556 Jaoa.1992.92.6.729consueloamado.medNoch keine Bewertungen
- Assessment of Nutritional Status Based On Strongkids Tool in Iranian Hospitalized ChildrenDokument7 SeitenAssessment of Nutritional Status Based On Strongkids Tool in Iranian Hospitalized Childrenfarah febriyantiNoch keine Bewertungen
- E782 FullDokument10 SeitenE782 FullDân NguyễnNoch keine Bewertungen
- Peyang 2Dokument22 SeitenPeyang 2RizqaFebrilianyNoch keine Bewertungen
- Medical Comorbidities in Children and AdolescentsDokument12 SeitenMedical Comorbidities in Children and AdolescentsSalud-psicología-psiquiatria DocenciaNoch keine Bewertungen
- Relationship of Body Fat and Cardiorespiratory Fitness With Cardiovascular Risk in Chinese ChildrenDokument5 SeitenRelationship of Body Fat and Cardiorespiratory Fitness With Cardiovascular Risk in Chinese ChildrenArya KusumaNoch keine Bewertungen
- Asociacioìn Entre SOP y TDAHDokument10 SeitenAsociacioìn Entre SOP y TDAHalondraNoch keine Bewertungen
- Effect of Physiotherapy On Spinal AlignmentDokument8 SeitenEffect of Physiotherapy On Spinal Alignmentnistormaria492Noch keine Bewertungen
- E113 FullDokument8 SeitenE113 FullMirza RisqaNoch keine Bewertungen
- Ploegstra2016, Crescimento X Hipertensão Pulmonar em PediatriaDokument10 SeitenPloegstra2016, Crescimento X Hipertensão Pulmonar em PediatrialaerciomoreiradearaujomoreiraNoch keine Bewertungen
- Content ServerDokument9 SeitenContent ServerKennie RamirezNoch keine Bewertungen
- Published PaperDokument6 SeitenPublished PaperjamesNoch keine Bewertungen
- NIH Public Access: Author ManuscriptDokument17 SeitenNIH Public Access: Author ManuscriptSabrina OliveiraNoch keine Bewertungen
- Biomedical Interventions For Teens and Young Adults: The Value of PersistenceDokument36 SeitenBiomedical Interventions For Teens and Young Adults: The Value of PersistenceautismoneNoch keine Bewertungen
- E357 FullDokument12 SeitenE357 FullCalvin AffendyNoch keine Bewertungen
- 444 FullDokument10 Seiten444 FullCalvin AffendyNoch keine Bewertungen
- Worobec2009 PDFDokument20 SeitenWorobec2009 PDFCalvin AffendyNoch keine Bewertungen
- Three-Year Longitudinal Survey Comparing Visual Satisfaction With LASIK and Contact LensesDokument8 SeitenThree-Year Longitudinal Survey Comparing Visual Satisfaction With LASIK and Contact LensesCalvin AffendyNoch keine Bewertungen
- E20153547 Full PDFDokument12 SeitenE20153547 Full PDFCalvin AffendyNoch keine Bewertungen
- Fracture Risk and Zoledronic Acid Therapy in Men With OsteoporosisDokument10 SeitenFracture Risk and Zoledronic Acid Therapy in Men With OsteoporosisCalvin AffendyNoch keine Bewertungen
- S177 Full PDFDokument4 SeitenS177 Full PDFCalvin AffendyNoch keine Bewertungen
- P013156567 PDFDokument3 SeitenP013156567 PDFCalvin AffendyNoch keine Bewertungen
- E868 FullDokument10 SeitenE868 FullCalvin AffendyNoch keine Bewertungen
- Intravenous Zoledronic Acid in Postmenopausal Women With Low Bone Mineral DensityDokument9 SeitenIntravenous Zoledronic Acid in Postmenopausal Women With Low Bone Mineral DensityCalvin AffendyNoch keine Bewertungen
- Journal Medicine: The New EnglandDokument8 SeitenJournal Medicine: The New EnglandCalvin AffendyNoch keine Bewertungen
- E1533 Full PDFDokument10 SeitenE1533 Full PDFCalvin AffendyNoch keine Bewertungen
- Penggunaan Sedasi Pada Anak Dengan VentilatorDokument5 SeitenPenggunaan Sedasi Pada Anak Dengan VentilatorCalvin AffendyNoch keine Bewertungen
- Iron Supplementation in Pregnancy or Infancy and Motor Development: A Randomized Controlled TrialDokument12 SeitenIron Supplementation in Pregnancy or Infancy and Motor Development: A Randomized Controlled TrialCalvin AffendyNoch keine Bewertungen
- S177 FullDokument4 SeitenS177 FullCalvin AffendyNoch keine Bewertungen
- E607 FullDokument10 SeitenE607 FullCalvin AffendyNoch keine Bewertungen
- Bowel Preparations For Colonoscopy: An RCT: AuthorsDokument10 SeitenBowel Preparations For Colonoscopy: An RCT: AuthorsCalvin AffendyNoch keine Bewertungen
- Jurnal LepraDokument20 SeitenJurnal LepraCalvin AffendyNoch keine Bewertungen
- PLX7100A Digital Mobile C-Arm X-Ray Machine: 1. Technical SpecificationDokument3 SeitenPLX7100A Digital Mobile C-Arm X-Ray Machine: 1. Technical SpecificationAbdalhakeem AlturkyNoch keine Bewertungen
- IncarnationDokument3 SeitenIncarnationViviana PueblaNoch keine Bewertungen
- An FPGA Implementation of A Feed-Back Chaotic Synchronization For Secure CommunicationsDokument5 SeitenAn FPGA Implementation of A Feed-Back Chaotic Synchronization For Secure Communicationslaz_chikhi1574Noch keine Bewertungen
- ImmunologyDokument8 SeitenImmunologyማላያላም ማላያላም89% (9)
- Application Note Usrp and HDSDR Spectrum MonitoringDokument14 SeitenApplication Note Usrp and HDSDR Spectrum MonitoringcaraboyNoch keine Bewertungen
- NumaticsFRLFlexiblokR072010 EsDokument40 SeitenNumaticsFRLFlexiblokR072010 EsGabriel San Martin RifoNoch keine Bewertungen
- Lec1 PDFDokument12 SeitenLec1 PDFtogarsNoch keine Bewertungen
- Physics Sample Question PaperDokument9 SeitenPhysics Sample Question PaperVarsha SharmaNoch keine Bewertungen
- Change LogDokument3 SeitenChange Logyoga hendriyantoNoch keine Bewertungen
- Product Bulletin N 6: Bearing Assemblies - Shaft VariationsDokument1 SeiteProduct Bulletin N 6: Bearing Assemblies - Shaft VariationsRANAIVOARIMANANANoch keine Bewertungen
- Construction Materials and TestingDokument23 SeitenConstruction Materials and TestingJaymark S. GicaleNoch keine Bewertungen
- XG5000 Manual (2009.10.26) (Eng)Dokument645 SeitenXG5000 Manual (2009.10.26) (Eng)wanderly_40100% (1)
- Dbms-Lab Assignment - 1: Name - VIKAS SINGH Roll No - 4257Dokument3 SeitenDbms-Lab Assignment - 1: Name - VIKAS SINGH Roll No - 4257Vikas SinghNoch keine Bewertungen
- Number Patterns and SequencesDokument10 SeitenNumber Patterns and SequencesMohamed Hawash80% (5)
- Momus Design CNC Router Manual Version 2.1Dokument178 SeitenMomus Design CNC Router Manual Version 2.1Francisco Teruel100% (8)
- 19 04 20 p2 PDFDokument32 Seiten19 04 20 p2 PDFGovind SajuNoch keine Bewertungen
- Introduction To DatabasesDokument33 SeitenIntroduction To Databases米皮皮Noch keine Bewertungen
- App NandDokument30 SeitenApp NandRajesh MedampudiNoch keine Bewertungen
- Excel Formulas and Functions 2021-The Intermediate Level Step byDokument122 SeitenExcel Formulas and Functions 2021-The Intermediate Level Step bymaolegu100% (3)
- V1 N2 1980 RabenhorstDokument6 SeitenV1 N2 1980 Rabenhorstraa2010Noch keine Bewertungen
- 4$20 Triangles$20 ProofsDokument23 Seiten4$20 Triangles$20 ProofsBaskaran SeetharamanNoch keine Bewertungen
- Beam Design: BackgroundDokument2 SeitenBeam Design: BackgroundolomizanaNoch keine Bewertungen
- RWC 123 Manoj Prabhakar KaiwartDokument13 SeitenRWC 123 Manoj Prabhakar KaiwartManoj Prabhakar KaiwartNoch keine Bewertungen
- Differential Pr. Gauges Bellow Type 1Dokument2 SeitenDifferential Pr. Gauges Bellow Type 1Vara PrasadNoch keine Bewertungen
- Case Study Class 12 Physics ImportantDokument5 SeitenCase Study Class 12 Physics Importantdivanshu2006yadavNoch keine Bewertungen
- Soiling Rates of PV Modules vs. Thermopile PyranometersDokument3 SeitenSoiling Rates of PV Modules vs. Thermopile PyranometersAbdul Mohid SheikhNoch keine Bewertungen
- Optical Properties of Gem Substances Educational Objective: This Exercise, Unit 7 in The Above Syllabus, Will Introduce Students To Skills andDokument19 SeitenOptical Properties of Gem Substances Educational Objective: This Exercise, Unit 7 in The Above Syllabus, Will Introduce Students To Skills andCarl SoriaNoch keine Bewertungen
- Epson L6170 Wi-Fi Duplex All-in-One Ink Tank Printer With ADFDokument3 SeitenEpson L6170 Wi-Fi Duplex All-in-One Ink Tank Printer With ADFCarl DonaireNoch keine Bewertungen
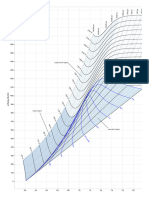
- Mollier Enthalpy Entropy Chart For Steam - US UnitsDokument1 SeiteMollier Enthalpy Entropy Chart For Steam - US Unitslin tongNoch keine Bewertungen
- ORC - Airbag SystemDokument13 SeitenORC - Airbag SystemGarikoitz FranciscoeneNoch keine Bewertungen
- Peak: The New Science of Athletic Performance That is Revolutionizing SportsVon EverandPeak: The New Science of Athletic Performance That is Revolutionizing SportsBewertung: 5 von 5 Sternen5/5 (97)
- Relentless: From Good to Great to UnstoppableVon EverandRelentless: From Good to Great to UnstoppableBewertung: 5 von 5 Sternen5/5 (788)
- Chair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouVon EverandChair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouBewertung: 3.5 von 5 Sternen3.5/5 (5)
- Functional Training and Beyond: Building the Ultimate Superfunctional Body and MindVon EverandFunctional Training and Beyond: Building the Ultimate Superfunctional Body and MindBewertung: 4.5 von 5 Sternen4.5/5 (1)
- Aging Backwards: Reverse the Aging Process and Look 10 Years Younger in 30 Minutes a DayVon EverandAging Backwards: Reverse the Aging Process and Look 10 Years Younger in 30 Minutes a DayNoch keine Bewertungen
- Boundless: Upgrade Your Brain, Optimize Your Body & Defy AgingVon EverandBoundless: Upgrade Your Brain, Optimize Your Body & Defy AgingBewertung: 4.5 von 5 Sternen4.5/5 (67)
- The Yogi Code: Seven Universal Laws of Infinite SuccessVon EverandThe Yogi Code: Seven Universal Laws of Infinite SuccessBewertung: 4.5 von 5 Sternen4.5/5 (104)
- Muscle for Life: Get Lean, Strong, and Healthy at Any Age!Von EverandMuscle for Life: Get Lean, Strong, and Healthy at Any Age!Bewertung: 4.5 von 5 Sternen4.5/5 (22)
- Yin Yoga: How to Enhance Your Modern Yoga Practice With Yin Yoga to Achieve an Optimal Mind-Body Connection: Yoga Mastery SeriesVon EverandYin Yoga: How to Enhance Your Modern Yoga Practice With Yin Yoga to Achieve an Optimal Mind-Body Connection: Yoga Mastery SeriesNoch keine Bewertungen
- Power of 10: The Once-A-Week Slow Motion Fitness RevolutionVon EverandPower of 10: The Once-A-Week Slow Motion Fitness RevolutionBewertung: 3.5 von 5 Sternen3.5/5 (11)
- Strong Is the New Beautiful: Embrace Your Natural Beauty, Eat Clean, and Harness Your PowerVon EverandStrong Is the New Beautiful: Embrace Your Natural Beauty, Eat Clean, and Harness Your PowerBewertung: 4 von 5 Sternen4/5 (5)
- Not a Diet Book: Take Control. Gain Confidence. Change Your Life.Von EverandNot a Diet Book: Take Control. Gain Confidence. Change Your Life.Bewertung: 3.5 von 5 Sternen3.5/5 (7)
- Wheels of Life: A User's Guide to the Chakra SystemVon EverandWheels of Life: A User's Guide to the Chakra SystemBewertung: 4.5 von 5 Sternen4.5/5 (34)
- Endure: Mind, Body, and the Curiously Elastic Limits of Human PerformanceVon EverandEndure: Mind, Body, and the Curiously Elastic Limits of Human PerformanceBewertung: 4.5 von 5 Sternen4.5/5 (237)
- Pranayama: The Yoga Science of BreathingVon EverandPranayama: The Yoga Science of BreathingBewertung: 4.5 von 5 Sternen4.5/5 (8)
- Strength Training Over 40: The Only Weight Training Workout Book You Will Need to Maintain or Build Your Strength, Muscle Mass, Energy, Overall Fitness and Stay Healthy Without Living in the GymVon EverandStrength Training Over 40: The Only Weight Training Workout Book You Will Need to Maintain or Build Your Strength, Muscle Mass, Energy, Overall Fitness and Stay Healthy Without Living in the GymBewertung: 4 von 5 Sternen4/5 (6)
- Music For Healing: With Nature Sounds For Natural Healing Powers: Sounds Of Nature, Deep Sleep Music, Meditation, Relaxation, Healing MusicVon EverandMusic For Healing: With Nature Sounds For Natural Healing Powers: Sounds Of Nature, Deep Sleep Music, Meditation, Relaxation, Healing MusicBewertung: 5 von 5 Sternen5/5 (1)
- Easy Strength: How to Get a Lot Stronger Than Your Competition-And Dominate in Your SportVon EverandEasy Strength: How to Get a Lot Stronger Than Your Competition-And Dominate in Your SportBewertung: 4.5 von 5 Sternen4.5/5 (17)
- Tibetan Yoga: Magical Movements of Body, Breath, and MindVon EverandTibetan Yoga: Magical Movements of Body, Breath, and MindBewertung: 5 von 5 Sternen5/5 (1)
- Mind Your Body: 4 Weeks to a Leaner, Healthier LifeVon EverandMind Your Body: 4 Weeks to a Leaner, Healthier LifeBewertung: 4.5 von 5 Sternen4.5/5 (5)
- Not a Diet Book: Take Control. Gain Confidence. Change Your Life.Von EverandNot a Diet Book: Take Control. Gain Confidence. Change Your Life.Bewertung: 4.5 von 5 Sternen4.5/5 (124)
- 8 Weeks to 30 Consecutive Pull-Ups: Build Your Upper Body Working Your Upper Back, Shoulders, and Biceps | at Home Workouts | No Gym Required |Von Everand8 Weeks to 30 Consecutive Pull-Ups: Build Your Upper Body Working Your Upper Back, Shoulders, and Biceps | at Home Workouts | No Gym Required |Noch keine Bewertungen
- The Power of Fastercise: Using the New Science of Signaling Exercise to Get Surprisingly Fit in Just a Few Minutes a DayVon EverandThe Power of Fastercise: Using the New Science of Signaling Exercise to Get Surprisingly Fit in Just a Few Minutes a DayBewertung: 4 von 5 Sternen4/5 (4)
- The Total Kettlebell Workout: Trade Secrets of a Personal TrainerVon EverandThe Total Kettlebell Workout: Trade Secrets of a Personal TrainerBewertung: 5 von 5 Sternen5/5 (1)
- Fascial Training: With Easy Exercises To More Mobility And Less Pain (10 Minutes Fascia Workout For Home)Von EverandFascial Training: With Easy Exercises To More Mobility And Less Pain (10 Minutes Fascia Workout For Home)Bewertung: 5 von 5 Sternen5/5 (3)
- True Yoga: Practicing With the Yoga Sutras for Happiness & Spiritual FulfillmentVon EverandTrue Yoga: Practicing With the Yoga Sutras for Happiness & Spiritual FulfillmentBewertung: 4.5 von 5 Sternen4.5/5 (22)
- Roxane Gay & Everand Originals: Built for This: The Quiet Strength of PowerliftingVon EverandRoxane Gay & Everand Originals: Built for This: The Quiet Strength of PowerliftingBewertung: 4.5 von 5 Sternen4.5/5 (133)