Das könnte Ihnen auch gefallen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- A Big Five Scoring System MBTIDokument10 SeitenA Big Five Scoring System MBTIcapuletoNoch keine Bewertungen
- Ogl 482 Discussion 1Dokument5 SeitenOgl 482 Discussion 1api-529016443Noch keine Bewertungen
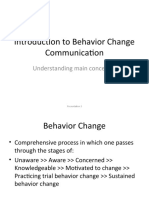
- Introduction To Behavior Change Communication: Understanding Main ConceptsDokument20 SeitenIntroduction To Behavior Change Communication: Understanding Main ConceptsMuhammad Junaid ShaikhNoch keine Bewertungen
- Weekly Home Learning Plan (English) Week 3Dokument6 SeitenWeekly Home Learning Plan (English) Week 3Jo-Ane T. SierasNoch keine Bewertungen
- 2A2 Civic LOVEDokument2 Seiten2A2 Civic LOVENOOR ASILATI BINTI ARIFFIN MoeNoch keine Bewertungen
- Performance Appraisal For Admin OfficerDokument5 SeitenPerformance Appraisal For Admin OfficerKaisar MukadamNoch keine Bewertungen
- Research Philosophy:: The Four ParadigmsDokument34 SeitenResearch Philosophy:: The Four ParadigmsjimmyhaziminNoch keine Bewertungen
- Subpersonality NotesDokument2 SeitenSubpersonality NotesDMNoch keine Bewertungen
- The Cone of Experience - PPT 9 27 1Dokument20 SeitenThe Cone of Experience - PPT 9 27 1Erica Santiago100% (1)
- Social and Emotional LearningDokument15 SeitenSocial and Emotional LearningIJ VillocinoNoch keine Bewertungen
- MAN 6266 - Interview Assignment PDFDokument2 SeitenMAN 6266 - Interview Assignment PDFjoseNoch keine Bewertungen
- Reaction Paper MT Q1 Taghoynsa DilimDokument1 SeiteReaction Paper MT Q1 Taghoynsa DilimJuneth Billones100% (2)
- Amelia Lorensia - Persepsi Apoteker Terhadap Hambatan Dalam Pelayanan Kefarmasian Penyakit Asma - 2020Dokument27 SeitenAmelia Lorensia - Persepsi Apoteker Terhadap Hambatan Dalam Pelayanan Kefarmasian Penyakit Asma - 2020nathasia elgaNoch keine Bewertungen
- Midterm ExamDokument7 SeitenMidterm ExamLovely Mae GalosNoch keine Bewertungen
- Mid-East Honors Association 2021 Conference ProgramDokument38 SeitenMid-East Honors Association 2021 Conference ProgramMid-East Honors AssociationNoch keine Bewertungen
- Naeyc Standard 4Dokument3 SeitenNaeyc Standard 4api-544451361Noch keine Bewertungen
- Plato's Understanding On RealityDokument1 SeitePlato's Understanding On RealityWella Lou JardelozaNoch keine Bewertungen
- MBA Third Semester Model Question Paper - 2009: Management and Organization Development-MU0002 (2 Credits)Dokument11 SeitenMBA Third Semester Model Question Paper - 2009: Management and Organization Development-MU0002 (2 Credits)ManindersuriNoch keine Bewertungen
- Ogl343 Module 3 Notes Part 1 Assignment 3 1 2Dokument2 SeitenOgl343 Module 3 Notes Part 1 Assignment 3 1 2api-538591755Noch keine Bewertungen
- TOK Science Unit PlannerDokument2 SeitenTOK Science Unit PlannerxaglobalNoch keine Bewertungen
- Constructing The Subject. Historical Origins of Psychological Research - Kurt Danziger (1990) PDFDokument261 SeitenConstructing The Subject. Historical Origins of Psychological Research - Kurt Danziger (1990) PDFAdriano Herrera Dá100% (2)
- Lesson Plan 9 Maths - Volume and Capacity ActivitiesDokument4 SeitenLesson Plan 9 Maths - Volume and Capacity Activitiesapi-299034986Noch keine Bewertungen
- Sample Progress ReportDokument1 SeiteSample Progress Reportapi-246567120Noch keine Bewertungen
- Lesson Plan HomophonesDokument11 SeitenLesson Plan Homophonesapi-356065858Noch keine Bewertungen
- Lesson Plan in MathematicsDokument11 SeitenLesson Plan in MathematicsMarianne Bendoy ParohinogNoch keine Bewertungen
- Maka-Diyos-Cluster For Upload - PDF Version 1Dokument16 SeitenMaka-Diyos-Cluster For Upload - PDF Version 1Angel Chane OstrazNoch keine Bewertungen
- A 5 Wilhelm Single Session Strengths & Strategies in Clinical PracticeDokument70 SeitenA 5 Wilhelm Single Session Strengths & Strategies in Clinical PracticeAngie CarrilloNoch keine Bewertungen
- The PPT Slides With Notes Under The Slides Should Be Converted/ Exported To A Word/PDF Document and Submitted Online Via Turnitin!Dokument4 SeitenThe PPT Slides With Notes Under The Slides Should Be Converted/ Exported To A Word/PDF Document and Submitted Online Via Turnitin!vikasNoch keine Bewertungen
- Midterm Exam in THC103 Quality Service Management in Tourim and Hospitality IndustryDokument6 SeitenMidterm Exam in THC103 Quality Service Management in Tourim and Hospitality IndustryRoy Cabarles100% (2)
- Session 1 - Life Cycle and Goal Setting - FinalDokument7 SeitenSession 1 - Life Cycle and Goal Setting - FinalLERKA LIEL ESTOLONIONoch keine Bewertungen