Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Current & Future Status of Herbal MedicinesDokument4 SeitenCurrent & Future Status of Herbal MedicinesimmchrNoch keine Bewertungen
- Traditional Medicine For The Rich and KnowledgeableDokument11 SeitenTraditional Medicine For The Rich and KnowledgeableKent MaravillosaNoch keine Bewertungen
- Utilization of Cam in AfricaDokument11 SeitenUtilization of Cam in AfricaKent MaravillosaNoch keine Bewertungen
- Obgyn DocumentationDokument13 SeitenObgyn DocumentationEli EidNoch keine Bewertungen
- Bagley 2006Dokument8 SeitenBagley 2006Kent MaravillosaNoch keine Bewertungen
- Case 1Dokument11 SeitenCase 1Kent MaravillosaNoch keine Bewertungen
- CPG Dengue Infection PDF FinalDokument82 SeitenCPG Dengue Infection PDF FinalTIong Tung WeiNoch keine Bewertungen
- I.elujobaetal 1Dokument16 SeitenI.elujobaetal 1Anonymous VPNZ1e28Us100% (1)
- Tay SachsDokument8 SeitenTay SachssyringomyeliaNoch keine Bewertungen
- Arrhythmias: M. Lacombe Mdfmr/Unecom July 22, 2009Dokument210 SeitenArrhythmias: M. Lacombe Mdfmr/Unecom July 22, 2009Kent MaravillosaNoch keine Bewertungen
- Nervous System ManuscriptDokument1 SeiteNervous System ManuscriptKent MaravillosaNoch keine Bewertungen
- Lit Crit in EnglishDokument1 SeiteLit Crit in EnglishKent MaravillosaNoch keine Bewertungen
- (TSG) Study Timetable TemplateDokument8 Seiten(TSG) Study Timetable Templatesatoni12Noch keine Bewertungen
- Rock and Roll PevDokument5 SeitenRock and Roll PevKent MaravillosaNoch keine Bewertungen
- Some Tools For ExergesisDokument5 SeitenSome Tools For ExergesisKent MaravillosaNoch keine Bewertungen
- Exer#15 FielDokument1 SeiteExer#15 FielKent MaravillosaNoch keine Bewertungen
- Qualitative Tests for CarbohydratesDokument15 SeitenQualitative Tests for CarbohydratesKent MaravillosaNoch keine Bewertungen
- Blood Banking and The Band Played On Reflection PaperDokument2 SeitenBlood Banking and The Band Played On Reflection PaperKent MaravillosaNoch keine Bewertungen
- Lit Crit in EnglishDokument1 SeiteLit Crit in EnglishKent MaravillosaNoch keine Bewertungen
- Lesson 8 Self AssessmentDokument49 SeitenLesson 8 Self AssessmentKent MaravillosaNoch keine Bewertungen
- Research On Bamboo AnticoagulantDokument2 SeitenResearch On Bamboo AnticoagulantKent MaravillosaNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (120)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- MINI PROJECT HOSPITAL .... Final AlterDokument7 SeitenMINI PROJECT HOSPITAL .... Final Alteryaazzoonn7788Noch keine Bewertungen
- Basics of Functional Echocardiography in Children and NeonatesDokument13 SeitenBasics of Functional Echocardiography in Children and Neonatestigtigrai49Noch keine Bewertungen
- Maryam Ahmadi Department of Health Services Management, School of Management and Medical Information Sciences, Vali Asr ST, Vanak SQ, Tehran, IranDokument19 SeitenMaryam Ahmadi Department of Health Services Management, School of Management and Medical Information Sciences, Vali Asr ST, Vanak SQ, Tehran, IraneScript-TeamNoch keine Bewertungen
- Case Study CHNDokument23 SeitenCase Study CHNKramer Dialola LacsonNoch keine Bewertungen
- Vaccination Sites Per Municipalities of South CotabatoDokument2 SeitenVaccination Sites Per Municipalities of South CotabatoHEMS SOCOTNoch keine Bewertungen
- Remdesivir Supplier Contact Status VerifiedDokument1 SeiteRemdesivir Supplier Contact Status VerifiedshawnNoch keine Bewertungen
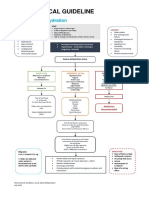
- AdultDehydrationGuidelineJuly2015 PDFDokument3 SeitenAdultDehydrationGuidelineJuly2015 PDFmarselamgeNoch keine Bewertungen
- Top 10 Companies in European Hospital Beds MarketDokument4 SeitenTop 10 Companies in European Hospital Beds MarketClassic BobbyNoch keine Bewertungen
- Kinesio Tape Courses Presents: Fundamentals and Advanced Kinesio Taping (KT1 and KT2)Dokument2 SeitenKinesio Tape Courses Presents: Fundamentals and Advanced Kinesio Taping (KT1 and KT2)Mirelle_73Noch keine Bewertungen
- Familiar. Reliable. Affordable.: GE HealthcareDokument6 SeitenFamiliar. Reliable. Affordable.: GE Healthcarecheng fengNoch keine Bewertungen
- The Culture of Healthcare: Sociotechnical Aspects: Clinicians and TechnologyDokument19 SeitenThe Culture of Healthcare: Sociotechnical Aspects: Clinicians and TechnologyHealth IT Workforce Curriculum - 2012Noch keine Bewertungen
- Case Study: Improving Quality and Finances at Blake Memorial HospitalDokument2 SeitenCase Study: Improving Quality and Finances at Blake Memorial HospitalMai Dương Quang HuyNoch keine Bewertungen
- (Oxford Handbooks in Nursing. - Oxford Medical Publications) Kisiel, Maria - Radford, Mark - Smith, Alison - Oxford Handbook of Surgical Nursing (2016, Oxford University Press)Dokument787 Seiten(Oxford Handbooks in Nursing. - Oxford Medical Publications) Kisiel, Maria - Radford, Mark - Smith, Alison - Oxford Handbook of Surgical Nursing (2016, Oxford University Press)Nganu AjaNoch keine Bewertungen
- Funda QuestionsDokument3 SeitenFunda QuestionsJennifer TumbokonNoch keine Bewertungen
- Clinical Biochemistry & Analytical ToxicologyDokument4 SeitenClinical Biochemistry & Analytical ToxicologyRohit Manakchand ZawarNoch keine Bewertungen
- Reducing Oncology Discharge TimeDokument7 SeitenReducing Oncology Discharge Timedrbhavya250% (1)
- Dr. Jose Fabella Memorial HospitalDokument2 SeitenDr. Jose Fabella Memorial HospitalMarc Jason Cruz DelomenNoch keine Bewertungen
- AHM Black White Boost FlexiDokument10 SeitenAHM Black White Boost FlexiDani Kirky Ylagan100% (1)
- CLRT Final ProjectDokument28 SeitenCLRT Final Projectapi-358148089Noch keine Bewertungen
- Teacher Confesses Feelings for StudentDokument9 SeitenTeacher Confesses Feelings for StudentZaboomafoo Thelemur100% (2)
- 08 Aug 2015Dokument76 Seiten08 Aug 2015RajabSaputraNoch keine Bewertungen
- Health Care Facilities PDFDokument12 SeitenHealth Care Facilities PDFshaaban2009Noch keine Bewertungen
- Advantages and Disadvantages For Nurses of Using Social MediaDokument3 SeitenAdvantages and Disadvantages For Nurses of Using Social Mediajoana marie reyesNoch keine Bewertungen
- Despersion NumericalsDokument15 SeitenDespersion NumericalsShubhamNoch keine Bewertungen
- Umbilical Granuloma: Modern Understanding of Etiopathogenesis, Diagnosis, and ManagementDokument6 SeitenUmbilical Granuloma: Modern Understanding of Etiopathogenesis, Diagnosis, and ManagementSari DewiNoch keine Bewertungen
- Application of ABC Method in Hospital ManagementDokument6 SeitenApplication of ABC Method in Hospital ManagementFreddy VargasNoch keine Bewertungen
- Patient Care Delivery SystemDokument13 SeitenPatient Care Delivery SystemAiza Apelada-NievaNoch keine Bewertungen
- Ect SopDokument6 SeitenEct Sopqonita0% (1)
- Focus-Pdca For Specimen ErrorsDokument3 SeitenFocus-Pdca For Specimen Errorsapi-252498131Noch keine Bewertungen
- Dental Implants - An Evolving Discipline - An Issue of Oral and Maxillofacial Clinics of North America (The Clinics - Dentistry) (UnitedVRG)Dokument182 SeitenDental Implants - An Evolving Discipline - An Issue of Oral and Maxillofacial Clinics of North America (The Clinics - Dentistry) (UnitedVRG)George TătarNoch keine Bewertungen