Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
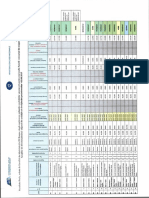
- Assessment of Validity Inconsistency IndexDokument1 SeiteAssessment of Validity Inconsistency Indexsara100% (1)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Common Psychiatric TermsDokument6 SeitenCommon Psychiatric TermsKatrina Heart Rauto AvilaNoch keine Bewertungen
- Organisation ClimateDokument5 SeitenOrganisation ClimateLavander MeggieNoch keine Bewertungen
- PD DSM 4 Vs 5Dokument15 SeitenPD DSM 4 Vs 5satish2k3Noch keine Bewertungen
- Review of - I - The Social Problems of An Industrial Civilization - IDokument3 SeitenReview of - I - The Social Problems of An Industrial Civilization - ILavander MeggieNoch keine Bewertungen
- Programul de Training Integrat Transformational - CBC RomaniaDokument5 SeitenProgramul de Training Integrat Transformational - CBC RomaniaLavander MeggieNoch keine Bewertungen
- Donini Orthorexia Nervosa Dimension of The Phenomena PDFDokument7 SeitenDonini Orthorexia Nervosa Dimension of The Phenomena PDFLavander MeggieNoch keine Bewertungen
- Carte Hospital Days-Treatment WaisDokument32 SeitenCarte Hospital Days-Treatment WaisLavander Meggie100% (1)
- BV Rezultat Final ConcursDokument5 SeitenBV Rezultat Final ConcursLavander MeggieNoch keine Bewertungen
- Download Gramatica Limbii Engleze PDF & Learn English GrammarDokument2 SeitenDownload Gramatica Limbii Engleze PDF & Learn English GrammarLavander MeggieNoch keine Bewertungen
- Cognitive Behavioral Therapy For Psychotic SymptomsDokument149 SeitenCognitive Behavioral Therapy For Psychotic SymptomsCrina SerbanNoch keine Bewertungen
- Creative Methods Metaphor in Psychotherapy PDFDokument42 SeitenCreative Methods Metaphor in Psychotherapy PDFLavander MeggieNoch keine Bewertungen
- Behavioural and Cognitive PsychotherapyDokument4 SeitenBehavioural and Cognitive PsychotherapyLavander MeggieNoch keine Bewertungen
- Recent Univ Baltimore Fonduri Guv 2011Dokument71 SeitenRecent Univ Baltimore Fonduri Guv 2011Lavander MeggieNoch keine Bewertungen
- 2013 Sample Psychology Cover LettersDokument2 Seiten2013 Sample Psychology Cover LettersLavander Meggie100% (1)
- © (P) Twin Sisters IP, LLC. All Rights ReservedDokument4 Seiten© (P) Twin Sisters IP, LLC. All Rights ReservedLavander MeggieNoch keine Bewertungen
- Attentive judges at the European Games in BakuDokument21 SeitenAttentive judges at the European Games in BakuLavander MeggieNoch keine Bewertungen
- Couture Dress Pattern InstructionsDokument10 SeitenCouture Dress Pattern InstructionsMazZzingerZ100% (4)
- Flagellated Protozoan Parasite Giardiasis Epithelium Ventral Binary Fission Gastro-Intestinal Tract Lumen Trophozoites AnaerobesDokument6 SeitenFlagellated Protozoan Parasite Giardiasis Epithelium Ventral Binary Fission Gastro-Intestinal Tract Lumen Trophozoites AnaerobesLavander MeggieNoch keine Bewertungen
- Nasha Mukti Kendra Bhopal PDFDokument4 SeitenNasha Mukti Kendra Bhopal PDFshrishuddhi1Noch keine Bewertungen
- Transcultural Psychiatry: Cultural Difference, Universalism and Social Psychiatry in The Age of DecolonisationDokument26 SeitenTranscultural Psychiatry: Cultural Difference, Universalism and Social Psychiatry in The Age of DecolonisationJinyoung ChangNoch keine Bewertungen
- Book Chums Interview With Sam VakninDokument6 SeitenBook Chums Interview With Sam VakninzadanliranNoch keine Bewertungen
- Caz 4Dokument17 SeitenCaz 4Marinela MeliszekNoch keine Bewertungen
- A Somatic Symptom DisorderDokument2 SeitenA Somatic Symptom DisorderAbdul Nisar JilaniNoch keine Bewertungen
- Scrupulosity in OCDDokument17 SeitenScrupulosity in OCDMiztaloges86Noch keine Bewertungen
- Icd 10Dokument3 SeitenIcd 10boblishNoch keine Bewertungen
- Substance Abuse & Mental HealthDokument1 SeiteSubstance Abuse & Mental Healthkaitlin100% (1)
- Causes and Types of Mental DisordersDokument12 SeitenCauses and Types of Mental DisordersJay-Jay Bordeos100% (1)
- Ang Mga Pananaw at Opinyon NG Pag-Uulat NG Mag-Uulat Sa Programang Ito Ay Hindi Ang Pangunahing Posisyon O Pahayag NG Organisasyon ItoDokument16 SeitenAng Mga Pananaw at Opinyon NG Pag-Uulat NG Mag-Uulat Sa Programang Ito Ay Hindi Ang Pangunahing Posisyon O Pahayag NG Organisasyon ItoRoilan MarlangNoch keine Bewertungen
- Annotated Bibliography On Depression Versus DramatizationDokument4 SeitenAnnotated Bibliography On Depression Versus Dramatizationapi-267761791Noch keine Bewertungen
- A Balanced Psychology and A Full LifeDokument4 SeitenA Balanced Psychology and A Full LifeonetimeitNoch keine Bewertungen
- ASESSMENTDokument49 SeitenASESSMENTPUSAT LATIHAN AADK0% (1)
- Negative Symptoms EQZ Lancet ReviewDokument14 SeitenNegative Symptoms EQZ Lancet ReviewConstanza González GutiérrezNoch keine Bewertungen
- Taking A History of DEPRESSIONDokument3 SeitenTaking A History of DEPRESSIONPrarthana Thiagarajan100% (13)
- OcdDokument5 SeitenOcdapi-314105403Noch keine Bewertungen
- Schizoaffective Disorder and Depression. A Case Study of A Patient From Ceará, BrazilDokument8 SeitenSchizoaffective Disorder and Depression. A Case Study of A Patient From Ceará, Braziljeremy ludwigNoch keine Bewertungen
- Personality Disorders ChartDokument11 SeitenPersonality Disorders ChartSolomon Seth Sallfors100% (1)
- Mitigation Declaration For Daniel Wayne CookDokument19 SeitenMitigation Declaration For Daniel Wayne CookTucsonSentinelNoch keine Bewertungen
- Depression The Soul Hungry VirusDokument6 SeitenDepression The Soul Hungry Virusapi-476496559Noch keine Bewertungen
- Holaway Et Al Intolerance of Uncertainty in OCD and GAD J Anxiety Disorders 2006Dokument17 SeitenHolaway Et Al Intolerance of Uncertainty in OCD and GAD J Anxiety Disorders 2006Jean BoutiereNoch keine Bewertungen
- Sluggish cognitive tempo associated with autistic traits and anxiety in children with ADHDDokument7 SeitenSluggish cognitive tempo associated with autistic traits and anxiety in children with ADHDmariliaNoch keine Bewertungen
- Schizoaffective Disorder: Andreas MarnerosDokument8 SeitenSchizoaffective Disorder: Andreas MarnerosArya LekshmiNoch keine Bewertungen
- Performance Task in Personal Development (Depression) : Submitted By: Submitted ToDokument6 SeitenPerformance Task in Personal Development (Depression) : Submitted By: Submitted ToJanea Arinya100% (1)
- RestrainingDokument9 SeitenRestrainingRavi PaulNoch keine Bewertungen
- Schizoid Personality Disorder: Social Withdrawal and Lack of EmotionDokument3 SeitenSchizoid Personality Disorder: Social Withdrawal and Lack of EmotionEzraManzanoNoch keine Bewertungen
- Bipolar 1 PDFDokument10 SeitenBipolar 1 PDFPrecious Ann ParelNoch keine Bewertungen
- A New Empirical Definition of Major Depressive Episode Recovery and Its Positive Impact On Future Course of IllnessDokument19 SeitenA New Empirical Definition of Major Depressive Episode Recovery and Its Positive Impact On Future Course of Illnessleeperlhan2000Noch keine Bewertungen