Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Lavender Lavender Lavender Lavender Lavender Lavender: UrineDokument3 SeitenLavender Lavender Lavender Lavender Lavender Lavender: UrineJonathan A. Sarmiento67% (6)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Manual On Quality Standads For HIV Testing Laboratories PDFDokument137 SeitenManual On Quality Standads For HIV Testing Laboratories PDFkandarpvyasa5930Noch keine Bewertungen
- Lupus GuideDokument154 SeitenLupus GuideKathleen Sia100% (2)
- Rheumatology Notes From DR Osama LecturesDokument76 SeitenRheumatology Notes From DR Osama LecturesMohamed ElAyadiNoch keine Bewertungen
- Pod Uveitis Book RevDokument252 SeitenPod Uveitis Book Revelika dwi100% (1)
- Combatting COVID-19: A 10-Point Summary On Diet, Nutrition and The Role of MicronutrientsDokument8 SeitenCombatting COVID-19: A 10-Point Summary On Diet, Nutrition and The Role of Micronutrientskandarpvyasa5930Noch keine Bewertungen
- Combatting COVID-19: A 10-Point Summary On Diet, Nutrition and The Role of MicronutrientsDokument8 SeitenCombatting COVID-19: A 10-Point Summary On Diet, Nutrition and The Role of Micronutrientskandarpvyasa5930Noch keine Bewertungen
- PR4100 Microplate Reader ManualDokument224 SeitenPR4100 Microplate Reader Manualkandarpvyasa5930Noch keine Bewertungen
- CPC16-RBC-Common Sense Pathology-CBC PDFDokument7 SeitenCPC16-RBC-Common Sense Pathology-CBC PDFkandarpvyasa5930Noch keine Bewertungen
- The Clinical Utility of Zonulin Testing Is Limited Due to Lack of Sensitivity, Specificity and ReproducibilityDokument3 SeitenThe Clinical Utility of Zonulin Testing Is Limited Due to Lack of Sensitivity, Specificity and Reproducibilitykandarpvyasa5930Noch keine Bewertungen
- Seroreactive Marker For Inflammatory Bowel DiseaseDokument22 SeitenSeroreactive Marker For Inflammatory Bowel Diseasekandarpvyasa5930Noch keine Bewertungen
- Unitaid and CHAI announce agreement with Omega Diagnostics to increase access to new, instrument-free CD4 test for people living with HIV in over 130 low- and middle-income countries - Clinton Health Access InitiativeDokument6 SeitenUnitaid and CHAI announce agreement with Omega Diagnostics to increase access to new, instrument-free CD4 test for people living with HIV in over 130 low- and middle-income countries - Clinton Health Access Initiativekandarpvyasa5930Noch keine Bewertungen
- The Clinical Utility of Zonulin Testing Is Limited Due to Lack of Sensitivity, Specificity and ReproducibilityDokument3 SeitenThe Clinical Utility of Zonulin Testing Is Limited Due to Lack of Sensitivity, Specificity and Reproducibilitykandarpvyasa5930Noch keine Bewertungen
- Unitaid and CHAI announce agreement with Omega Diagnostics to increase access to new, instrument-free CD4 test for people living with HIV in over 130 low- and middle-income countries - Clinton Health Access InitiativeDokument6 SeitenUnitaid and CHAI announce agreement with Omega Diagnostics to increase access to new, instrument-free CD4 test for people living with HIV in over 130 low- and middle-income countries - Clinton Health Access Initiativekandarpvyasa5930Noch keine Bewertungen
- The Hiv AIDS Charity For LifeDokument12 SeitenThe Hiv AIDS Charity For Lifekandarpvyasa5930Noch keine Bewertungen
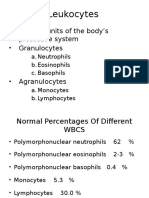
- WBCs 1Dokument21 SeitenWBCs 1kandarpvyasa5930Noch keine Bewertungen
- Gita SarDokument17 SeitenGita Sarkushal jaitwaniNoch keine Bewertungen
- The Immune SystemDokument6 SeitenThe Immune Systemkandarpvyasa5930Noch keine Bewertungen
- ANCAfor Crohns Diseaseand Ulcerative ColitisDokument31 SeitenANCAfor Crohns Diseaseand Ulcerative Colitiskandarpvyasa5930Noch keine Bewertungen
- Food Elimination Based On IgG AntibodiesDokument6 SeitenFood Elimination Based On IgG Antibodieskandarpvyasa5930Noch keine Bewertungen
- Ana Testing - AACCDokument8 SeitenAna Testing - AACCkandarpvyasa5930Noch keine Bewertungen
- Antibodies Against Food Antigens in Patients With Autistic Spectrum DisordersDokument11 SeitenAntibodies Against Food Antigens in Patients With Autistic Spectrum Disorderskandarpvyasa5930Noch keine Bewertungen
- Using Conditional Formatting To Highlight Positives, or Any Sample of InterestDokument3 SeitenUsing Conditional Formatting To Highlight Positives, or Any Sample of Interestkandarpvyasa5930Noch keine Bewertungen
- Male Reproductive System: Related Kidshealth LinksDokument7 SeitenMale Reproductive System: Related Kidshealth Linkskandarpvyasa5930Noch keine Bewertungen
- IgG Vs IgE PDFDokument2 SeitenIgG Vs IgE PDFkandarpvyasa5930Noch keine Bewertungen
- Value of Serum ECP and IgE in Differentiating Between Asthma and COPDDokument7 SeitenValue of Serum ECP and IgE in Differentiating Between Asthma and COPDkandarpvyasa5930Noch keine Bewertungen
- Immunology Selfandnon Selffromaphenomenologicalpointofview 131229151657 Phpapp01Dokument74 SeitenImmunology Selfandnon Selffromaphenomenologicalpointofview 131229151657 Phpapp01kandarpvyasa5930100% (1)
- Randomised Controlled Trial of Food Elimination Diet Based On IgGDokument9 SeitenRandomised Controlled Trial of Food Elimination Diet Based On IgGkandarpvyasa5930Noch keine Bewertungen
- Diet Restriction in Migraine, Based On IgG Against Foods PDFDokument9 SeitenDiet Restriction in Migraine, Based On IgG Against Foods PDFkandarpvyasa5930Noch keine Bewertungen
- Systemic Lupus Erythematosus PathophysiologyDokument8 SeitenSystemic Lupus Erythematosus PathophysiologyAnonymous OU6w8lX9Noch keine Bewertungen
- Ataxiachhetri 2014Dokument10 SeitenAtaxiachhetri 2014david arredondoNoch keine Bewertungen
- Laboratory Diagnosis of Hypersensitivity and AutoimmunityDokument41 SeitenLaboratory Diagnosis of Hypersensitivity and AutoimmunityDenish Calmax AngolNoch keine Bewertungen
- Advances in SLE managementDokument9 SeitenAdvances in SLE managementDaniela HernándezNoch keine Bewertungen
- Mimickers of UrticariaDokument9 SeitenMimickers of UrticariaNaeNoch keine Bewertungen
- Pathology ReviewDokument430 SeitenPathology Reviewpatriciacaf100% (2)
- Lab Tests Help Diagnose LupusDokument4 SeitenLab Tests Help Diagnose LupusLukes GutierrezNoch keine Bewertungen
- Diagnosis and Management of Pediatric Autoimmune PDFDokument16 SeitenDiagnosis and Management of Pediatric Autoimmune PDFRamina PasariNoch keine Bewertungen
- Nutrition and Rheumatic Disease PDFDokument304 SeitenNutrition and Rheumatic Disease PDFnamnamanm joonieNoch keine Bewertungen
- Systemic Lupous Erythematosus (SLE) Part 2Dokument68 SeitenSystemic Lupous Erythematosus (SLE) Part 2Power La Victoria Floro100% (3)
- Rheumatology MedicineDokument19 SeitenRheumatology MedicineSami Ur RehmanNoch keine Bewertungen
- Approach To The Patient With Muscle Weakness - UpToDateDokument12 SeitenApproach To The Patient With Muscle Weakness - UpToDatePatriciaNoch keine Bewertungen
- Osteo Arthritis and Inflammatory Arthritis: DR - Yanto Budiman. SP - Rad, M.Kes Bagian Radiologi FK/RS. Atma JayaDokument45 SeitenOsteo Arthritis and Inflammatory Arthritis: DR - Yanto Budiman. SP - Rad, M.Kes Bagian Radiologi FK/RS. Atma JayaMira FindoroNoch keine Bewertungen
- Incorrectly: CorrectlyDokument25 SeitenIncorrectly: CorrectlypikachuNoch keine Bewertungen
- Rheumatology & Rehabilitation 2018-2019Dokument57 SeitenRheumatology & Rehabilitation 2018-2019Selim TarekNoch keine Bewertungen
- Inova Catalog 2013Dokument56 SeitenInova Catalog 2013wangxuliang100% (1)
- PIEPIEDokument23 SeitenPIEPIEJaycee NodadoNoch keine Bewertungen
- Anemiile Aplastice Copii1Dokument28 SeitenAnemiile Aplastice Copii1Daniela LupanNoch keine Bewertungen
- 5Dokument275 Seiten5Carlos HernándezNoch keine Bewertungen
- Diseases of The Immune System: OBC 231 General PathologyDokument91 SeitenDiseases of The Immune System: OBC 231 General PathologyRana MohammadNoch keine Bewertungen
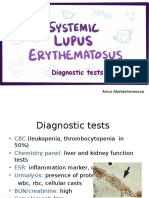
- PBL 3 - SLE (Diagnostic Tests)Dokument9 SeitenPBL 3 - SLE (Diagnostic Tests)Ainur AbdrakhmanovaNoch keine Bewertungen
- Delayed Hypersensitivity and Type IV ReactionsDokument12 SeitenDelayed Hypersensitivity and Type IV Reactionsella Sy100% (1)
- AASLD Guideline of Autoimmune Hepatitis PDFDokument52 SeitenAASLD Guideline of Autoimmune Hepatitis PDFPritam SahaNoch keine Bewertungen
- Clinical Manifestations and Diagnosis of Systemic Lupus Erythematosus in Adults - UpToDateDokument55 SeitenClinical Manifestations and Diagnosis of Systemic Lupus Erythematosus in Adults - UpToDateOlga BabiiNoch keine Bewertungen
- ATI RN Predictor Study NotesDokument20 SeitenATI RN Predictor Study NotesJennifer Vicioso100% (9)
- Connective Tissue DZDokument1 SeiteConnective Tissue DZAndre GarciaNoch keine Bewertungen