Das könnte Ihnen auch gefallen
- Transfusion Error and Near MissesDokument35 SeitenTransfusion Error and Near Missesanaeshkl100% (1)
- FlaggingDokument65 SeitenFlaggingTony KurniawanNoch keine Bewertungen
- Case Series AminaphtoneDokument3 SeitenCase Series AminaphtoneevalubisNoch keine Bewertungen
- Managing CKD: regular assessments, BP control, cardiovascular protectionDokument2 SeitenManaging CKD: regular assessments, BP control, cardiovascular protectionRifky Octavio PNoch keine Bewertungen
- Lumafusion Shortcuts LandscapeDokument2 SeitenLumafusion Shortcuts Landscapepocho clashNoch keine Bewertungen
- Serum Protein ElectrophoresisDokument9 SeitenSerum Protein Electrophoresiskiedd_04100% (4)
- Cancer of LarynxDokument29 SeitenCancer of LarynxQasim HaleimiNoch keine Bewertungen
- CRP vs ESR Clinical AuditDokument12 SeitenCRP vs ESR Clinical AuditLuke LauNoch keine Bewertungen
- WHO Handbook of Blood TranfusionDokument344 SeitenWHO Handbook of Blood TranfusionWan Zafirah100% (1)
- Saudi Council ExamDokument23 SeitenSaudi Council ExamFarooq MohammadNoch keine Bewertungen
- Fetal Growth Restriction ACOG 2013Dokument12 SeitenFetal Growth Restriction ACOG 2013Maverick 18100% (3)
- Levey Jennings ChartsDokument8 SeitenLevey Jennings Chartsmuhammad wajahat100% (3)
- TRALIDokument26 SeitenTRALIVirgina Destiana SuhendarNoch keine Bewertungen
- Hemoglobin Electrophoresis1Dokument19 SeitenHemoglobin Electrophoresis1nidaats100% (1)
- Chapter 8 Blood DonationDokument55 SeitenChapter 8 Blood DonationCHALIE MEQUNoch keine Bewertungen
- ImmunohematologyDokument38 SeitenImmunohematologyNoreenNoch keine Bewertungen
- UrinalysisDokument36 SeitenUrinalysisMarl EstradaNoch keine Bewertungen
- Blood TransfusionDokument38 SeitenBlood TransfusiontorkNoch keine Bewertungen
- Acinetobacter BaumanniiDokument53 SeitenAcinetobacter BaumanniiLaboratorium BorromeusNoch keine Bewertungen
- MDSDokument46 SeitenMDSFesti Mada HelmiNoch keine Bewertungen
- Coombs TestDokument13 SeitenCoombs TestPatNoppadolNoch keine Bewertungen
- Thalasemia RSCMDokument28 SeitenThalasemia RSCMAnonymous ujOv31SNoch keine Bewertungen
- Diagnosis and Management of Plasma Cell DisordersDokument23 SeitenDiagnosis and Management of Plasma Cell Disordersbubbu92Noch keine Bewertungen
- Eng9 - Q3 - M4 - W4 - Interpret The Message Conveyed in A Poster - V5Dokument19 SeitenEng9 - Q3 - M4 - W4 - Interpret The Message Conveyed in A Poster - V5FITZ100% (1)
- Overview of HIV and Its Management: Caroline Mills-Davies Emmanuel FantevieDokument101 SeitenOverview of HIV and Its Management: Caroline Mills-Davies Emmanuel FantevieImanuel Fantevie100% (1)
- Training Plan JDVP 2020 - BPP (40days)Dokument36 SeitenTraining Plan JDVP 2020 - BPP (40days)Shallimar Alcarion100% (1)
- CytomegalovirusDokument33 SeitenCytomegalovirustummalapalli venkateswara raoNoch keine Bewertungen
- CH-2.21 Analyte Reference Interval Instrumentation Methodology ChartDokument48 SeitenCH-2.21 Analyte Reference Interval Instrumentation Methodology ChartAli KING FREDDY100% (1)
- Spouses vs. Dev't Corp - Interest Rate on Promissory NotesDokument2 SeitenSpouses vs. Dev't Corp - Interest Rate on Promissory NotesReinQZNoch keine Bewertungen
- Pancytopenia As Initial Presentation of Acute Lymphoblastic Leukemia and Its Associationwith Bone MarrowresponseDokument6 SeitenPancytopenia As Initial Presentation of Acute Lymphoblastic Leukemia and Its Associationwith Bone MarrowresponseIJAR JOURNALNoch keine Bewertungen
- Immature Platelet Fraction (IPF)Dokument5 SeitenImmature Platelet Fraction (IPF)asankandessNoch keine Bewertungen
- Managing Tuberculosis in PregnancyDokument1 SeiteManaging Tuberculosis in PregnancyAndi Tenri Ola Oddang IINoch keine Bewertungen
- Diagnosis and Treatment of Lupus NephritisDokument34 SeitenDiagnosis and Treatment of Lupus NephritisDr Edi Hidayat100% (1)
- Antepartum Haemmorhage and Breaking Bad News - OSCE Mark SchemeDokument2 SeitenAntepartum Haemmorhage and Breaking Bad News - OSCE Mark Schemeespiria100% (2)
- Fetal Lung MaturityDokument17 SeitenFetal Lung MaturityAkbarNovan100% (1)
- Chapter 11 Clinical Laboratory InstrumentationDokument19 SeitenChapter 11 Clinical Laboratory InstrumentationAnonymous 58LGc3Noch keine Bewertungen
- DR Wifanto S Jeo, SPB-BD - Acute AbdomenDokument28 SeitenDR Wifanto S Jeo, SPB-BD - Acute AbdomenIrma DamayantiNoch keine Bewertungen
- Kurva Disosiasi HB OksigenDokument6 SeitenKurva Disosiasi HB Oksigenhendra_darmawan_4Noch keine Bewertungen
- Intinsic PEEP, Gas Trapping and The Expiratory Hold ManoeuvreDokument1 SeiteIntinsic PEEP, Gas Trapping and The Expiratory Hold ManoeuvreKhairiyah MahalilNoch keine Bewertungen
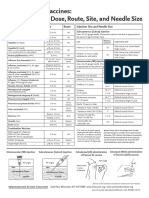
- Administering Vaccines: Dose, Route, Site and Needle Size GuideDokument1 SeiteAdministering Vaccines: Dose, Route, Site and Needle Size GuideKate Lucernas MayugaNoch keine Bewertungen
- AKI Vs CKD Lecture Latest 3rd Dec 2018Dokument51 SeitenAKI Vs CKD Lecture Latest 3rd Dec 2018mugilessNoch keine Bewertungen
- Fresh Frozen Plasma (FFP)Dokument1 SeiteFresh Frozen Plasma (FFP)Prajatiya HarwokoNoch keine Bewertungen
- Bimbingan ThoraksDokument71 SeitenBimbingan ThoraksHedya Nadhrati SururaNoch keine Bewertungen
- MycoDot PIDokument4 SeitenMycoDot PITanveer100% (1)
- Intrauterine Fetal Transfusion of Red Blood CellsDokument16 SeitenIntrauterine Fetal Transfusion of Red Blood CellsHervi LaksariNoch keine Bewertungen
- Validity and importance of harm resultsDokument2 SeitenValidity and importance of harm resultsFekhaza AlfarissiNoch keine Bewertungen
- Serological Markers of HBV InfectionDokument8 SeitenSerological Markers of HBV InfectioncristieristiieNoch keine Bewertungen
- Rational Blood Transfusion in Infant and ChildrenDokument37 SeitenRational Blood Transfusion in Infant and ChildrenBayu KurniawanNoch keine Bewertungen
- Cross MatchingDokument2 SeitenCross MatchingHimanshu_0Noch keine Bewertungen
- CEBM Levels of EvidenceDokument2 SeitenCEBM Levels of EvidenceBellatriix Bonisa MadarjaNoch keine Bewertungen
- HAEMOPOIESISDokument6 SeitenHAEMOPOIESISDiyana ZahariNoch keine Bewertungen
- Thrombopoiesis and Megakaryopoiesis: BY Dr. Etu-Efeotor T. PDokument22 SeitenThrombopoiesis and Megakaryopoiesis: BY Dr. Etu-Efeotor T. PPrincewill SeiyefaNoch keine Bewertungen
- Hiv-Associated Nephropathy (Hivan) : DR KibaruDokument27 SeitenHiv-Associated Nephropathy (Hivan) : DR KibaruMalueth AnguiNoch keine Bewertungen
- Microcytic Anemia PDFDokument8 SeitenMicrocytic Anemia PDFMargarita TorresNoch keine Bewertungen
- ABO Blood Group DiscrepanciesDokument9 SeitenABO Blood Group DiscrepanciesRichard SiahaanNoch keine Bewertungen
- Multiple Myeloma OverviewDokument52 SeitenMultiple Myeloma OverviewanmegpraNoch keine Bewertungen
- Hemoblastosis in ChildrenDokument40 SeitenHemoblastosis in ChildrenAli Baker Algelane100% (3)
- Massive Blood Transfusion Protocol (MBTP) Definition and ManagementDokument17 SeitenMassive Blood Transfusion Protocol (MBTP) Definition and ManagementevanNoch keine Bewertungen
- Boys Simplified Field Tables Weight For Length Birth To 2 Years (Percentiles)Dokument5 SeitenBoys Simplified Field Tables Weight For Length Birth To 2 Years (Percentiles)Gabrielly Lopes100% (1)
- HarrisADVIA2120methods LabHema2005 11 47-61 PDFDokument16 SeitenHarrisADVIA2120methods LabHema2005 11 47-61 PDFedu_14cNoch keine Bewertungen
- Thalassemia: Red Cell DisordersDokument27 SeitenThalassemia: Red Cell DisorderstitisNoch keine Bewertungen
- Bhutan National Standards BT ServicesDokument98 SeitenBhutan National Standards BT ServicesDarla YsavelNoch keine Bewertungen
- Safe Blood UseDokument2 SeitenSafe Blood UseAnnette LowryNoch keine Bewertungen
- Operative Blood Transfusion Quality Improvement AuditDokument4 SeitenOperative Blood Transfusion Quality Improvement AuditMerhan FoudaNoch keine Bewertungen
- Blood Bank Technology Specialist - The Comprehensive Guide: Vanguard ProfessionalsVon EverandBlood Bank Technology Specialist - The Comprehensive Guide: Vanguard ProfessionalsNoch keine Bewertungen
- Catalogo 4life en InglesDokument40 SeitenCatalogo 4life en InglesJordanramirezNoch keine Bewertungen
- Keyboard notes to Fur Elise melodyDokument2 SeitenKeyboard notes to Fur Elise melodyReji SarsalejoNoch keine Bewertungen
- Real Vs Nominal Values (Blank)Dokument4 SeitenReal Vs Nominal Values (Blank)Prineet AnandNoch keine Bewertungen
- 3 CRIM LAW 2 CASES TO BE DIGESTED Gambling Malfeasance Misfeasance Bribery Graft Corruption and MalversationDokument130 Seiten3 CRIM LAW 2 CASES TO BE DIGESTED Gambling Malfeasance Misfeasance Bribery Graft Corruption and MalversationElma MalagionaNoch keine Bewertungen
- RTS PMR Question Bank Chapter 2 2008Dokument7 SeitenRTS PMR Question Bank Chapter 2 2008iwan93Noch keine Bewertungen
- Meesho FDokument75 SeitenMeesho FAyan khanNoch keine Bewertungen
- MAT 1100 Mathematical Literacy For College StudentsDokument4 SeitenMAT 1100 Mathematical Literacy For College StudentsCornerstoneFYENoch keine Bewertungen
- KINGS OF TURKS - TURKISH ROYALTY Descent-LinesDokument8 SeitenKINGS OF TURKS - TURKISH ROYALTY Descent-Linesaykutovski100% (1)
- Connotative Vs Denotative Lesson Plan PDFDokument5 SeitenConnotative Vs Denotative Lesson Plan PDFangiela goc-ongNoch keine Bewertungen
- Fundamentals of Analytics in Practice /TITLEDokument43 SeitenFundamentals of Analytics in Practice /TITLEAcad ProgrammerNoch keine Bewertungen
- Class Namespace DesciptionDokument9 SeitenClass Namespace DesciptionĐào Quỳnh NhưNoch keine Bewertungen
- The 4Ps of Labor: Passenger, Passageway, Powers, and PlacentaDokument4 SeitenThe 4Ps of Labor: Passenger, Passageway, Powers, and PlacentaMENDIETA, JACQUELINE V.Noch keine Bewertungen
- WSP - Aci 318-02 Shear Wall DesignDokument5 SeitenWSP - Aci 318-02 Shear Wall DesignSalomi Ann GeorgeNoch keine Bewertungen
- Deforestation Contributes To Global Warming: Bruno GERVETDokument11 SeitenDeforestation Contributes To Global Warming: Bruno GERVETMajid JatoiNoch keine Bewertungen
- Amnesia: A Game of Remembering YourselfDokument11 SeitenAmnesia: A Game of Remembering YourselfNina JonesNoch keine Bewertungen
- Ethanox 330 Antioxidant: Safety Data SheetDokument7 SeitenEthanox 330 Antioxidant: Safety Data Sheetafryan azhar kurniawanNoch keine Bewertungen
- 1 Minute Witness PDFDokument8 Seiten1 Minute Witness PDFMark Aldwin LopezNoch keine Bewertungen
- Segmenting, Targeting, and Positioning (STP)Dokument16 SeitenSegmenting, Targeting, and Positioning (STP)Rachmat PutraNoch keine Bewertungen
- Agile Process ModelsDokument15 SeitenAgile Process ModelsShadrack KimutaiNoch keine Bewertungen
- Configure Initial ISAM Network SettingsDokument4 SeitenConfigure Initial ISAM Network SettingsnelusabieNoch keine Bewertungen
- Practise Active and Passive Voice History of Central Europe: I Lead-InDokument4 SeitenPractise Active and Passive Voice History of Central Europe: I Lead-InCorina LuchianaNoch keine Bewertungen
- Evirtualguru Computerscience 43 PDFDokument8 SeitenEvirtualguru Computerscience 43 PDFJAGANNATH THAWAITNoch keine Bewertungen
- Pashmina vs Cashmere: Which Luxury Fiber Is SofterDokument15 SeitenPashmina vs Cashmere: Which Luxury Fiber Is SofterSJVN CIVIL DESIGN100% (1)
- Calvo, G (1988) - Servicing The Public Debt - The Role of ExpectationsDokument16 SeitenCalvo, G (1988) - Servicing The Public Debt - The Role of ExpectationsDaniela SanabriaNoch keine Bewertungen
- Gender and DelinquencyDokument26 SeitenGender and DelinquencyCompis Jenny-annNoch keine Bewertungen