Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- EFire Brochure v6Dokument2 SeitenEFire Brochure v6apurvaapurva100% (1)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Nonparametric Testing in Excel PDFDokument72 SeitenNonparametric Testing in Excel PDFyudi_2008Noch keine Bewertungen
- Excel Calculation (T-Test and Toolpak)Dokument6 SeitenExcel Calculation (T-Test and Toolpak)Benmark JabayNoch keine Bewertungen
- Sepsis YaDokument22 SeitenSepsis YaGita ListawatiNoch keine Bewertungen
- Effects On Clinical Outcomes of Adding Dipeptidyl Peptidase-4 Inhibitors VersusDokument19 SeitenEffects On Clinical Outcomes of Adding Dipeptidyl Peptidase-4 Inhibitors VersusGita ListawatiNoch keine Bewertungen
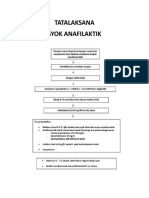
- Protap Syok AnafilaktikDokument1 SeiteProtap Syok AnafilaktikGita ListawatiNoch keine Bewertungen
- Tics SeverityDokument10 SeitenTics SeverityGita ListawatiNoch keine Bewertungen
- Chest RadiographyDokument23 SeitenChest Radiographyapi-3773951100% (2)
- J Neurol Neurosurg Psychiatry 2013 Sharma 1302 8Dokument8 SeitenJ Neurol Neurosurg Psychiatry 2013 Sharma 1302 8Gita ListawatiNoch keine Bewertungen
- Screening of Asymptomatic Children For Tuberculosis:: Is A Lateral Chest Radiograph Routinely Indicated?Dokument7 SeitenScreening of Asymptomatic Children For Tuberculosis:: Is A Lateral Chest Radiograph Routinely Indicated?jayyidahafifahNoch keine Bewertungen
- Review ArticleDokument7 SeitenReview ArticleDeddy ArionesyaNoch keine Bewertungen
- OutDokument7 SeitenOutAnggie BP DiponegoroNoch keine Bewertungen
- Changes in Intraocular Pressure After Pharmacologic Pupil DilationDokument5 SeitenChanges in Intraocular Pressure After Pharmacologic Pupil DilationAnggie BP DiponegoroNoch keine Bewertungen
- Jurnal THT 2Dokument3 SeitenJurnal THT 2Gita ListawatiNoch keine Bewertungen
- Anestesi Tracheal IntubationDokument4 SeitenAnestesi Tracheal IntubationGita ListawatiNoch keine Bewertungen
- In Vitro: Differential Diagnosis of Clavus and Verruca by A Predictive Model Generated From Electrical ImpedanceDokument7 SeitenIn Vitro: Differential Diagnosis of Clavus and Verruca by A Predictive Model Generated From Electrical ImpedanceGita ListawatiNoch keine Bewertungen
- Jurnal ReadingDokument5 SeitenJurnal ReadingGita ListawatiNoch keine Bewertungen
- j.1469-0691.2012.03798.x.pdf Scabies Journal PDFDokument11 Seitenj.1469-0691.2012.03798.x.pdf Scabies Journal PDFHafich ErnandaNoch keine Bewertungen
- Jcad 7 10 20Dokument8 SeitenJcad 7 10 20Gita ListawatiNoch keine Bewertungen
- Handbook: For Clinical Management of DengueDokument124 SeitenHandbook: For Clinical Management of DengueraattaiNoch keine Bewertungen
- Scabies in The Developing World - Its Prevalence, Complications, and ManagementDokument15 SeitenScabies in The Developing World - Its Prevalence, Complications, and ManagementGita ListawatiNoch keine Bewertungen
- P ('t':'3', 'I':'176969959') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Dokument10 SeitenP ('t':'3', 'I':'176969959') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Cecep Saeful HudaNoch keine Bewertungen
- Eritroderma CaseDokument7 SeitenEritroderma CaseGita ListawatiNoch keine Bewertungen
- AppendiksDokument6 SeitenAppendiksGita ListawatiNoch keine Bewertungen
- AppendiksDokument6 SeitenAppendiksGita ListawatiNoch keine Bewertungen
- 2000 Nobel Prize Winner in MedicineDokument2 Seiten2000 Nobel Prize Winner in MedicineGita ListawatiNoch keine Bewertungen
- Growth Charts (Kurva Pertumbuhan Anak CDC-NCHS)Dokument10 SeitenGrowth Charts (Kurva Pertumbuhan Anak CDC-NCHS)Gita ListawatiNoch keine Bewertungen
- Chemistry - Pharmacology and Toxicology of Methamphetamine and Related Designer DrugsDokument377 SeitenChemistry - Pharmacology and Toxicology of Methamphetamine and Related Designer DrugsAlfonso BallestasNoch keine Bewertungen
- Rupture of MembranesDokument8 SeitenRupture of MembranesSa'adah Munawaroh HDNoch keine Bewertungen
- Randomize Trial Treatment Varicose VeinsDokument10 SeitenRandomize Trial Treatment Varicose VeinsGita ListawatiNoch keine Bewertungen
- Ms. Annieska Alde Instructor ApplicantDokument2 SeitenMs. Annieska Alde Instructor ApplicantMaria AnnieskaNoch keine Bewertungen
- Your Instructions Are Not Always HelpfuDokument10 SeitenYour Instructions Are Not Always Helpfupatricio silvaNoch keine Bewertungen
- Good High School Research Paper TopicsDokument7 SeitenGood High School Research Paper Topicswpuzxcbkf100% (1)
- COMPONENT 3 - Curriculum ExperiencesDokument15 SeitenCOMPONENT 3 - Curriculum ExperiencesJayCesar67% (3)
- Operations ResearchDokument2 SeitenOperations ResearchIshant Bansal100% (4)
- Behaviour Response Flow Chart 5 Nov 2012Dokument1 SeiteBehaviour Response Flow Chart 5 Nov 2012jakilaNoch keine Bewertungen
- Self-Organizing Map and Cellular Automata CombinedDokument8 SeitenSelf-Organizing Map and Cellular Automata CombinedMarco Antonio Reséndiz DíazNoch keine Bewertungen
- Geography and PlanningDokument41 SeitenGeography and PlanningbolindroNoch keine Bewertungen
- An Investigation of The Factors Affecting Customer Based Brand Equity: A Case of Burger King, SubangDokument6 SeitenAn Investigation of The Factors Affecting Customer Based Brand Equity: A Case of Burger King, SubangBridgestone55Noch keine Bewertungen
- Analyzing Noise Robustness of MFCC and GFCC Features in Speaker IdentificationDokument5 SeitenAnalyzing Noise Robustness of MFCC and GFCC Features in Speaker Identificationhhakim32Noch keine Bewertungen
- 17 BSC Hons Quantity Surveying and Commercial ManagementDokument17 Seiten17 BSC Hons Quantity Surveying and Commercial ManagementKrish DoodnauthNoch keine Bewertungen
- Job Evaluation GuidelineDokument47 SeitenJob Evaluation GuidelineandrewlkpNoch keine Bewertungen
- Evaluate The Importance Question (12 Marks)Dokument1 SeiteEvaluate The Importance Question (12 Marks)Natalia100% (1)
- Streaming Real-Time Market DataDokument5 SeitenStreaming Real-Time Market DataMoly SenguptaNoch keine Bewertungen
- Academic Self Efficacy in Bachelor Level Nursing Students: Development and Validation of A New InstrumentDokument11 SeitenAcademic Self Efficacy in Bachelor Level Nursing Students: Development and Validation of A New InstrumentOlga Penaten DemonNoch keine Bewertungen
- AI & ChatGPTDokument64 SeitenAI & ChatGPTSergio Ocando (SEOM90)Noch keine Bewertungen
- Literature Review Institutional TheoryDokument8 SeitenLiterature Review Institutional Theorylixdpuvkg100% (1)
- Strategic Management All ChsDokument94 SeitenStrategic Management All ChsBona IbrahimNoch keine Bewertungen
- Chest PainDokument10 SeitenChest PainYeri HoloNoch keine Bewertungen
- Chapter 5Dokument40 SeitenChapter 5Ebisa ChemedaNoch keine Bewertungen
- 0 ListaDokument31 Seiten0 ListaRicardo CostaNoch keine Bewertungen
- Chief Education Supervisor & Education ProgramDokument27 SeitenChief Education Supervisor & Education ProgramIvy Joy TorresNoch keine Bewertungen
- Probability - Homework Week 2Dokument8 SeitenProbability - Homework Week 2uses privateNoch keine Bewertungen
- Contingency Reserve VS Management Reserve - PM VidyaDokument1 SeiteContingency Reserve VS Management Reserve - PM VidyaYousef ANoch keine Bewertungen
- Cambridge International ExaminationsDokument12 SeitenCambridge International ExaminationsNgợm NghịchNoch keine Bewertungen
- BigDataforDevelopment UNGlobalPulseJune2012Dokument47 SeitenBigDataforDevelopment UNGlobalPulseJune2012Ana Caroline Sanchez SilvaNoch keine Bewertungen
- Lab and Project Work Sum 19Dokument50 SeitenLab and Project Work Sum 19Aabid RashidNoch keine Bewertungen