Das könnte Ihnen auch gefallen
- 6-7 Trigger Point and ApplicationDokument16 Seiten6-7 Trigger Point and ApplicationDaniel WilsonNoch keine Bewertungen
- Business TargetsDokument5 SeitenBusiness TargetsDaniel WilsonNoch keine Bewertungen
- LeaseAgreementDWSI - Tenant Highlighted.1Dokument2 SeitenLeaseAgreementDWSI - Tenant Highlighted.1Daniel WilsonNoch keine Bewertungen
- RBS Business PlanDokument9 SeitenRBS Business PlanDaniel WilsonNoch keine Bewertungen
- DWSIM Case HistoryDokument8 SeitenDWSIM Case HistoryDaniel WilsonNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Role of Dispensers in The Rational Use of DrugsDokument19 SeitenThe Role of Dispensers in The Rational Use of DrugsAci LusianaNoch keine Bewertungen
- Case Study SLDokument5 SeitenCase Study SLCharmie Mei Paredes-RoqueNoch keine Bewertungen
- History Taking GuideDokument2 SeitenHistory Taking GuideKristel Anne G. CatabayNoch keine Bewertungen
- Treating Paranoid OrganizationDokument6 SeitenTreating Paranoid Organizationredpsych103100% (2)
- Patient care and discharge planDokument2 SeitenPatient care and discharge planBryan Carmona100% (1)
- The Apgar ScoreDokument6 SeitenThe Apgar ScoretiuwangNoch keine Bewertungen
- NCP: Labor Stage 1 Latent PhaseDokument9 SeitenNCP: Labor Stage 1 Latent PhaseJavieNoch keine Bewertungen
- Canadian Framework For Teamwork and Communications Lit ReviewDokument68 SeitenCanadian Framework For Teamwork and Communications Lit ReviewanxxxanaNoch keine Bewertungen
- Stress: Dr. Jayesh PatidarDokument56 SeitenStress: Dr. Jayesh PatidarDr. Jayesh Patidar100% (2)
- Ursing Standards: Intrdocution:-Standard Is An Acknowledged Measure of Comparison For Quantitative or QualitativeDokument13 SeitenUrsing Standards: Intrdocution:-Standard Is An Acknowledged Measure of Comparison For Quantitative or QualitativemalathiNoch keine Bewertungen
- Family and Pediatric Dentistry Business PlanDokument27 SeitenFamily and Pediatric Dentistry Business PlanSiti Latifah Maharani100% (1)
- Dall Miles Surgical ProtocolDokument16 SeitenDall Miles Surgical Protocolfarnaz_2647334Noch keine Bewertungen
- Open Structure Rhinoplasty For Management of The Non-Caucasian NoseDokument9 SeitenOpen Structure Rhinoplasty For Management of The Non-Caucasian NoseJose ManuelNoch keine Bewertungen
- Glasgow Coma ScaleDokument3 SeitenGlasgow Coma Scalerenell83181Noch keine Bewertungen
- Osteosarcoma DR: Gehan MohamedDokument19 SeitenOsteosarcoma DR: Gehan MohamedNico DougaNoch keine Bewertungen
- Coxa PlanaDokument8 SeitenCoxa PlanaLorebell100% (2)
- Perloff TOFDokument28 SeitenPerloff TOFvamshidhNoch keine Bewertungen
- Epilepsy PresentationDokument10 SeitenEpilepsy Presentationapi-346838508Noch keine Bewertungen
- Pancreas Functions and DiseasesDokument18 SeitenPancreas Functions and DiseasesLisa PalabaoNoch keine Bewertungen
- Recommendation Letter - SheriDokument1 SeiteRecommendation Letter - Sheriapi-355180754100% (1)
- Aprilia Putri Rahmadini, M.Psi ., PsikologDokument12 SeitenAprilia Putri Rahmadini, M.Psi ., PsikologReffa Rizkyani IrawanNoch keine Bewertungen
- HEYER VizOR 6 - Manual 1.0 EN PDFDokument128 SeitenHEYER VizOR 6 - Manual 1.0 EN PDFkalandorka92Noch keine Bewertungen
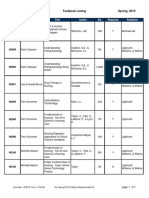
- BFLSON Course Textbook ListingDokument7 SeitenBFLSON Course Textbook ListingWina ViqaNoch keine Bewertungen
- Wit - A Film Review, Analysis and Interview With Playwright Margaret EdsonDokument9 SeitenWit - A Film Review, Analysis and Interview With Playwright Margaret EdsonamelamerNoch keine Bewertungen
- Poster Mini MiliariaDokument25 SeitenPoster Mini MiliariafillygogoNoch keine Bewertungen
- Coital Injuries of the VaginaDokument4 SeitenCoital Injuries of the VaginaFitri Nur DiniNoch keine Bewertungen
- Non Surgical Management of Periapical Lesions Using Calcium HydroxideDokument6 SeitenNon Surgical Management of Periapical Lesions Using Calcium HydroxideVinisha Vipin SharmaNoch keine Bewertungen
- Assessing Pulse Oximetry (Performance Checklist) : Iloilo Doctors' College College of NursingDokument1 SeiteAssessing Pulse Oximetry (Performance Checklist) : Iloilo Doctors' College College of NursingJemy Tamaño MorongNoch keine Bewertungen
- Infectious Diseases - Infective EndocarditisDokument41 SeitenInfectious Diseases - Infective Endocarditisfire_n_iceNoch keine Bewertungen
- Anaesthetic Drug Crib Sheet-8 PDFDokument1 SeiteAnaesthetic Drug Crib Sheet-8 PDFLiam O'ConnorNoch keine Bewertungen