Das könnte Ihnen auch gefallen
- Apriso Savings Card: Bin: Group: ID: ExpirationDokument1 SeiteApriso Savings Card: Bin: Group: ID: ExpirationuserillusionNoch keine Bewertungen
- SingulairDokument1 SeiteSingulairNava GrahazNoch keine Bewertungen
- Mosquito Repellent Is Available As A Statewide Benefit: Covered ProgramsDokument5 SeitenMosquito Repellent Is Available As A Statewide Benefit: Covered ProgramsJuanNoch keine Bewertungen
- BRILINTA CAD $5 No FTO PDFDokument1 SeiteBRILINTA CAD $5 No FTO PDFperaNoch keine Bewertungen
- Lantus Co-Pay Savings CardDokument1 SeiteLantus Co-Pay Savings CardAnthony Mckenzie0% (1)
- Prescription Reimb Claim FormDokument2 SeitenPrescription Reimb Claim FormimthedciNoch keine Bewertungen
- Relistor Savings Card: 0 CopayDokument1 SeiteRelistor Savings Card: 0 CopayJulieann RodgersNoch keine Bewertungen
- LinzessSavingCardPDF 2Dokument1 SeiteLinzessSavingCardPDF 2tqzj54jmxnNoch keine Bewertungen
- Galderma Pharmaceutical BrochureDokument1 SeiteGalderma Pharmaceutical BrochureJamesNoch keine Bewertungen
- GL3655EDokument0 SeitenGL3655EandyhrNoch keine Bewertungen
- Schedule A Vaccination Appointment Walgreens Immunization Services ConfirmationAppt PageDokument1 SeiteSchedule A Vaccination Appointment Walgreens Immunization Services ConfirmationAppt Pagexerona83Noch keine Bewertungen
- Pparx ApplicationsDokument8 SeitenPparx ApplicationsJames MullinsNoch keine Bewertungen
- KombiglyzeXR Savings CardDokument1 SeiteKombiglyzeXR Savings CardRodolfo ArangoNoch keine Bewertungen
- Zer - Pay: Every Fill. Every MonthDokument1 SeiteZer - Pay: Every Fill. Every MonthrebecaNoch keine Bewertungen
- Pay As Little As: Savings ProgramDokument1 SeitePay As Little As: Savings ProgramelasticemperorNoch keine Bewertungen
- Savings CardDokument1 SeiteSavings CardAvinash MalladhiNoch keine Bewertungen
- HeathGuard BrochureDokument2 SeitenHeathGuard BrochureKumud GandhiNoch keine Bewertungen
- 2023 - Oe - Notice - 2008 - FinalDokument5 Seiten2023 - Oe - Notice - 2008 - FinalabroughearNoch keine Bewertungen
- Galderma Care CardDokument2 SeitenGalderma Care CardKlaudia WojtynskaNoch keine Bewertungen
- EligibilityResultsNotice PDFDokument10 SeitenEligibilityResultsNotice PDFtoluNoch keine Bewertungen
- Eligibility NoticeDokument17 SeitenEligibility NoticeFlintston3Noch keine Bewertungen
- Eligibility Results NoticeDokument12 SeitenEligibility Results NoticeDesign to BlessNoch keine Bewertungen
- Abbott Diabetes Care (PDF Library)Dokument2 SeitenAbbott Diabetes Care (PDF Library)RINA.Noch keine Bewertungen
- Patient Assistance Program: How To ApplyDokument3 SeitenPatient Assistance Program: How To ApplyDavid NowakowskiNoch keine Bewertungen
- Health Insurance FAQ From IntrawestDokument9 SeitenHealth Insurance FAQ From IntrawestScott FranzNoch keine Bewertungen
- Insurance Manual PDFDokument56 SeitenInsurance Manual PDFesesmith108Noch keine Bewertungen
- EligibilityResultsNotice 2Dokument12 SeitenEligibilityResultsNotice 2Shannon GambleNoch keine Bewertungen
- Ihc Hmo Coin Value Hmo 405 PlatinumDokument12 SeitenIhc Hmo Coin Value Hmo 405 PlatinumJennifer WrightNoch keine Bewertungen
- Eligibility Results NoticeDokument12 SeitenEligibility Results NoticeNinaPintaSantaMariaNoch keine Bewertungen
- Eligibility Results NoticeDokument12 SeitenEligibility Results NoticePhilip ChastaingNoch keine Bewertungen
- Pharmacy Update: Health Net Medi-Cal Claims Processing Migrates From Medimpact To Cvs Caremark Effective November 1Dokument2 SeitenPharmacy Update: Health Net Medi-Cal Claims Processing Migrates From Medimpact To Cvs Caremark Effective November 1Saul RuizNoch keine Bewertungen
- Summary of Benefits: For Bcbsga Mediblue Access (Ppo)Dokument44 SeitenSummary of Benefits: For Bcbsga Mediblue Access (Ppo)J MillerNoch keine Bewertungen
- VANIQA Coupon PDFDokument1 SeiteVANIQA Coupon PDFChristopher BrownNoch keine Bewertungen
- Your Eligibility Results: Family Member(s) Results Next StepsDokument10 SeitenYour Eligibility Results: Family Member(s) Results Next StepsAdam DonéNoch keine Bewertungen
- COVID-19 and Flu Vaccination Walgreens ImmunizaDokument1 SeiteCOVID-19 and Flu Vaccination Walgreens ImmunizakittenrollNoch keine Bewertungen
- Eligibility Results NoticeDokument12 SeitenEligibility Results NoticefullmetalrebelNoch keine Bewertungen
- A Better Medicare. A Better You: MD Medicarechoice, IncDokument19 SeitenA Better Medicare. A Better You: MD Medicarechoice, Inclancastd54Noch keine Bewertungen
- 3CCO OHP Drug Formulary FinalWebDokument124 Seiten3CCO OHP Drug Formulary FinalWebKandraNoch keine Bewertungen
- Formulary - Good ReadDokument121 SeitenFormulary - Good ReadJananiRajamanickamNoch keine Bewertungen
- Morningstar India Private Limited: Hospitalization Benefit PlanDokument10 SeitenMorningstar India Private Limited: Hospitalization Benefit PlandevanyaNoch keine Bewertungen
- Med GulfDokument44 SeitenMed GulfAnonymous B7pghhNoch keine Bewertungen
- 2012 Comprehensive Formulary: List of Covered DrugsDokument51 Seiten2012 Comprehensive Formulary: List of Covered DrugsKapilNoch keine Bewertungen
- Selections Membership GuideDokument52 SeitenSelections Membership GuideNader AdelNoch keine Bewertungen
- Your Eligibility Results: Department of Health and Human Services 465 Industrial Boulevard London, Kentucky 40750-0001Dokument16 SeitenYour Eligibility Results: Department of Health and Human Services 465 Industrial Boulevard London, Kentucky 40750-0001John SpiersNoch keine Bewertungen
- ComprKaiehensive FormularyDokument77 SeitenComprKaiehensive Formularypeter_rabbitNoch keine Bewertungen
- Health Insurance Spring 2017Dokument2 SeitenHealth Insurance Spring 2017Manideep RemalaNoch keine Bewertungen
- Here's A CONCERTA Savings Program CardDokument1 SeiteHere's A CONCERTA Savings Program CardSpencer JacksonNoch keine Bewertungen
- Sisc Q ADokument7 SeitenSisc Q Aapi-204910805Noch keine Bewertungen
- Bupa Gold Membership GuideDokument14 SeitenBupa Gold Membership GuidebupavietnamNoch keine Bewertungen
- Prescription Assistance Programs: What Resources Are Available To Help Locate An Assistance Program For My Medications?Dokument1 SeitePrescription Assistance Programs: What Resources Are Available To Help Locate An Assistance Program For My Medications?Sorbito ComettoNoch keine Bewertungen
- 50a580af40315 PDFDokument1 Seite50a580af40315 PDFSorbito ComettoNoch keine Bewertungen
- Eligibility Results NoticeDokument12 SeitenEligibility Results NoticeKehra SongNoch keine Bewertungen
- N202669852876 Template012 131071016 09 22 2020 05 19 17 ENDokument8 SeitenN202669852876 Template012 131071016 09 22 2020 05 19 17 ENmaraki2012Noch keine Bewertungen
- C Is Health Su Raksha Policy WordingDokument16 SeitenC Is Health Su Raksha Policy Wordingsmith willNoch keine Bewertungen
- EligibilityResultsNotice 5Dokument7 SeitenEligibilityResultsNotice 5Larisa AbrahamyanNoch keine Bewertungen
- Eligibility Results NoticeDokument11 SeitenEligibility Results NoticeWilliam PeeleNoch keine Bewertungen
- Assignment of Benefits MedicareDokument6 SeitenAssignment of Benefits Medicarepmojoumpd100% (1)
- Print ApplicationDokument7 SeitenPrint ApplicationHarris HoneycuttNoch keine Bewertungen
- Trigonometric Functions Trigonometric FunctionsDokument18 SeitenTrigonometric Functions Trigonometric FunctionsGisele PhaloNoch keine Bewertungen
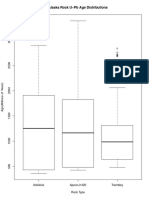
- Trem Probability Distribution PDFDokument1 SeiteTrem Probability Distribution PDFGisele PhaloNoch keine Bewertungen
- Trem Probability DistributionDokument1 SeiteTrem Probability DistributionGisele PhaloNoch keine Bewertungen
- A New Leadership Curriculum: The Multiplication of IntelligenceDokument4 SeitenA New Leadership Curriculum: The Multiplication of IntelligenceGisele PhaloNoch keine Bewertungen
- Trem Frequency Distribution PDFDokument1 SeiteTrem Frequency Distribution PDFGisele PhaloNoch keine Bewertungen
- Rplot03 PDFDokument1 SeiteRplot03 PDFGisele PhaloNoch keine Bewertungen
- BioDokument1 SeiteBioGisele PhaloNoch keine Bewertungen
- Cover Letter GuideDokument10 SeitenCover Letter GuideGisele PhaloNoch keine Bewertungen
- G Major Scale Arpeggio For GuitarDokument1 SeiteG Major Scale Arpeggio For GuitarGisele PhaloNoch keine Bewertungen
- 2016 Dplan WorksheetDokument4 Seiten2016 Dplan WorksheetGisele PhaloNoch keine Bewertungen
- Online Final Exam Spring Part A-ProblemsDokument4 SeitenOnline Final Exam Spring Part A-ProblemsGisele PhaloNoch keine Bewertungen
- Beginning Music Theory-01 (SP14)Dokument2 SeitenBeginning Music Theory-01 (SP14)Gisele PhaloNoch keine Bewertungen
- Physics Test Review QuestionsDokument1 SeitePhysics Test Review QuestionsGisele PhaloNoch keine Bewertungen
- Latin America ReviewDokument4 SeitenLatin America ReviewGisele PhaloNoch keine Bewertungen
- Vocab 7Dokument4 SeitenVocab 7Gisele PhaloNoch keine Bewertungen
- AP Spanish Literature - Ms - LizarragaDokument8 SeitenAP Spanish Literature - Ms - LizarragaGisele Phalo50% (2)
- Drug Stores Top 100 VT - JustdialDokument6 SeitenDrug Stores Top 100 VT - JustdialTal subuNoch keine Bewertungen
- GDT 2 115Dokument3 SeitenGDT 2 115Isti IzzuddinNoch keine Bewertungen
- PharmacotherapyDokument15 SeitenPharmacotherapyPrincess RonsableNoch keine Bewertungen
- SB 154Dokument14 SeitenSB 154Phillip StuckyNoch keine Bewertungen
- Final FMOH National Guideline For Compounding of DermatologicalDokument143 SeitenFinal FMOH National Guideline For Compounding of DermatologicalKumera Dinkisa ToleraNoch keine Bewertungen
- Book 15 Homework & EEDokument62 SeitenBook 15 Homework & EEgamblerNoch keine Bewertungen
- Scope of Clinical PharmacyDokument13 SeitenScope of Clinical PharmacykeerthanaNoch keine Bewertungen
- Expanded Scope Orientation ManualDokument47 SeitenExpanded Scope Orientation ManualEmad MerganNoch keine Bewertungen
- Final Report For Colorado Public Option - Includes Appendices I - IVDokument101 SeitenFinal Report For Colorado Public Option - Includes Appendices I - IVapi-491077033Noch keine Bewertungen
- 36 Medical Useand MisuseDokument9 Seiten36 Medical Useand MisuseAlfredo MorenoNoch keine Bewertungen
- Data Warehousing and Mining CourseworkDokument19 SeitenData Warehousing and Mining CourseworkVal0% (1)
- Diploma in Pharmac1Dokument22 SeitenDiploma in Pharmac1Sharmila LamisharNoch keine Bewertungen
- Application Letter (Pharma)Dokument1 SeiteApplication Letter (Pharma)rinkashime jikitaNoch keine Bewertungen
- PT - Mapeh 6 - Q4 - V2Dokument6 SeitenPT - Mapeh 6 - Q4 - V2MarlynSanchezTenorioNoch keine Bewertungen
- Sample Questions PEBC ExamDokument2 SeitenSample Questions PEBC ExamReem HassanNoch keine Bewertungen
- Registration of Veterinary Drug and ProductDokument2 SeitenRegistration of Veterinary Drug and ProductLeogarda NudoNoch keine Bewertungen
- Drugs Standard Rules 2041 - NepalDokument38 SeitenDrugs Standard Rules 2041 - NepalAbhishek Man ShresthaNoch keine Bewertungen
- Case Study PRE-SEEN MAY 2021.editedDokument14 SeitenCase Study PRE-SEEN MAY 2021.editedDAVID OWUSUNoch keine Bewertungen
- Infected Blanket Policies:: Joan Jack, B.Ed, LLB, #OjibwaywarriormomDokument17 SeitenInfected Blanket Policies:: Joan Jack, B.Ed, LLB, #OjibwaywarriormomJoan JackNoch keine Bewertungen
- Polytechnic University of The PhilippinesDokument20 SeitenPolytechnic University of The PhilippinesdaniellaNoch keine Bewertungen
- Importance of Consumer HealthDokument22 SeitenImportance of Consumer HealthTeacher BhingNoch keine Bewertungen
- Group BaafogDokument9 SeitenGroup Baafogakinrotimi omotayoNoch keine Bewertungen
- Hospital Pharmacy PracticeDokument14 SeitenHospital Pharmacy PracticeGerald GamboaNoch keine Bewertungen
- Opioid Analgesics: Symposium On Pain MedicineDokument12 SeitenOpioid Analgesics: Symposium On Pain Medicineyunica simanjuntakNoch keine Bewertungen
- Clinical PharmacyDokument7 SeitenClinical PharmacyKabir ManchandaNoch keine Bewertungen
- Aproved Drug Products Suplements 2013Dokument136 SeitenAproved Drug Products Suplements 2013renshagullNoch keine Bewertungen
- NJ Mpje PDFDokument168 SeitenNJ Mpje PDFPatrick Mata100% (3)
- DR Narendra Kumar Assistant ProfessorDokument16 SeitenDR Narendra Kumar Assistant ProfessorAbdiweli AbubakarNoch keine Bewertungen
- Sweta Agarwal-EPGP-13A-114: Major Target Segmentation Can Be Done On Below BasisDokument3 SeitenSweta Agarwal-EPGP-13A-114: Major Target Segmentation Can Be Done On Below BasisSweta AgarwalNoch keine Bewertungen
- English Researh Paper1Dokument7 SeitenEnglish Researh Paper1monigiraldoNoch keine Bewertungen
- The Power of Our Supreme Court: How Supreme Court Cases Shape DemocracyVon EverandThe Power of Our Supreme Court: How Supreme Court Cases Shape DemocracyBewertung: 5 von 5 Sternen5/5 (2)
- Legal Writing in Plain English: A Text with ExercisesVon EverandLegal Writing in Plain English: A Text with ExercisesBewertung: 3 von 5 Sternen3/5 (2)
- Employment Law: a Quickstudy Digital Law ReferenceVon EverandEmployment Law: a Quickstudy Digital Law ReferenceBewertung: 1 von 5 Sternen1/5 (1)
- Dictionary of Legal Terms: Definitions and Explanations for Non-LawyersVon EverandDictionary of Legal Terms: Definitions and Explanations for Non-LawyersBewertung: 5 von 5 Sternen5/5 (2)
- Legal Research: a QuickStudy Laminated Law ReferenceVon EverandLegal Research: a QuickStudy Laminated Law ReferenceNoch keine Bewertungen
- Nolo's Deposition Handbook: The Essential Guide for Anyone Facing or Conducting a DepositionVon EverandNolo's Deposition Handbook: The Essential Guide for Anyone Facing or Conducting a DepositionBewertung: 5 von 5 Sternen5/5 (1)
- Legal Guide for Starting & Running a Small BusinessVon EverandLegal Guide for Starting & Running a Small BusinessBewertung: 4.5 von 5 Sternen4.5/5 (9)
- Legal Forms for Starting & Running a Small Business: 65 Essential Agreements, Contracts, Leases & LettersVon EverandLegal Forms for Starting & Running a Small Business: 65 Essential Agreements, Contracts, Leases & LettersNoch keine Bewertungen
- Legal Writing in Plain English, Third Edition: A Text with ExercisesVon EverandLegal Writing in Plain English, Third Edition: A Text with ExercisesNoch keine Bewertungen
- How to Make Patent Drawings: Save Thousands of Dollars and Do It With a Camera and Computer!Von EverandHow to Make Patent Drawings: Save Thousands of Dollars and Do It With a Camera and Computer!Bewertung: 5 von 5 Sternen5/5 (1)
- Flora and Vegetation of Bali Indonesia: An Illustrated Field GuideVon EverandFlora and Vegetation of Bali Indonesia: An Illustrated Field GuideBewertung: 5 von 5 Sternen5/5 (2)
- Torts: QuickStudy Laminated Reference GuideVon EverandTorts: QuickStudy Laminated Reference GuideBewertung: 5 von 5 Sternen5/5 (1)
- So You Want to be a Lawyer: The Ultimate Guide to Getting into and Succeeding in Law SchoolVon EverandSo You Want to be a Lawyer: The Ultimate Guide to Getting into and Succeeding in Law SchoolNoch keine Bewertungen
- LLC or Corporation?: Choose the Right Form for Your BusinessVon EverandLLC or Corporation?: Choose the Right Form for Your BusinessBewertung: 3.5 von 5 Sternen3.5/5 (4)
- Nolo's Essential Guide to Buying Your First HomeVon EverandNolo's Essential Guide to Buying Your First HomeBewertung: 4 von 5 Sternen4/5 (43)
- Essential Guide to Workplace Investigations, The: A Step-By-Step Guide to Handling Employee Complaints & ProblemsVon EverandEssential Guide to Workplace Investigations, The: A Step-By-Step Guide to Handling Employee Complaints & ProblemsBewertung: 3 von 5 Sternen3/5 (2)
- Nolo's Encyclopedia of Everyday Law: Answers to Your Most Frequently Asked Legal QuestionsVon EverandNolo's Encyclopedia of Everyday Law: Answers to Your Most Frequently Asked Legal QuestionsBewertung: 4 von 5 Sternen4/5 (18)