Das könnte Ihnen auch gefallen
- The Chinese Version of The World Health Organization Quality of Life Instrument-Older Adults Module (WHOQOL-OLD) : Psychometric EvaluationDokument8 SeitenThe Chinese Version of The World Health Organization Quality of Life Instrument-Older Adults Module (WHOQOL-OLD) : Psychometric EvaluationSyed ShahNoch keine Bewertungen
- Behavioral Economics and The Promotion of Health Among Aging PopulationsDokument12 SeitenBehavioral Economics and The Promotion of Health Among Aging PopulationsGonzalo PachecoNoch keine Bewertungen
- TehCH - Physical Activity 2011 PDFDokument9 SeitenTehCH - Physical Activity 2011 PDFesan samaNoch keine Bewertungen
- Disability, Frailty and Depression in The Community-Dwelling Older Adults With OsteosarcopeniaDokument7 SeitenDisability, Frailty and Depression in The Community-Dwelling Older Adults With OsteosarcopeniaKhairunnisa Ayu KresnandaNoch keine Bewertungen
- Identifying A Cut-Off Point For Normal Mobility: A Comparison of The Timed Up and Go' Test in Community-Dwelling and Institutionalised Elderly WomenDokument6 SeitenIdentifying A Cut-Off Point For Normal Mobility: A Comparison of The Timed Up and Go' Test in Community-Dwelling and Institutionalised Elderly WomenCarolina SandovalNoch keine Bewertungen
- Effects of The Training Given To Older Adults On Urinary IncontinenceDokument13 SeitenEffects of The Training Given To Older Adults On Urinary IncontinenceJesusNavarrete97Noch keine Bewertungen
- Using Formative Research With Older Adults To InfoDokument10 SeitenUsing Formative Research With Older Adults To InfoYameen JanNoch keine Bewertungen
- Gerontology Individual Assignment 1Dokument14 SeitenGerontology Individual Assignment 1Innocent T SumburetaNoch keine Bewertungen
- RRL LocalinternationalDokument11 SeitenRRL LocalinternationalkdfhjfhfNoch keine Bewertungen
- Lifestyle Management Practice of 40 - 59 Years Cohort in Hong KongDokument9 SeitenLifestyle Management Practice of 40 - 59 Years Cohort in Hong KongSaudah Sii SipitNoch keine Bewertungen
- 2 Prevalence of Sarcopenia in Multi EthnicsDokument10 Seiten2 Prevalence of Sarcopenia in Multi EthnicsdavidtuanandartuaNoch keine Bewertungen
- Qi Gong Quality Life in TaiwanDokument6 SeitenQi Gong Quality Life in TaiwanpenfoNoch keine Bewertungen
- Factors Influencing Health Knowledge and Behaviors Among The Elderly in Rural ChinaDokument17 SeitenFactors Influencing Health Knowledge and Behaviors Among The Elderly in Rural ChinaDilaArdaNiNoch keine Bewertungen
- Taking Up Physical Activity in Later Life and Healthy Ageing: The English Longitudinal Study of AgeingDokument6 SeitenTaking Up Physical Activity in Later Life and Healthy Ageing: The English Longitudinal Study of AgeingmartinNoch keine Bewertungen
- Caffeinated Drinks Intake, Late Chronotype, and Increased Body Mass Index Among Medical Students in Chongqing, China: A Multiple Mediation ModelDokument12 SeitenCaffeinated Drinks Intake, Late Chronotype, and Increased Body Mass Index Among Medical Students in Chongqing, China: A Multiple Mediation ModelRhael LopesNoch keine Bewertungen
- Age MenarcheDokument7 SeitenAge MenarchenamiracarolineNoch keine Bewertungen
- A Group of 500 Women Whose Health May Depart Notably From The Norm: Protocol For A Cross-Sectional SurveyDokument12 SeitenA Group of 500 Women Whose Health May Depart Notably From The Norm: Protocol For A Cross-Sectional Surveyhanna.oravecz1Noch keine Bewertungen
- Research ArticleDokument8 SeitenResearch Articlewoldekidansamuel299Noch keine Bewertungen
- Emerging Issues in Geriatric Care: Aging and Public Health PerspectivesDokument6 SeitenEmerging Issues in Geriatric Care: Aging and Public Health PerspectiveslynhareeNoch keine Bewertungen
- Findings From Britain: The Effects Illness Quality of Households in GreatDokument7 SeitenFindings From Britain: The Effects Illness Quality of Households in GreatGunung MahameruNoch keine Bewertungen
- Rajiv Gandhi University of Health Sciences Karnataka, Bangalore Annexure - IDokument11 SeitenRajiv Gandhi University of Health Sciences Karnataka, Bangalore Annexure - IMatthew RiveraNoch keine Bewertungen
- Paradigm of The StudyDokument6 SeitenParadigm of The Studyjervrgbp15Noch keine Bewertungen
- Health Literacy On Hypertension and Functional Health Status Among Elderly of Malabon City, PhilippinesDokument20 SeitenHealth Literacy On Hypertension and Functional Health Status Among Elderly of Malabon City, PhilippinesGlobal Research and Development ServicesNoch keine Bewertungen
- Physical Activity Levels and Health-Related Quality of Life in Young Italian PopulationDokument17 SeitenPhysical Activity Levels and Health-Related Quality of Life in Young Italian PopulationCarlos RodriguezNoch keine Bewertungen
- 3612-Article Text-12854-2-10-20240108Dokument12 Seiten3612-Article Text-12854-2-10-202401084ymwg78wxcNoch keine Bewertungen
- Ijerph 16 02592Dokument14 SeitenIjerph 16 02592KikimariaNoch keine Bewertungen
- Mak, 2018. Estilo de Vida Promotor de La Salud y Calidad de Vida Entre Los Estudiantes de Enfermería ChinosDokument8 SeitenMak, 2018. Estilo de Vida Promotor de La Salud y Calidad de Vida Entre Los Estudiantes de Enfermería ChinosIván Lázaro IllatopaNoch keine Bewertungen
- TaiwanDokument11 SeitenTaiwanbin linNoch keine Bewertungen
- Occupation, Physical Fitness and Adiposity Markers Among Security Guards and Students of Delhi UniversityDokument8 SeitenOccupation, Physical Fitness and Adiposity Markers Among Security Guards and Students of Delhi UniversityPradeepNoch keine Bewertungen
- Da7b 2 PDFDokument10 SeitenDa7b 2 PDFAlyssa Anne GrandaNoch keine Bewertungen
- Polypharmacy Physical and Nutritional Status and Depression in The Elderly Do Polypharmacy Deserve Some Credits in These ProblemsDokument14 SeitenPolypharmacy Physical and Nutritional Status and Depression in The Elderly Do Polypharmacy Deserve Some Credits in These ProblemsiwannasleepeverytimeNoch keine Bewertungen
- The Role of Healthy Lifestyles in Healthy AgingDokument3 SeitenThe Role of Healthy Lifestyles in Healthy AgingDESMOND EZIEKENoch keine Bewertungen
- IJPR.2016.191 Kebugaran Pada LansiaDokument8 SeitenIJPR.2016.191 Kebugaran Pada LansiaMas AbrarNoch keine Bewertungen
- 2020 Article 1986Dokument13 Seiten2020 Article 1986Arierta PujitresnaniNoch keine Bewertungen
- The Relationship Between Periodontal Disease and Public Health: A Population-Based StudyDokument6 SeitenThe Relationship Between Periodontal Disease and Public Health: A Population-Based StudyHtet AungNoch keine Bewertungen
- Paul Willis - Trans AdultsDokument11 SeitenPaul Willis - Trans Adultsมา ยาNoch keine Bewertungen
- Association Between Physical Activity and Menopausal Symptoms in Perimenopausal WomenDokument8 SeitenAssociation Between Physical Activity and Menopausal Symptoms in Perimenopausal WomenAlejandra JinezNoch keine Bewertungen
- Food To Eat and AvoidDokument12 SeitenFood To Eat and Avoidrula alsawalqaNoch keine Bewertungen
- HG - SR.2019.09.01. Trayectorias de Envejecimiento Humano en MéxicoDokument10 SeitenHG - SR.2019.09.01. Trayectorias de Envejecimiento Humano en MéxicoAlejandro GuzmánNoch keine Bewertungen
- Prevalence of Overweight and Obesity and Weight Loss Practice Among Beijing Adults, 2011Dokument10 SeitenPrevalence of Overweight and Obesity and Weight Loss Practice Among Beijing Adults, 2011Aboy GunawanNoch keine Bewertungen
- P122Dokument10 SeitenP122Vicho Neira PinochetNoch keine Bewertungen
- 10 Priya Et AlDokument5 Seiten10 Priya Et AleditorijmrhsNoch keine Bewertungen
- Scientific Research Journal of India SRJI Vol-3 Issue-3 Year 2014Dokument209 SeitenScientific Research Journal of India SRJI Vol-3 Issue-3 Year 2014Dr. Krishna N. SharmaNoch keine Bewertungen
- Literature Review Bariatric SurgeryDokument8 SeitenLiterature Review Bariatric Surgeryaflsigfek100% (1)
- A Study of The Morbidity Pattern Among The Geriatric Population in A Rural Area of West BengalDokument5 SeitenA Study of The Morbidity Pattern Among The Geriatric Population in A Rural Area of West BengalAnirban ChatterjeeNoch keine Bewertungen
- Effectiveness of Tai Chi Exercise On Overall Quality of LifeDokument7 SeitenEffectiveness of Tai Chi Exercise On Overall Quality of LifeAndreRicardoCPNoch keine Bewertungen
- P3 Health StatusDokument9 SeitenP3 Health StatusNovita Mariani GlekoNoch keine Bewertungen
- Ageism, Healthy Life Expectancy and Population Ageing: How Are They Related?Dokument11 SeitenAgeism, Healthy Life Expectancy and Population Ageing: How Are They Related?Betsabé CastroNoch keine Bewertungen
- Final Assessment For Introduction To Research Methods (RMCR3101)Dokument4 SeitenFinal Assessment For Introduction To Research Methods (RMCR3101)Maddah HussainNoch keine Bewertungen
- Rajiv Gandhi University of Health Sciences Bangalore, KarnatakaDokument11 SeitenRajiv Gandhi University of Health Sciences Bangalore, KarnatakaGuna RamyaNoch keine Bewertungen
- Progression and Predictors of Mild Cognitive Impairment in Chinese Elderly: A Prospective Follow-Up in The Shanghai Aging StudyDokument9 SeitenProgression and Predictors of Mild Cognitive Impairment in Chinese Elderly: A Prospective Follow-Up in The Shanghai Aging StudyCristina SavaNoch keine Bewertungen
- Microbiota Adulto MayorDokument18 SeitenMicrobiota Adulto MayorOlga GuerreroNoch keine Bewertungen
- Relationship Between Subjective Well-Being and Healthy Lifestyle Behaviours in Older Adults: A Longitudinal StudyDokument10 SeitenRelationship Between Subjective Well-Being and Healthy Lifestyle Behaviours in Older Adults: A Longitudinal Studysharjeelhyder gopanagNoch keine Bewertungen
- Belsky Daniel Et Al., Quantification of Biological Aging in Young AdultsDokument7 SeitenBelsky Daniel Et Al., Quantification of Biological Aging in Young AdultsAristide de BésureNoch keine Bewertungen
- NRP 6 551Dokument8 SeitenNRP 6 551Faqhrul AqimNoch keine Bewertungen
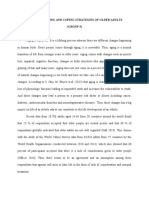
- Effects of Aging and Coping Strategies of Older Adults (GROUP 3)Dokument16 SeitenEffects of Aging and Coping Strategies of Older Adults (GROUP 3)Michael AmandyNoch keine Bewertungen
- Physical Activity, Physical Condition and Quality of Life in OlderDokument9 SeitenPhysical Activity, Physical Condition and Quality of Life in OlderAndré PeriquitoNoch keine Bewertungen
- Introduction to Public Health in ChinaVon EverandIntroduction to Public Health in ChinaLiming LiNoch keine Bewertungen
- Ethics, Qualitative And Quantitative Methods In Public Health ResearchVon EverandEthics, Qualitative And Quantitative Methods In Public Health ResearchNoch keine Bewertungen
- NLP Project ReportDokument27 SeitenNLP Project ReportNitin kumar singhNoch keine Bewertungen
- 21675-Article Text-25688-1-2-20220628Dokument2 Seiten21675-Article Text-25688-1-2-20220628hzauccgNoch keine Bewertungen
- Kenny-230718-Top 70 Microsoft Data Science Interview QuestionsDokument17 SeitenKenny-230718-Top 70 Microsoft Data Science Interview QuestionsvanjchaoNoch keine Bewertungen
- Biomedical Signal Processing and Control: Jibin Wang, Ping Wang, Suping WangDokument10 SeitenBiomedical Signal Processing and Control: Jibin Wang, Ping Wang, Suping WangLaura CursaruNoch keine Bewertungen
- Answers For Mastering Data Analysis in ExcelDokument3 SeitenAnswers For Mastering Data Analysis in ExcelWathek Al Zuaiby67% (6)
- FOUR - Peds Manuscript REV Oct 21Dokument24 SeitenFOUR - Peds Manuscript REV Oct 21Riandini Pramudita RNoch keine Bewertungen
- Elshoush 2019Dokument6 SeitenElshoush 2019bekNoch keine Bewertungen
- Engineering Geology: Hyuck Jin Park, Jung Hyun Lee, Ik WooDokument15 SeitenEngineering Geology: Hyuck Jin Park, Jung Hyun Lee, Ik WooPatricio Saldaña MirandaNoch keine Bewertungen
- Machine Learning Extended ProjectDokument3 SeitenMachine Learning Extended ProjectKrishnameera pythonNoch keine Bewertungen
- NARF 3D Range Image Features For Object RecognitioDokument3 SeitenNARF 3D Range Image Features For Object RecognitioIvan VidovićNoch keine Bewertungen
- FRA AssignmentDokument31 SeitenFRA AssignmentPranav ViswanathanNoch keine Bewertungen
- Beta Angle 2003Dokument6 SeitenBeta Angle 2003surendra334Noch keine Bewertungen
- Federal Law Enforcement Use of Facial Recognition TechnologyDokument24 SeitenFederal Law Enforcement Use of Facial Recognition TechnologyUday BhatnagarNoch keine Bewertungen
- Diagnosis of Malaria Using Double Hidden Layer Extreme Learning Machine Algorithm With CNN Feature Extraction and Parasite InflatorDokument14 SeitenDiagnosis of Malaria Using Double Hidden Layer Extreme Learning Machine Algorithm With CNN Feature Extraction and Parasite InflatorMd NahiduzzamanNoch keine Bewertungen
- Machine Learning Project: Problem 1Dokument26 SeitenMachine Learning Project: Problem 1manas vikram50% (2)
- 25 Years of The Taffler Z-Score Model DoeDokument44 Seiten25 Years of The Taffler Z-Score Model DoeGaMer LoidNoch keine Bewertungen
- Probabilistic Models For ClassificationDokument32 SeitenProbabilistic Models For ClassificationSweta PatilNoch keine Bewertungen
- Popdx: An Automated Framework For Patient Phenotyping Across 392 246 Individuals in The Uk Biobank StudyDokument11 SeitenPopdx: An Automated Framework For Patient Phenotyping Across 392 246 Individuals in The Uk Biobank StudysubaNoch keine Bewertungen
- s40479 023 00233 0Dokument9 Seitens40479 023 00233 0nurazizahsn11Noch keine Bewertungen
- Name:Fedrick Samuel W Reg No: 19MIS1112 Course: Machine Learning (SWE4012) Slot: L11 + L12 Faculty: Dr.M. PremalathaDokument30 SeitenName:Fedrick Samuel W Reg No: 19MIS1112 Course: Machine Learning (SWE4012) Slot: L11 + L12 Faculty: Dr.M. PremalathaFèdríck SämùélNoch keine Bewertungen
- Bayer's in Silico ADMET Platform - Journey of Machine LearningDokument8 SeitenBayer's in Silico ADMET Platform - Journey of Machine LearningYOUTEACHNoch keine Bewertungen
- Predicting & Optimizing Airlines Customer Satisfaction Using ClasDokument84 SeitenPredicting & Optimizing Airlines Customer Satisfaction Using Clas263sailajacgpNoch keine Bewertungen
- FULLTEXT01Dokument99 SeitenFULLTEXT01Velu ManiNoch keine Bewertungen
- 3.stroke Prediction Using Smote-Tomek and Neural NetworkDokument5 Seiten3.stroke Prediction Using Smote-Tomek and Neural NetworkgeethaNoch keine Bewertungen
- Abstracts 8th Congress CSMBLM Rijeka Korekcija N.nikolac 5.11.2015. BO2Dokument101 SeitenAbstracts 8th Congress CSMBLM Rijeka Korekcija N.nikolac 5.11.2015. BO2BoyITBNoch keine Bewertungen
- Unit 3 (ML)Dokument26 SeitenUnit 3 (ML)BHAVIN THUMARNoch keine Bewertungen
- Cyber Threat Intelligence Mining For Proactive Cybersecurity Defense: A Survey and New PerspectivesDokument27 SeitenCyber Threat Intelligence Mining For Proactive Cybersecurity Defense: A Survey and New Perspectivesímélcím tökrandomNoch keine Bewertungen
- 12-4 - ActDokument110 Seiten12-4 - ActTawfeeq AuqbiNoch keine Bewertungen
- Autoph4: An Automated Method For Generating Pharmacophore Models From Protein Binding Pockets Supporting InformationDokument37 SeitenAutoph4: An Automated Method For Generating Pharmacophore Models From Protein Binding Pockets Supporting InformationAngelCo PetsNoch keine Bewertungen
- Behavioral Attributes and Financial Churn Prediction: Regulararticle Open AccessDokument18 SeitenBehavioral Attributes and Financial Churn Prediction: Regulararticle Open AccessHakanNoch keine Bewertungen