American Journal of Engineering Research (AJER)
2016
American Journal of Engineering Research (AJER)
e-ISSN: 2320-0847 p-ISSN : 2320-0936
Volume-5, Issue-6, pp-285-292
www.ajer.org
Research Paper
Open Access
A Constraint-Based Access Control Model for Information Distribution in
Nigerias Healthcare Systems
1
Sarumi Jerry and 2Prof.Adekunle Yinka
Department of Computer Science, Lagos State Polytechnic, Ikorodu, Lagos State.
Department of Computer Science, Babcock University, Ilishan-Remo, Ogun State
ABSTRACT : Sharing clinical data within the domain of Nigerias healthcare system through an Information Technology
central platform appears to be a major challenge, perhaps due to low technological development of the country. This
deficiency constantly exposes the supposedly private data of patients to the wrong hands through the current hand-to-hand
transfer of such data within the healthcare domain. The manual transfer, as observed is appalling; and has subjected the
healthcare information distribution system to breaches of security, delivery, confidentiality and ethical risk issues. This
research addresses these deficiency with a unique contribution to already existing electronic NHMS record keeping systems
by designing and developing a framework with a proof of concept for centralization of patient clinical data for Nigeria
healthcare delivery. It provides an electronic hand-shake using an access control model that can store clinical data of all
patients and share the same data among the concerned healthcare professionals in the healthcare domain. The specific
objectives of this research are to develop a constraint based framework for access control in an information distribution
system that will generate a pattern of misuse and also provide a central information platform for the control of access
related activities. The distributed system is a cloud server where information of the patients are stored and can be easily
accessible by the NHMS personnel or doctors remotely. Achieving this objective compels the study to adopt authentication
and authorization method at inter / intra organizational level for the security and delivery of patients clinical data. The use
of role based access control tools were used to regulate individual access rights to the network resources based on security
policies and rules defined in the program. The developing platform is Windows OS and the web server is Apache. The
system was designed to securely manage and coordinate patients clinical profiles, dynamically identify levels of data to be
accessed, grant authorized access to clinicians/doctors, and privileges to online information transfer / delivery. In order to
access a resource, users must meet the regulatory conditions of the policy class which is in conformity with organizational
standards as stipulated by the Federal Ministry of Health in Nigeria that regularize healthcare policies. The system was
designed to be flexible and adaptive in order to allow users pass on their rights of access to other users, permission given
for right of access can be withdrawn based on the stipulated restrictions that have been defined in the program. The
research is a novel model that is in compliance with healthcare standards in relation to data and service user-friendliness.
The designed framework facilitates flexibility to any deployed environment.
Keywords: Accessibility, access control, electronic hand shake, authentication, authorization, confidentiality and cloud
server.
I.
INTRODUCTION
Health care accessibility has been identified as one of the major indicators of development in Nigeria Health care system.
The importance of the availability of adequate health care facilities in providing sustainable development can therefore not
be over-emphasized. Contrary to some opinions, it has been agreed that lack of basic health care facilities have led to
inefficiency in production, declining productivity, reduced life expectance and increased infant mortality rate. The health
care industry in Nigeria is presently still growing unlike what is obtained in developed countries in Europe and America.
This reported growth (high death rate, increased mortality rate and reduce life span) is obvious in the unavailability of good
health care facilities in Nigeria and the health care system is insufficient when available because of lack of accessibility to
facility (Perry,2000) and (Olutola et al, 2009)
Therefore, this thesis presents an Information Distribution for NationalHealthcare Management Scheme (NHMS) that uses a
web-based spatial approach, authentication and authorization method and role based access control tools to regulate
individual access rights to the network resources to aid the distribution of health care facilities in Nigeria. This system is
expected to assist doctors and clinicians in identifying patients profiles and medical status. It is also expected to provide
support with respect to rightly locating health care facilities at real time; especially to areas where serious attention is
inevitable. With this system, patients, doctors, cliniciansand stakeholders would be able to visualize the distribution of
hospitals in Nigeria. Government would therefore benefit since the system would assist her in communicating effectively to
the general public concerning the demand for more health care facilities.
II. REVIEW OF RELATED WORKS
Chandramouli, (2001) recognizes the emergency access requirement and proposes a logic driven role based dynamic model
supporting context constraints. He introduces a concept called `domain' to group objects. The researcher uses emergency and
logic driven concept as a tool to group related data but the information cannot be access remotely. This new concept of
www.ajer.org
Page 285
American Journal Of Engineering Research (AJER)
2016
context based approach will enable us group objects in cloud server instead of the domain as expressed by Chandramouli,
(2001). Hence, the information can be secured and easily accessible from any network resources remotely.
Verhanneman, (2003) supports practice of fine-grained and dynamic policies in the healthcare domain. They focus on a
reconfigurable implementation and identify a number of shortcomings of current technologies for aiding their
implementation. Standard data representation formatsand ontologies are used to make the model compatible with different
health care systems but in this newly developed system, a client server approach was used. The doctors, patient and
clinicians are the client while the admin is the server. The two tears will be integrated together with the concept of
middleware technology; hence, this enable a health policy compliances between the two tiers.
Blobel, (2004) Information technology is expected to become an essential tool in providing reliable information for
supporting the delivery of health care services. Nevertheless, incorporating such technologies to support the provision of
health care raises concerns over the protection of patients information. The technological, social and legal implications
regarding the access and release of medical data have to be considered carefully during the implementation of
interconnected health information systems. Secure an effective data exchange along with the protection of patients
confidentiality are two issues that electronic health records need to address to make them reliable and secured in a shared
healthcare environments. This newly developed health care system looked into these constraints by developing a web based
system for effective data exchange and encryption of the database to keep patients information secure.
Jahnke, (2005) provide a context-aware information service for healthcare systems. They introduce an ontology-based
context management system that allows a user to define contexts employing terms from the NHMS field. Their context
ontology is composed of domain independent (e.g. time and location) and domain dependent (following Health Level 7
Reference Information Model) parts. Agility is a distinctive aspect of the health care profession. Clinicians operate in a fast
changing environment with needs to access different pieces of information in different situations. On the surface it would
appear that clinicians would benefit tremendously from the use of modern mobile technology. In reality, however, the health
care sector has been hesitant to embrace electronic clinical information systems in general and mobile technologies in
particular. In this developed system, we introduce an ontology-based Context Management System that allows the user to
define contexts using terms from the medical fieldto improve the adoption of healthcareinformation..
Toninelli, (2006) presents a secure collaboration mechanism. They used Context-aware information service and semantic
modeling technologies to provide a semantic Context Aware Access Control (CAAC) framework. Semantic technologies are
used for context/policy specification to allow high-level description and reasoning as employed in this study.
Hung, (2007) provides an extended RBAC model that focuses on privacy. He investigates the privacy requirements
identified by the Health Insurance Portability and Accountability Act (HIPAA). He determines the major privacy concerns
as the:
i.
Acq
uisition, storage, and processing of data,
ii
Consent for processing and disclosure of data,
iii
Rights of subjects to access and modify their data sets.
Regarding confidentiality, integrity and availability requirements of patient data, a major concern is to avoid disclosure of
these data to unqualified users. Access by unauthorized users to patient data may result in misdiagnosis, delays in treatment,
or mistreatment. Other consequences may include financial problems such as denial of insurance coverage and loss of job
opportunities (Hung, 2007).
Hung, (2007) discusses issues in developing a privacy access control model for supporting mobile and ad hoc healthcare
applications. They developed their model, considering privacy rules for Protected Health Informatics (i.e. limitation on
collection, disclosure, use, and retention) and mobility. They used a policy specification language such as Ponder and Rei to
implement their model. However, their method did not bridge the gaps that exist within heterogeneous and homogeneous
systems that is addressed / embraced by this study which the developed system covers
Hafner, (2008) identify a number of use cases in the healthcare domain such as dynamic access control, delegation, break
glass, 4-eyes-principle, and usage control. They used specialized SELECT-Framework for model driven security for the
healthcare domain based on UCON (a security policy model for usage control). They use unified modeling language (UML)
and object constraint language (OCL) to express constraints and relations.
III.
SYSTEM DESIGN
The constraint based access control system model for information distribution in Nigerias healthcare systems as designed,
NHMS needs to be implemented to satisfy all the requirements mentioned in the above section as well as future needs as
demanded. One of the major design principles based for the system is the extendibility. NHMS is expected to cater for all
present market requirements while having the flexibility to face changing requirements as it is being used because the
healthcare sector is a rapidly evolving industry which introduces new things to the world day by day. Initially the main
inputs and outputs are analyzed because manipulating inputs and producing the required output is the fundamental of any
system. For NHMS, there are a widerange of inputs both identified as well as unidentified. As mentioned above, the system
should have the ability to manipulate unidentified inputs as well as in the future since extendibility is enforced. Identified
inputs are shown in Table 3.1
www.ajer.org
Page 286
American Journal Of Engineering Research (AJER)
2016
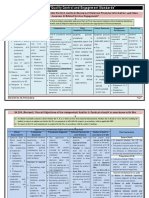
Table 3.1: Defining the Inputs Methods
3.1Database Design
Database can be identified as the heart of the system since it is the main asset for the system and should keep all data related
to NHMS. The database should be able to store all the data formats discussed and it is designed for efficient data storing and
retrieving functionality to cater for large number of users. Concurrent processing of data is required as the NHMS
information can be manipulated from anywhere simultaneously. Since the system is from remote locations via the web
service, stored procedures are used to cater for the large traffic of usage expected.
3.2 Class Diagram
A class diagram in the Unified Modeling Language (UML) is a type of static structure diagram that describes the structure
of a system by showing the system's classes, their attributes, and the relationships between the classes as shown in fig 3.2.
The class diagram is the main building block in object oriented modeling. The classes in a class diagram represent both the
main objects and or interactions in the application and the objects to be programmed. The main classes that are identified in
our system NHMS design are as follows: Assessment, Assessment Result, Categories, Patient, NHMS field, Personal Detail,
and Users.
www.ajer.org
Page 287
American Journal Of Engineering Research (AJER)
2016
IV. RESULT AND IMPLEMENTATION
<?php
classPrivilegedUserextendsUser
5.3 Privileged user Algorithm
{
private$roles;
publicfunction__construct() {
parent::__construct();
}
Fig: 4.2 Privileged user Algorithm (Source: Adaptive)
// override User method
4.1.1 Role Class
publicstaticfunctiongetByUsername($username) {
The primary focus of the Role class is to return a role object that is populated with each role corresponding permissions.
This will allow you
to easily
check whether
permission
is available
having to=perform
redundant SQL queries with
$sql=
"SELECT
* FROM
users
WHEREwithout
username
:username";
every request.
The getRolePerms()
method
creates a new Role object based on a specific role ID, and then uses a JOIN clause to combine
$sth=
$GLOBALS["DB"]->prepare($sql);
the roleperm and permdesc tables. For each permissions associated with the given role, the description is stored as the key
$sth->execute(array(":username"=>
and its value is set
to true. The hasPerm () method accepts a permission $username));
$result= $sth->fetchAll();
if(!empty($result)) {
$privUser= newPrivilegedUser();
$privUser->user_id = $result[0]["user_id"];
$privUser->username = $username;
$privUser->password = $result[0]["password"];
$privUser->email_addr = $result[0]["email_addr"];
$privUser->initRoles();
return$privUser;
} else{
description and returns the value based on the current object.
returnfalse;
4.1.2 Privileged User Class
}
}
www.ajer.org
Page 288
American Journal Of Engineering Research (AJER)
2016
By creating a new class in the NHMS Database that extends your existing user class, you can reuse your existing code
logic for managing users and then add some additional methods on top of those which are geared specifically towards
working with privileges as shown in fig 4.3
Fig 4.3: patient database structure
Login Details
Step 1-Type http://localhost/hospital/staff_info.php
Step 2-Login as Admin (Username: aliyat, Password: mummy1)
Step 3-Click on Access to login doctors profile
Step 4-Fill in information as required
Step 5-Click Insert to save information
Seedetails in figures 4.8 to 4.15:
Fig 4.8: Administrator Login
Fig4.8 Admin profile
www.ajer.org
Page 289
American Journal Of Engineering Research (AJER)
2016
Fig 4.8 above is the login screen for doctors, patient and admin. Login username and password will be created by the admin
so that they have access to edit their profiles and gained access rights toindividual dashboard(interface).
Fig 4.8.1: Output
Fig 4.8.1 display the welcome page for the administrator. This interface allow the administrator to create an access role for
the patient and the doctors. The interface also help the admin to register patients and retrieval of patients, nurses and doctors
records.
www.ajer.org
Page 290
American Journal Of Engineering Research (AJER)
2016
Fig 4.9: Doctors details
Figure 4.9 above helps to create the doctors profile and inserting it into the database for remote access. It includes the
doctor registration number, name, username, password, email and the doctors phone number
Fig 4.10 Add doctor menu;
The form was used to add the doctors full identity like genotype, weight, date of birth, blood group, address, profile
photo. It will automatically be storedand archived so that it will be access remotely by other resident doctors when
required.
DOCTORS PROFILE
www.ajer.org
Page 291
American Journal Of Engineering Research (AJER)
2016
Fig 4.11: First Doctor
The form above display the profile of the first doctor. The doctors profile can be retrieved from the archived after querying
the database. This display the summary of the doctor biography and profile for other doctors to view/access in case of
emergency
CONCLUSION
Constraint based access control model for information distribution in Nigerias healthcare system is a novel innovation that
will ensure security, confidentiality and ethical risk issues in the healthcare domain as well as improve the quality, efficiency
and effectiveness of healthcare delivery by allowing healthcare professionals to share information about their patients across
the globe. This model will hugely cut the cost of travelling for NHMS consultations, which runs into billions of dollars /
Naira especially from developing world in the face of poverty and dwindling economies of these nations.With the rapid
development of technology in the healthcare sector, collaboration and integration of healthcare systemsare required to help
management in administrative activities; provide information in healthcare services and also, reveals that the majority of
patients are willing to use newtechnologies to deal with healthcare services.
REFRENCE
[1.]
[2.]
[3.]
[4.]
[5.]
[6.]
[7.]
[8.]
[9.]
Blobe
l., B, Karla., D, Marc., K, Lunn., K, Pharow., P, Ruptsalian., N, Blobel., B. (2004). Authorization and access control for electronic health record
systems. International Journal of NHMS Informatics, Vol. 73, Issue 6, pp251-257.
Chan
dramouli, R (2001). A framework for multiple authorization types in a healthcare application system. In Proceedings of the 17th Annual Computer
Security Applications Conference, pages 137-148.
Hafner, M (2008). Models in software engineering: modeling and enforcing advanced access control policies in healthcare systems. International
Journal of Computer Intelligence. Vol. 5, issue 2, pages 132-144.
Hung, P.C.K (2007). Research issues of privacy access control model for mobile ad-hoc healthcare applications with xacml. Advanced
Information Networking and Applications Workshops, pp582-587.
Jahnke, J.H (2005) Toward context-aware computing in clinical care. In OOPSLA Workshop on Building Software for Pervasive Computing.
United State
Olutola .M. O and Oloruntoba .S. O, (2009). An information Databank Framework for the Health care Industry in Nigeria, International Journal of
Computing and ICT Research, Vol. 3, No. 2.
Perry, B., and Gesler, W. (2000). Physical Access to Primary Health Care in Andean Boliva. Soc.Sci. American Journal of Scientific Research.
Vol. 50, Issue7, pp1177-1188.
Tonin
elli, A (2006), A semantic context-aware access control framework for secure collaborations in pervasive computing environments. In ISWC '06:
Fifth International Semantic Web Conference, pages 473-486.
Verha
nneman, T (2003) Distributed applications and interoperable systems volume 2893 of Lecture Notes in Computer Science, chapter Adaptable
Access Control Policies for NHMS Information Systems, pages 133-140.
www.ajer.org
Page 292
Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- ISM Powerpoint GeneralDokument96 SeitenISM Powerpoint Generaltejmayer100% (14)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Data Center Physical Security Best Practices Checklist PDFDokument3 SeitenData Center Physical Security Best Practices Checklist PDFaL DoomNoch keine Bewertungen
- Brother hl-2140, hl-2150n, hl-2170w Service ManualDokument174 SeitenBrother hl-2140, hl-2150n, hl-2170w Service ManualAdi Popa100% (1)
- 2021 Asset Management and Maintenance Priorities Survey ReportDokument29 Seiten2021 Asset Management and Maintenance Priorities Survey ReportShashannk DoshiNoch keine Bewertungen
- Quarry Design HandbookDokument160 SeitenQuarry Design Handbookalidoon50% (2)
- Def-Stan00-35pt2iss4 Trial Prog Derivation and AssessmentDokument101 SeitenDef-Stan00-35pt2iss4 Trial Prog Derivation and AssessmentBahadır HarmancıNoch keine Bewertungen
- The Business Case For A Next Generation SIEMDokument11 SeitenThe Business Case For A Next Generation SIEMGheorghica AndreeaNoch keine Bewertungen
- The Differentiation Between The Turbulence and Two-Phase Models To Characterize A Diesel Spray at High Injection PressureDokument7 SeitenThe Differentiation Between The Turbulence and Two-Phase Models To Characterize A Diesel Spray at High Injection PressureAJER JOURNALNoch keine Bewertungen
- A Concept of Input-Output Oriented Super-Efficiency in Decision Making Units.Dokument6 SeitenA Concept of Input-Output Oriented Super-Efficiency in Decision Making Units.AJER JOURNALNoch keine Bewertungen
- Pixel Based Off-Line Signature Verification SystemDokument6 SeitenPixel Based Off-Line Signature Verification SystemAJER JOURNALNoch keine Bewertungen
- Performance Analysis of LTE in Rich Multipath Environments Considering The Combined Effect of Different Download Scheduling Schemes and Transmission ModesDokument6 SeitenPerformance Analysis of LTE in Rich Multipath Environments Considering The Combined Effect of Different Download Scheduling Schemes and Transmission ModesAJER JOURNALNoch keine Bewertungen
- The Role of Citizen Participant in Urban Management (Case Study: Aligudarz City)Dokument6 SeitenThe Role of Citizen Participant in Urban Management (Case Study: Aligudarz City)AJER JOURNALNoch keine Bewertungen
- Improved RSA Cryptosystem Based On The Study of Number Theory and Public Key CryptosystemsDokument7 SeitenImproved RSA Cryptosystem Based On The Study of Number Theory and Public Key CryptosystemsAJER JOURNALNoch keine Bewertungen
- Comparative Analysis of Cell Phone Sound Insulation and Its Effects On Ear SystemDokument6 SeitenComparative Analysis of Cell Phone Sound Insulation and Its Effects On Ear SystemAJER JOURNALNoch keine Bewertungen
- Experimental Investigation On The Effects of Digester Size On Biogas Production From Cow DungDokument6 SeitenExperimental Investigation On The Effects of Digester Size On Biogas Production From Cow DungAJER JOURNALNoch keine Bewertungen
- An Evaluation of Skilled Labour Shortage in Selected Construction Firms in Edo State, NigeriaDokument12 SeitenAn Evaluation of Skilled Labour Shortage in Selected Construction Firms in Edo State, NigeriaAJER JOURNALNoch keine Bewertungen
- Production and Comparartive Study of Pellets From Maize Cobs and Groundnut Shell As Fuels For Domestic Use.Dokument6 SeitenProduction and Comparartive Study of Pellets From Maize Cobs and Groundnut Shell As Fuels For Domestic Use.AJER JOURNALNoch keine Bewertungen
- Switching of Security Lighting System Using Gsm.Dokument12 SeitenSwitching of Security Lighting System Using Gsm.AJER JOURNALNoch keine Bewertungen
- Unmanned Aerial Vehicle and Geospatial Technology Pushing The Limits of DevelopmentDokument6 SeitenUnmanned Aerial Vehicle and Geospatial Technology Pushing The Limits of DevelopmentAJER JOURNALNoch keine Bewertungen
- Structure and Surface Characterization of Nanostructured Tio2 Coatings Deposited Via HVOF Thermal Spray ProcessesDokument9 SeitenStructure and Surface Characterization of Nanostructured Tio2 Coatings Deposited Via HVOF Thermal Spray ProcessesAJER JOURNALNoch keine Bewertungen
- Recycling of Scrapped Mating Rings of Mechanical Face SealsDokument5 SeitenRecycling of Scrapped Mating Rings of Mechanical Face SealsAJER JOURNALNoch keine Bewertungen
- Experimental Evaluation of Aerodynamics Characteristics of A Baseline AirfoilDokument6 SeitenExperimental Evaluation of Aerodynamics Characteristics of A Baseline AirfoilAJER JOURNALNoch keine Bewertungen
- Minimizing Household Electricity Theft in Nigeria Using GSM Based Prepaid MeterDokument11 SeitenMinimizing Household Electricity Theft in Nigeria Using GSM Based Prepaid MeterAJER JOURNALNoch keine Bewertungen
- Utilization of "Marble Slurry" in Cement Concrete Replacing Fine AgreegateDokument4 SeitenUtilization of "Marble Slurry" in Cement Concrete Replacing Fine AgreegateAJER JOURNALNoch keine Bewertungen
- Weighted Denoising With Multi-Spectral Decomposition For Image CompressionDokument13 SeitenWeighted Denoising With Multi-Spectral Decomposition For Image CompressionAJER JOURNALNoch keine Bewertungen
- Distinct Revocable Data Hiding in Ciphered ImageDokument7 SeitenDistinct Revocable Data Hiding in Ciphered ImageAJER JOURNALNoch keine Bewertungen
- Urbanization and The Risk of Flooding in The Congo Case of The City of BrazzavilleDokument6 SeitenUrbanization and The Risk of Flooding in The Congo Case of The City of BrazzavilleAJER JOURNALNoch keine Bewertungen
- WHY JESUS CHRIST CAME INTO THE WORLD?... (A New Theory On "TIE MINISTRY")Dokument12 SeitenWHY JESUS CHRIST CAME INTO THE WORLD?... (A New Theory On "TIE MINISTRY")AJER JOURNALNoch keine Bewertungen
- Statistical Method of Estimating Nigerian Hydrocarbon ReservesDokument10 SeitenStatistical Method of Estimating Nigerian Hydrocarbon ReservesAJER JOURNALNoch keine Bewertungen
- Eye State Detection Using Image Processing TechniqueDokument6 SeitenEye State Detection Using Image Processing TechniqueAJER JOURNALNoch keine Bewertungen
- DMP Packet Scheduling For Wireless Sensor NetworkDokument8 SeitenDMP Packet Scheduling For Wireless Sensor NetworkAJER JOURNALNoch keine Bewertungen
- An Exponent-Based Propagation Path Loss Model For Wireless System Networks at Vehicular SpeedDokument12 SeitenAn Exponent-Based Propagation Path Loss Model For Wireless System Networks at Vehicular SpeedAJER JOURNALNoch keine Bewertungen
- Theoretical and Experimental Study of Cavitation Dispersing in "Liquid-Solid" System For Revelation of Optimum Influence ModesDokument10 SeitenTheoretical and Experimental Study of Cavitation Dispersing in "Liquid-Solid" System For Revelation of Optimum Influence ModesAJER JOURNALNoch keine Bewertungen
- The Design and Implementation of A Workshop Reservation SystemDokument7 SeitenThe Design and Implementation of A Workshop Reservation SystemAJER JOURNALNoch keine Bewertungen
- Head Determination and Pump Selection For A Water Treatment Plant in Villages Around Maiduguri, Borno State, NigeriaDokument5 SeitenHead Determination and Pump Selection For A Water Treatment Plant in Villages Around Maiduguri, Borno State, NigeriaAJER JOURNALNoch keine Bewertungen
- Frequency Selective Fading in Wireless Communication Using Genetic AlgorithmDokument6 SeitenFrequency Selective Fading in Wireless Communication Using Genetic AlgorithmAJER JOURNALNoch keine Bewertungen
- Risk Assessment and Risk MappingDokument7 SeitenRisk Assessment and Risk MappingAJER JOURNALNoch keine Bewertungen
- AD EHSMS RF - V2 0 - Standard PresentationDokument79 SeitenAD EHSMS RF - V2 0 - Standard Presentationasimnaqvi2008Noch keine Bewertungen
- Tripwire CCM Policies and Platform Support 2015Q4 DatasheetDokument12 SeitenTripwire CCM Policies and Platform Support 2015Q4 DatasheetSteve BundeNoch keine Bewertungen
- Installation/Operating Manual: Submersible Borehole PumpDokument88 SeitenInstallation/Operating Manual: Submersible Borehole PumpMarco BustosNoch keine Bewertungen
- Com - Opera.mini - Native.operafileo File:///storage/emulated/0/download/manual Rps 450 GB Vec626r0 PDFDokument86 SeitenCom - Opera.mini - Native.operafileo File:///storage/emulated/0/download/manual Rps 450 GB Vec626r0 PDFMamadou djibril BaNoch keine Bewertungen
- Corporate Governance in Bangladesh: Evidence of ComplianceDokument22 SeitenCorporate Governance in Bangladesh: Evidence of ComplianceMehrab Jami Aumit 1812818630Noch keine Bewertungen
- Executive Summary Impact Assessment EMFA eCPL8l5LECc21EAEChijuNp0 89594Dokument4 SeitenExecutive Summary Impact Assessment EMFA eCPL8l5LECc21EAEChijuNp0 89594Fernando Rivera LazoNoch keine Bewertungen
- Resources AssetDokument17 SeitenResources AssetCarolineNoch keine Bewertungen
- USA Vs AnthemDokument112 SeitenUSA Vs AnthemAshleeNoch keine Bewertungen
- Entity Terder Committees Tender Committee For Central Management Agency/Ministry/Subvented AgencyDokument17 SeitenEntity Terder Committees Tender Committee For Central Management Agency/Ministry/Subvented AgencyjovahsonNoch keine Bewertungen
- Feiya Engineering and Trading Com - LTDDokument4 SeitenFeiya Engineering and Trading Com - LTDKwaku DuahNoch keine Bewertungen
- Third Report by Court-Appointed Independent Monitor On The Status of The NYC Department of Correction, April 3, 2017Dokument256 SeitenThird Report by Court-Appointed Independent Monitor On The Status of The NYC Department of Correction, April 3, 2017DNAinfoNewYorkNoch keine Bewertungen
- 5887 Site PrepDokument118 Seiten5887 Site PrepLeeNoch keine Bewertungen
- Intertek - IEC 62368-1 Standard Compliance Guide White Paper - 2019.04Dokument11 SeitenIntertek - IEC 62368-1 Standard Compliance Guide White Paper - 2019.04Kajal MukherjeeNoch keine Bewertungen
- Tenaris Sustainability Report 2017Dokument52 SeitenTenaris Sustainability Report 2017hasdNoch keine Bewertungen
- Framework of INTOSAI Government Auditing StandardsDokument21 SeitenFramework of INTOSAI Government Auditing StandardssukandeNoch keine Bewertungen
- Az 900Dokument10 SeitenAz 900Abhishek PubbisettyNoch keine Bewertungen
- Sa Question Bank by Kapil Goyal Sir PDFDokument55 SeitenSa Question Bank by Kapil Goyal Sir PDFManoj VenkatNoch keine Bewertungen
- 1937481554-BRS Presicion Manufacturin PVT LTD ReportDokument15 Seiten1937481554-BRS Presicion Manufacturin PVT LTD Reportlingadevaru13Noch keine Bewertungen
- Roles and responsibilities of ICT functionsDokument20 SeitenRoles and responsibilities of ICT functionsManjur AlamNoch keine Bewertungen
- DoD Suspicious Activity Reporting PolicyDokument17 SeitenDoD Suspicious Activity Reporting PolicydorinkarakogluNoch keine Bewertungen
- Connection of Roof Battens To Timber Rafters in Light Weight Metal Roof Sheet ConstructionDokument3 SeitenConnection of Roof Battens To Timber Rafters in Light Weight Metal Roof Sheet ConstructionAnthony LeilyNoch keine Bewertungen
- SA 'S ChartsDokument46 SeitenSA 'S ChartsBharath Kumar100% (1)
- Solar Installers Safety ChecklistDokument3 SeitenSolar Installers Safety ChecklistOubahsis NissrineNoch keine Bewertungen