Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Zirk and Poetzschke2004On The Suitability of Refractometry For The Analysis of Glucose in Blood-Derived FluidsDokument9 SeitenZirk and Poetzschke2004On The Suitability of Refractometry For The Analysis of Glucose in Blood-Derived FluidsPWaaaaNoch keine Bewertungen
- Blood Banking and SerologyDokument9 SeitenBlood Banking and SerologyMiaNoch keine Bewertungen
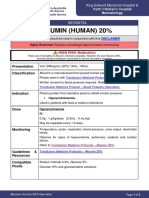
- Albumin 20 Per CentDokument3 SeitenAlbumin 20 Per CentidaNoch keine Bewertungen
- Wbi11 01 2024 Jan QPNDokument28 SeitenWbi11 01 2024 Jan QPNfreemanNoch keine Bewertungen
- Mordheim - NosferatuDokument13 SeitenMordheim - Nosferatucyloss23100% (2)
- Episode 10Dokument18 SeitenEpisode 10Pang Chixx90% (31)
- Learning Module For Science 9 First Quarter: Camarines Norte College IncDokument24 SeitenLearning Module For Science 9 First Quarter: Camarines Norte College IncCrisanto VelascoNoch keine Bewertungen
- Food PyramidDokument12 SeitenFood PyramidAgnes Enya LorraineNoch keine Bewertungen
- Drug StudyDokument2 SeitenDrug StudyAjay SupanNoch keine Bewertungen
- Duran, Fatima Medriza - MS ModulesDokument130 SeitenDuran, Fatima Medriza - MS Modulesnot your medz duranNoch keine Bewertungen
- Erba Actime - APTTDokument2 SeitenErba Actime - APTTthinh.ho2Noch keine Bewertungen
- Cardiopulmonary Resuscitation (CPR)Dokument26 SeitenCardiopulmonary Resuscitation (CPR)Serrano, John DanielleNoch keine Bewertungen
- Ustet ReviewerDokument16 SeitenUstet ReviewerVinzynt Isler Carmona100% (19)
- Alkalife Reverse Aging Handbook Sang Whang WebDokument24 SeitenAlkalife Reverse Aging Handbook Sang Whang Weblab337100% (4)
- Level - 1 I. Fill in The BlanksDokument5 SeitenLevel - 1 I. Fill in The BlanksKesanam SpNoch keine Bewertungen
- NCP On Postpartum MotherDokument9 SeitenNCP On Postpartum MotherM.S.H Tube100% (1)
- NUR 102 - Human Anatomy and Physiology Rev. 001Dokument12 SeitenNUR 102 - Human Anatomy and Physiology Rev. 001Alan0% (2)
- Heparin Protocol For DVT PEDokument3 SeitenHeparin Protocol For DVT PEhorzhanNoch keine Bewertungen
- LDTDokument6 SeitenLDTRaian SuyuNoch keine Bewertungen
- Home Based CareDokument34 SeitenHome Based CaremewselectionsNoch keine Bewertungen
- BSC Hons Zoology 2016-17 - 23 - 7 - 18Dokument45 SeitenBSC Hons Zoology 2016-17 - 23 - 7 - 18DHUVADU JAGANATHAMNoch keine Bewertungen
- Free Nclex QuestionsDokument161 SeitenFree Nclex QuestionspadmaNoch keine Bewertungen
- ELSci Q2 Lesson 5 - Metabolic Processes Among Living ThingsDokument51 SeitenELSci Q2 Lesson 5 - Metabolic Processes Among Living ThingsItsClarenceNoch keine Bewertungen
- Walter Cannon - Traumatic ShockDokument10 SeitenWalter Cannon - Traumatic ShockMarina de CarneriNoch keine Bewertungen
- Biology Checkpoint Topics Part 1Dokument36 SeitenBiology Checkpoint Topics Part 1esteban ferrada silvaNoch keine Bewertungen
- Over View of BloodDokument42 SeitenOver View of BloodJenadi BinartoNoch keine Bewertungen
- Abnormal Bleeding IN Children: DR Barnabas Atwiine Paediatric Haematologist and Oncologist MustDokument48 SeitenAbnormal Bleeding IN Children: DR Barnabas Atwiine Paediatric Haematologist and Oncologist MustSsenyonga DominicNoch keine Bewertungen
- Group SummaryDokument4 SeitenGroup Summaryapi-482732223Noch keine Bewertungen
- Brain Damaging Habits: 1. No BreakfastDokument8 SeitenBrain Damaging Habits: 1. No BreakfastSAKTHIVEL A100% (1)
- Science 6 Reviewer For Quiz BeeDokument2 SeitenScience 6 Reviewer For Quiz BeeNovabelle Pandoy100% (6)