Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Module 14 Pediatric TB ENGLISHDokument85 SeitenModule 14 Pediatric TB ENGLISHDellNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Family Planning HandbookDokument387 SeitenFamily Planning HandbookvthiseasNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Jurnal Farmakologi Anti Konvulsi PDFDokument13 SeitenJurnal Farmakologi Anti Konvulsi PDFtherempongss100% (1)
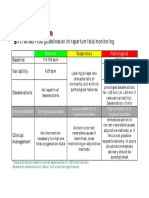
- CTG Classification PDFDokument1 SeiteCTG Classification PDFDellNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- 5 Morisky Medication Adherence-Scale PDFDokument1 Seite5 Morisky Medication Adherence-Scale PDFDellNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- A Practical Classification of Septonasal Deviation.42Dokument3 SeitenA Practical Classification of Septonasal Deviation.42DellNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- SPSS Crosstab PDFDokument3 SeitenSPSS Crosstab PDFDellNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Appendix 8 Normal Urine Output PDFDokument1 SeiteAppendix 8 Normal Urine Output PDFDellNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- 5 Morisky Medication Adherence-Scale PDFDokument1 Seite5 Morisky Medication Adherence-Scale PDFDellNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Fitzpatrick's Dermatology in General Medicine, Eighth Edition, 2 Volume SetDokument30 SeitenFitzpatrick's Dermatology in General Medicine, Eighth Edition, 2 Volume SetDellNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Cutaneous Tuberculosis: Epidemiologic, Etiopathogenic and Clinical Aspects - Part IDokument10 SeitenCutaneous Tuberculosis: Epidemiologic, Etiopathogenic and Clinical Aspects - Part IDellNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- UT Dallas Syllabus For Govt4396.002.08s Taught by Gregory Thielemann (Gregt)Dokument2 SeitenUT Dallas Syllabus For Govt4396.002.08s Taught by Gregory Thielemann (Gregt)UT Dallas Provost's Technology GroupNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- JIS G 3141: Cold-Reduced Carbon Steel Sheet and StripDokument6 SeitenJIS G 3141: Cold-Reduced Carbon Steel Sheet and StripHari0% (2)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Performance Monitoring and Coaching FormDokument3 SeitenPerformance Monitoring and Coaching Formjanine masilang100% (2)
- What's New in CAESAR II: Piping and Equipment CodesDokument1 SeiteWhat's New in CAESAR II: Piping and Equipment CodeslnacerNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Umwd 06516 XD PDFDokument3 SeitenUmwd 06516 XD PDFceca89Noch keine Bewertungen
- Bolt Grade Markings and Strength ChartDokument2 SeitenBolt Grade Markings and Strength ChartGregory GaschteffNoch keine Bewertungen
- Global Divides: The North and The South: National University Sports AcademyDokument32 SeitenGlobal Divides: The North and The South: National University Sports AcademyYassi CurtisNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- MultiLoadII Mobile Quick Start PDFDokument10 SeitenMultiLoadII Mobile Quick Start PDFAndrés ColmenaresNoch keine Bewertungen
- Sociology As A Form of Consciousness - 20231206 - 013840 - 0000Dokument4 SeitenSociology As A Form of Consciousness - 20231206 - 013840 - 0000Gargi sharmaNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Tutorial 5 SolvedDokument3 SeitenTutorial 5 SolvedAshutoshKumarNoch keine Bewertungen
- Music 10 (2nd Quarter)Dokument8 SeitenMusic 10 (2nd Quarter)Dafchen Villarin MahasolNoch keine Bewertungen
- 6GK74435DX040XE0 Datasheet enDokument3 Seiten6GK74435DX040XE0 Datasheet enLuis CortezNoch keine Bewertungen
- Interlocking Block TechnologyDokument15 SeitenInterlocking Block TechnologyChaula Trivedi100% (5)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Algoritm BackTracking EnglezaDokument6 SeitenAlgoritm BackTracking Englezaionutz_67Noch keine Bewertungen
- WAQF Podium Design Presentation 16 April 2018Dokument23 SeitenWAQF Podium Design Presentation 16 April 2018hoodqy99Noch keine Bewertungen
- MCI Approved Medical College in Uzbekistan PDFDokument3 SeitenMCI Approved Medical College in Uzbekistan PDFMBBS ABROADNoch keine Bewertungen
- Sem4 Complete FileDokument42 SeitenSem4 Complete Fileghufra baqiNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Case CapsuleDokument8 SeitenCase CapsuleLiza BulsaraNoch keine Bewertungen
- Contents EEMUA Publication 190 Edition1 May 2015Dokument4 SeitenContents EEMUA Publication 190 Edition1 May 2015Aditya JainNoch keine Bewertungen
- Eggermont 2019 ABRDokument15 SeitenEggermont 2019 ABRSujeet PathakNoch keine Bewertungen
- 2022 WR Extended VersionDokument71 Seiten2022 WR Extended Versionpavankawade63Noch keine Bewertungen
- Eloy-Stock English Full PDFDokument0 SeitenEloy-Stock English Full PDFR.s. WartsNoch keine Bewertungen
- Design of Penstock: Reference Code:IS 11639 (Part 2)Dokument4 SeitenDesign of Penstock: Reference Code:IS 11639 (Part 2)sunchitk100% (3)
- NCP - Major Depressive DisorderDokument7 SeitenNCP - Major Depressive DisorderJaylord Verazon100% (1)
- Lesson 6 - Vibration ControlDokument62 SeitenLesson 6 - Vibration ControlIzzat IkramNoch keine Bewertungen
- Technology Based Project: Special Track 1)Dokument14 SeitenTechnology Based Project: Special Track 1)Kim ChiquilloNoch keine Bewertungen
- Sample - SOFTWARE REQUIREMENT SPECIFICATIONDokument20 SeitenSample - SOFTWARE REQUIREMENT SPECIFICATIONMandula AbeyrathnaNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Week 4 - Theoretical Framework - LectureDokument13 SeitenWeek 4 - Theoretical Framework - LectureRayan Al-ShibliNoch keine Bewertungen
- Hướng Dẫn Chấm: Ngày thi: 27 tháng 7 năm 2019 Thời gian làm bài: 180 phút (không kể thời gian giao đề) HDC gồm có 4 trangDokument4 SeitenHướng Dẫn Chấm: Ngày thi: 27 tháng 7 năm 2019 Thời gian làm bài: 180 phút (không kể thời gian giao đề) HDC gồm có 4 trangHưng Quân VõNoch keine Bewertungen
- Case Study 2Dokument5 SeitenCase Study 2api-247285537100% (1)